


1Adult Psychiatry A and Medical Psychology Department and 8Dermatology Department, CHU Clermont-Ferrand, Clermont Auvergne University, 2Adult Psychiatry A and Medical Psychology Department and 7Clinical Research and Innovation Department, CHU Clermont-Ferrand, Clermont-Ferrand, 3Psychiatry Department, CHU St-Etienne, University Jean Monnet, St-Etienne, 4Psychiatric Emergencies, Esquirol Hospital, Limoges, 5University Hospital of Psychiatry and Psychotherapy, Laxou, 6Dermatology Department, CHU Nord Hospital, Saint-Etienne, France
Psychiatric and personality disorders have been extensively documented in patients with systemic lupus ery-thematosus (SLE). However, the prevalence of personality disorders in skin-restricted lupus (SRL) patients remains unknown. The aim of this study was to assess the prevalence of personality disorders in SRL outpatients and to examine the associated factors. We evaluated 60 SRL outpatients and 118 controls matched for sex, age and education level. On the basis of the Personality Diagnostic Questionnaire 4+, 38% of patients vs 20% of controls fulfilled the criteria for at least one personality disorder (OR 2.2 [95% CI 1.01–4.6], p = 0.048). Only one patient with a personality disorder had specialised mental health care. Late lupus onset and more frequent past treatments by thalidomide were associated factors. This study evidences a high prevalence of personality disorders in SRL patients and shows that most SRL patients with personality disorder do not receive specialised mental health care.
Key words: skin-restricted lupus; personality disorders; PDQ4+; LuPsy cohort.
Accepted Apr 27, 2017; Epub ahead of print Apr 27, 2017
Acta Derm Venereol 2017
Corr: Prof Isabelle Jalenques, Adult Psychiatry A and Medical Psychology Department, CHU Clermont-Ferrand, 58 rue Montalembert, FR-63003 Clermont-Ferrand Cedex 1, France. E-mail: ijalenques@chu-clermontferrand.fr
Psychiatric and personality disorders (PD) have been reported in patients with systemic lupus erythematosus (SLE) (1–4). Although skin-restricted lupus erythematosus (SRL), which comprises discoid lupus erythematosus (DLE), lupus tumidus (LT) and subacute cutaneous lupus erythematosus (SCLE), is as common as SLE (5) its relation with psychiatric disorders and PDs has only exceptionally been explored. We recently evidenced a high prevalence of several psychiatric disorders (anxiety, depression, suicide risk and alcohol dependence) among SRL patients (6). Another study reported that about 35% of cutaneous lupus erythematosus patients met criteria for depression and/or anxiety (7). In an exploratory study, our group observed that 50% of 20 patients with SCLE and DLE had at least one PD, in particular obsessive-compulsive and depressive PD (8). However, this study had several limitations. First, the patient sample was small. Second, patients were prospectively recruited but on a voluntary basis and hence, although more than 30% of those interviewed agreed to participate, it can be assumed that the sample was not truly representative of SRL patients because enriched by patients beset by feelings of sadness. Finally, there was no comparison with a control group. We therefore decided to conduct a prospective study to systematically assess the prevalence of PDs among SRL patients recruited in dermatological outpatient clinics. Our secondary objectives were to examine the co-occurring Axis I psychiatric disorders and to investigate the factors associated with PD in SRL patients.
The study received approval from the regional Ethical Review Board (Comité de Protection des Personnes Sud-Est 6, ref. 2008-A00343-52/AU740, 18 June 2009). The aims and procedures were explained to participants, who all gave written informed consent.
From June 2009 to June 2012, outpatients with SRL aged 18 years or older were consecutively recruited in 8 French university hospitals. Inclusion criteria were designed to select patients with indisputable chronic or sub-acute lupus restricted to the skin and to exclude those having systemic lupus with cutaneous symptoms (see Jalenques et al. (6). Patients were either newly diagnosed or already undergoing lupus treatment. After recruitment, they were evaluated on the same day by a dermatologist and a trained psychiatrist.
Control subjects were recruited through a poster campaign and corporate intranet among volunteers from a clinical research centre, workers in public hospitals and the national railway company, and administrative personnel of the state education system. All individuals who had symptoms that could be related to a past or present lupus (systemic or cutaneous) were excluded. Two control subjects were matched with each patient for age (± 5 years), sex and education level (equivalent diploma). Controls underwent a medical examination and the same psychiatric evaluation as the patients.
We collected data concerning sex, age at visit, education level, smoking and medical history. Lupus history comprised date of first symptoms, ongoing and past specific treatments and smoking habits. Clinical examination established the number and location of lesions with mention of those on visible areas of the body. Pictures of the lesions were taken in each patient. Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) (9) score was calculated for patients at inclusion when possible.
Personality disorders were investigated by the latest version of the Personality Diagnostic Questionnaire 4+ (PDQ-4+), designed by Hyler in 1994 (10). We used the French version, validated by Bouvard & Cosma (11) in a non-clinical population and by Laconi et al. (12) in a clinical population. The PDQ-4+ consists of a 99-item self-report questionnaire requiring a first-person True or False response. PDQ-4+ explores the 12 DSM-IV personality disorders: paranoid, schizoid, schizotypal (cluster A), antisocial, borderline, histrionic, narcissistic (cluster B), avoidant, dependent, obsessive-compulsive (cluster C), depressive and passive-aggressive (negativistic) personalities. Some items detect individuals who wish to give too good an image of themselves (“too good”) and others detect “suspect” respondents (liars). The latter were excluded from the study. Remaining items correspond directly to a personality disorder. A True answer always indicates that the item should be considered and counted as pathological. For each PD, diagnosis of the disorder can be suggested when there is the required number of criteria. If one PD is detected, the psychiatrist who also investigated the axe I psychiatric disorders has to confirm or rule out the diagnosis on the basis of the clinical significance scale (CSS) of the PDQ-4+, which is an individual directive interview. This interview verifies if: there was no mistake in the answers to all positive questions; the traits have been present since age 18, or at least over the last few years; the traits are not due primarily to axis I disorders, such as anxiety or mood disorder, alcohol or drug abuse, or to a medical condition; the traits lead to significant functional impairment in at least one major area (family, social, professional) or to personal distress.
The PDQ-4+ allows the calculation of an overall score corresponding to the total sum of the pathological responses. Its total score is used as an index of overall personality disturbance with scores under 20 ruling out PD, those between 20 and 30 requiring further assessment and those > 30 indicating probable PD diagnosis (13).
Possible co-occurring axis I psychiatric disorders were investigated by the Mini International Neuropsychiatric Interview (MINI 5.0.0) (14). This structured psychiatric interview has been validated in French (15, 16) in the general population and was used for standardized evaluation of 16 current Axis I psychiatric disorders as defined by the DSM-IV.
Results were expressed as mean ± standard deviation (or median [interquartile range]) and as frequencies (%).
In univariate analyses, the primary and secondary objectives were assessed by comparing PDs in patients and controls and searching for associated factors by the χ2 test (or Fisher’s exact test when appropriate) for categorical and binary data and the Student’s t test (or Mann-Whitney’s U test if normality rejected by the Shapiro Wilk’s test) for continuous data.
Multivariate analysis was performed with a logistic regression model adjusted for age, sex, educational level, smoking status, presence of psychiatric disorder and groups (patient or control) for the primary objective. For the secondary objectives, a logistic regression model was performed using backward selection, adjusted for clinically and statistically significant factors. Results are expressed as adjusted odds ratio and their 95% confidence interval (CI).
Statistics were computed with STATA V12 (Stata Corp, College Station, Texas, USA). All p-values were two-sided and a p-value < 0.05 was considered statistically significant.
Eighty patients were recruited, of whom 7 had non-assessable data, 12 did not undergo the CSS interview and 1 was a “suspect” respondent. Hence, 60 patients (47 female = 78%) were fully assessed (Fig. S1). Excluded patients presented no differences from the recruits. After a median follow-up of 44 months following inclusion, none of the patients had developed a systemic lupus, including those with positive antinuclear antibodies. One hundred and sixty controls were recruited. The data of 40 controls, matched with those of excluded patients, were omitted. In addition, one control with non-assessable data and one with a “suspect” questionnaire were excluded. Hence, the patients were compared with 118 controls.
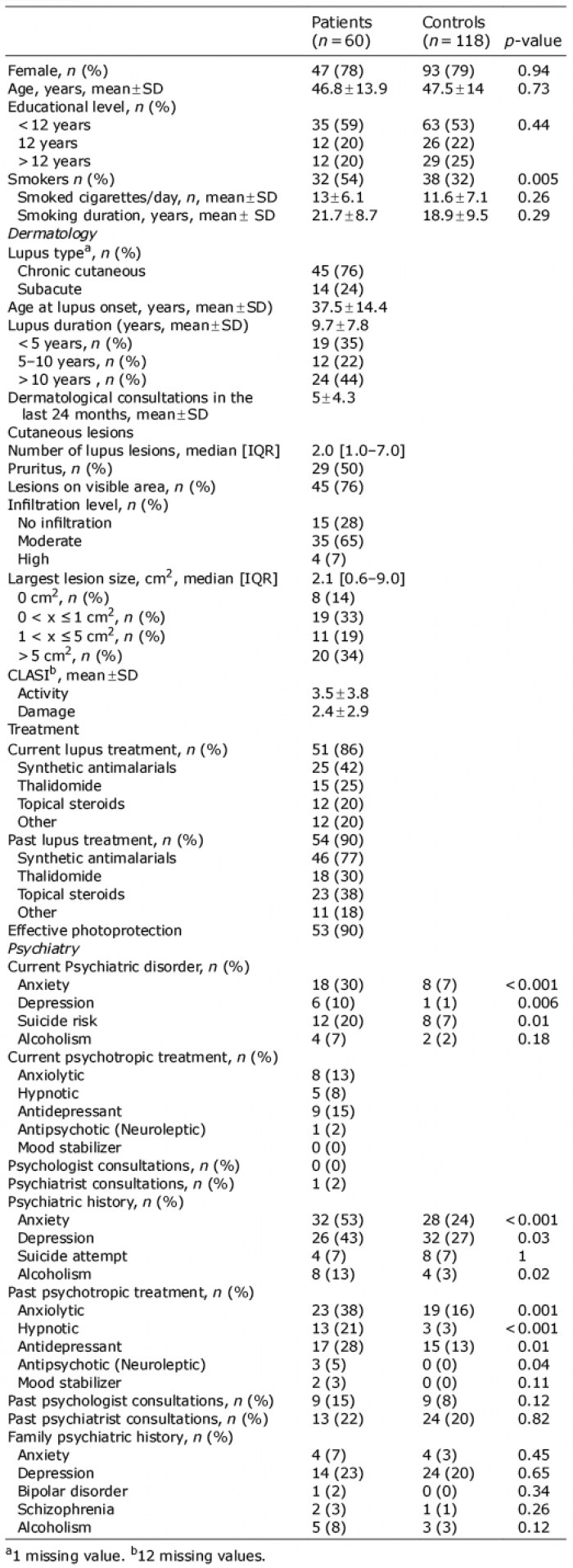
The characteristics of the participants are described in Table I. Briefly, mean patient age was 46.8 ± 13.9 years, age at first lupus symptoms was 37.5 ± 14.4 years and mean duration of disease was 9.7 ± 7.8 years; 45 (76%) patients had chronic lupus and 14 (24%) a subacute form.
Table I. Patient and control characteristics
CLASI activity and damage scores were recorded in 48 patients. Forty-five patients (76%) had lesions on a visible area of the body (Table I). Fifty one patients (86%) were receiving treatment for lupus (anti-malarial treatment in 42%, thalidomide in 25% and topical steroids in 20%).
As previously reported (6), more patients were smokers (54% vs 32%, p = 0.005) and they had more current Axis I psychiatric disorders (OR 2.4 [95% CI 1.2–4.8], p = 0.01).
The patients’ PDQ4+ score was significantly higher than that of controls (20.4 vs 16.1, p = 0.02), with no difference in score distribution according to the index of overall personality disturbance (Table II and Fig. 1). The scores showed that 23 patients (38%) vs 24 controls (20%) fulfilled the criteria for at least one personality disorder (OR 2.2 [95% CI 1.01–4.63], p = 0.048).
Table II. Personality disorder prevalence
Fig. 1. Personality Diagnostic Questionnaire 4+ (PDQ 4+) score distribution. One circle represents the PDQ4+ total score for one skin-restricted lupus patient (on left) or for one control (on right). A black line represents the mean value of PDQ4+ total score: 20.4 for patients as against 16.1 for controls. The difference is significant (p = 0.02). Total score is used as an index of overall personality disturbance, with scores under 20 ruling out PD, those between 20 and 30 requiring further assessment and those above 30 signalling probable PD diagnosis. These two score thresholds (20 and 30) are represented by red lines. There is no distribution difference between skin-restricted lupus patients and controls (p = 0.07).
Owing to the small population size, no significant difference was observed when each PD was compared individually. The most common PDs were disorders from Cluster C (specifically, avoidant and obsessive-compulsive) in both patients and controls. Depressive and paranoid PDs were also frequent in the two groups.
As personality disorders were frequently associated with Axis I psychiatric disorders, we investigated the proportion of patients who had this co-occurrence. Eleven patients (18%) had PDs alone and 12 (20%) had at least one co-occurring psychiatric disorder. We therefore decided to look for the most frequently associated psychiatric and personality disorders (Table SI). Fifty-two percent of patients with at least one PD also had a psychiatric disorder as against 38% of patients without PDs. Almost all PD categories were associated with psychiatric disorders. Unfortunately, because of insufficient data it was not possible to assess significant differences.
Of the 23 patients with PDs, only 1 (5%) were receiving current specialised mental health care and only 6 (26%) current psychotropic treatment (Table III). Treatments were anxiolytic (4 patients), antidepressant (4 patients), hypnotic (1 patient) and antipsychotic (1 patient).
Table III. Psychiatric care of skin restricted lupus patients with personality disorder (n = 23)
Most treatments were for patients with co-occurring Axis I psychiatric disorders: no patient without co-occurring axis I psychiatric disorder had consulted a psychiatrist and only 2 were receiving psychotropic treatment (1 anxiolytic and 1 antidepressant).
Demographic and skin characteristics of patients were examined for association with current PDs. In univariate analysis (Table SII), age, age at lupus onset, number of lupus lesions, skin lesion infiltration level and lupus past treatment by thalidomide were significantly different in patients with and without current PDs. Multivariable backward logistic regression identified sex, age at lupus onset and past thalidomide treatment as possible factors associated with PDs. Results are presented in Table IV.
Table IV. Associated risk factors of personality disorder in lupus patients
In patients with PDs, age at lupus onset was significantly higher and past treatment by thalidomide significantly more common.
This study was designed to evaluate the prevalence of PD in patients with SRL. Our patient sample was similar to skin lupus populations described elsewhere in terms of female/male ratio (80/20) and age at lupus onset (17) and, as in other reports, we found a statistically higher number of smokers among patients than among controls (18–20). As the prevalence of some personality disorders varies with sex, age and education level, we matched patients and controls for these variables. The prevalence of PDs in the general population and according to sex, as assessed by a True or False self-report questionnaire in the only documented study of this kind, was similar to that of our control population (21). Additionally, the prevalence rates of current psychiatric diagnoses estimated in our controls were similar to those reported in the French general population on the basis of DSM-IV criteria (22). Trained physicians confirmed the diagnoses of PDs in both patients and controls by the PDQ4+ with a CSS individual interview. Their awareness of the Axis I diagnosis of patients and controls made with the MINI 5.0.0 improved the diagnostic efficacy of the PDQ-4+ with CSS (23).
Our study reports, for the first time, a high prevalence of PDs among SRL patients, without any difference between chronic and subacute types. We show that SRL patients had a significantly higher prevalence of personality disorders (38%) than did the controls (20%), at rates close to those of patients with SLE (35.6%) (4). Our SRL patients had a higher risk of PDs (OR 2.1 [95% CI 1.0–4.5]), at rates close to those of patients with SLE, than the overall population (OR 3.05 [95% CI 1.37–6.78] (4)) and also in terms of sex distribution (women: OR 1.71 [95% CI 1.24–2.28] and men OR 2.60 [95% CI 1.24–4.81]) (3). SRL patients did not have a more extensive medical history than controls and there was no significant difference in co-morbidities other than that of skin and psychiatric disorders between the two groups. This supports the hypothesis that PDs observed in SRL patients are truly related to the disease itself.
The avoidant, depressive and obsessive-compulsive PDs were the 3 most prevalent in our SRL patients. The avoidant and obsessive-compulsive PDs were the two most frequent in SLE patients in the study of Uguz et al. (4). However, these authors did not study depressive PD since it was not included in the older DSM III classification that they used.
The co-occurrence of PDs and Axis I psychiatric disorders was frequent in SRL patients, which is consistent with the strong association of PDs with Axis I disorders observed in the general population (24). The most common co-occurrence, as in the general population, was cluster C PDs (avoidant and obsessive-compulsive PDs) and anxiety or depressive disorders. Unfortunately, the distribution of patients among 10 different diagnoses of PDs made it impossible to identify significant differences (25). In our SRL patients, as in the general population, PDs were observed in co-occurrence with suicidal behaviour (26–28). PDs and Axis I psychiatric disorders had high prevalence rates in SLE patients in the study of Uguz et al. (4). One publication has documented the increased co-occurrence of avoidant and obsessive-compulsive PDs and Axis I psychiatric disorders in patients with chronic idiopathic urticaria (29). Personality traits have been investigated in other skin diseases. Whereas we did not observe a correlation between SRL severity (CLASI) and PDs, some personality traits have been related to itch or induced scratching in patients with atopic dermatitis (30) and to severe pruritus in patients with psoriasis (31).
Although the prevalence of PDs was high in our SRL patients, most were not receiving specialist mental health care, irrespective of whether they had a co-occurring Axis I psychiatric disorder. Less than half of patients suffering from co-occurrence of PDs and Axis I psychiatric disorders were taking psychotropic treatment and only one was receiving specialist mental health care. These figures are much lower than those in studies on the use of specialised mental health care services for patients in the French general population suffering from psychological or psychiatric disorders, and despite the fact that the association of a somatic disease generally increases the likelihood of recourse to specialised mental health care (32, 33) and that the co-occurrence of PDs and Axis I psychiatric disorders is a factor of severity. Several PDs are suicide risk factors and most PDs can be suicide co-factors when co-occurring with Axis I psychiatric disorders, particularly depression (26–28, 34). Additionally, Morey et al. (35) demonstrated that the 6-year outcomes for patients with PDs plus major depressive disorder at the index evaluation were significantly worse than those of patients with pure major depressive disorder.
Our study is unable to explain why late onset of SRL is associated with the occurrence of PDs in SRL patients. However, our results could be useful in alerting physicians to the existence of this specific patient population. As we reported previously for SRL patients with Axis I psychiatric disorders, SRL patients with PDs had received past thalidomide treatment significantly more often (6). This could be related to a higher resistance of SRL patients with PDs to first-line treatments of SRL. PD with a medical condition may render patient management complex and uncertain (33).
Our study has certain limitations. First, those enrolled were recruited in university hospitals. However, there is no evidence suggesting that the clinical severity of SRL patients seen in a university hospital is different from that of other SRL patients. Additionally, all of our SRL patients attended outpatient clinics and none subsequently developed systemic lupus. Second, the physicians who assessed patients’ mental health were not blinded to the group (patient or control) status since 72% of patients had lesions on a visible area of the skin. Third, we cannot directly compare prevalence in our study with that of other chronic skin dermatoses or that of patients with systemic lupus. Our results nevertheless suggest that such comparative studies would be of interest.
We report, for the first time, a high prevalence of PDs in SRL patients and a high co-occurrence with Axis I psychiatric disorders. We also show that most SRL patients with PDs do not receive appropriate specialised mental health care. Yet, PDs are a cause of psychological distress, impaired global functioning, worse outcomes of co-occurring psychiatric disorders (35, 36) and excess mortality, in particular as a result of suicide (37). Additionally, PDs may complicate the management of medical treatment (33). Our results raise the necessity of screening for the presence of PD and possible associated Axis I disorders in SRL patients and referral of such patients for psychiatric evaluation and appropriate treatment.
The authors thank Consoli S for help in the preparation of the study design, the patients who participated in this study and J Watts for advice on the English version of the manuscript.
This study was supported by a grant from the French Ministry of Health (PHRC IR 2006 Jalenques, N°2008-A00343-52) and from Société Française de Dermatologie, 2010.
The LuPsy cohort investigators: F. Aubin (Université de Franche Comté, CHU Besançon, Service de Dermatologie, Besançon, France), C. Bedane (Department of dermatology, Hopital Dupuytren, Limoges, France), M. Chastaing (Unité de Psychiatrie de Liaison et Service de Dermatologie, CHU Brest, Brest, France), P. Combemale, J.P. Courbier (Hôpital d’instruction des armées Desgenettes, Lyon, France), C. Durand (Service de Psychiatrie de l’Adulte A et Psychologie médicale, CHU Clermont-Ferrand, Clermont-Ferrand, France), J.P. Grand (CHS Le Valmont, Urgences et Psychiatrie de Liaison, Hôpital Général de Valence, Valence, France), E. Haffen (Department of clinical psychiatry, INSERM, university hospital of Besançon, Besançon, France), L. Misery (University Hospital of Brest, Department of Dermatology and University of Western Brittany, Laboratory of Neurosciences of Brest, Brest, France), F. Skowron (Service de dermatologie, CH de Valence, Valence, France), A. Sparsa (Department of dermatology, Hopital Dupuytren, Limoges, France), G. Theilhol (Service de Psychiatrie de l’Adulte A et Psychologie médicale, CHU Clermont-Ferrand, Clermont-Ferrand, France), J. Waton (Service de dermatologie, CHU de Nancy, Nancy, France).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize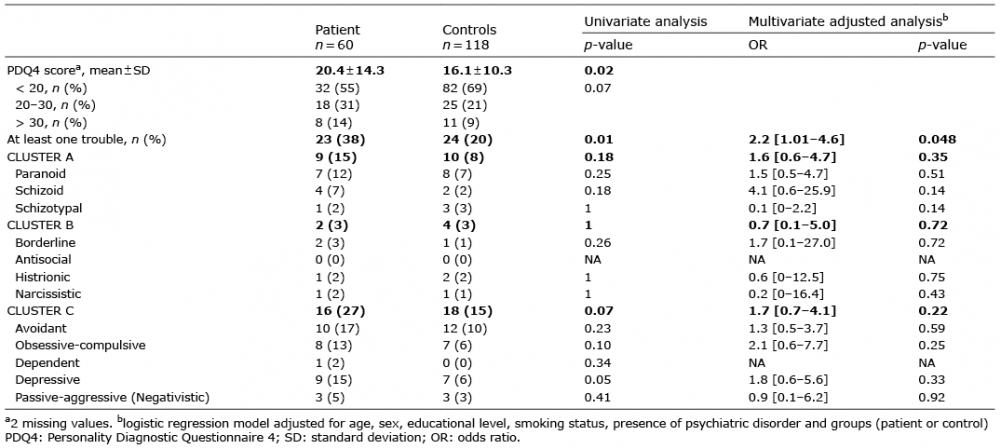 Click to show fullsize
Click to show fullsize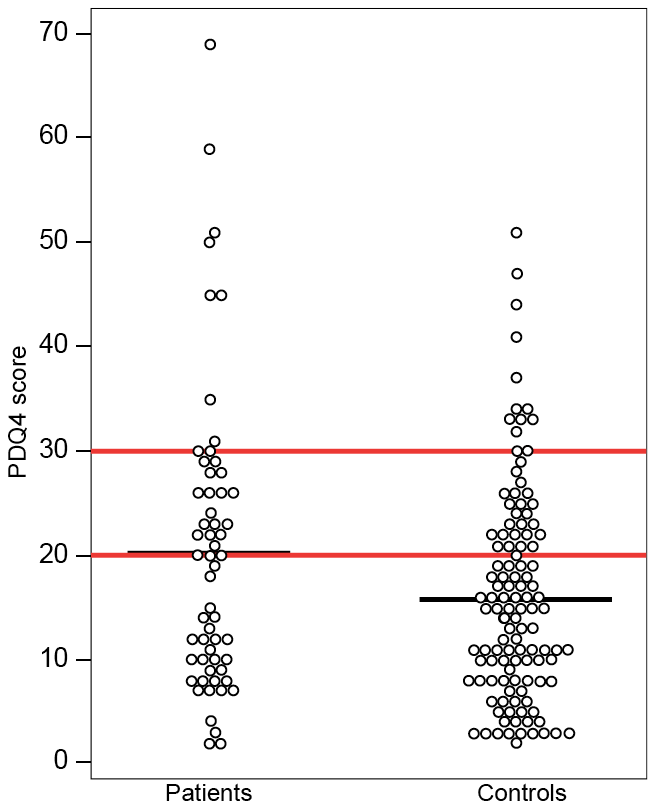 Click to show fullsize
Click to show fullsize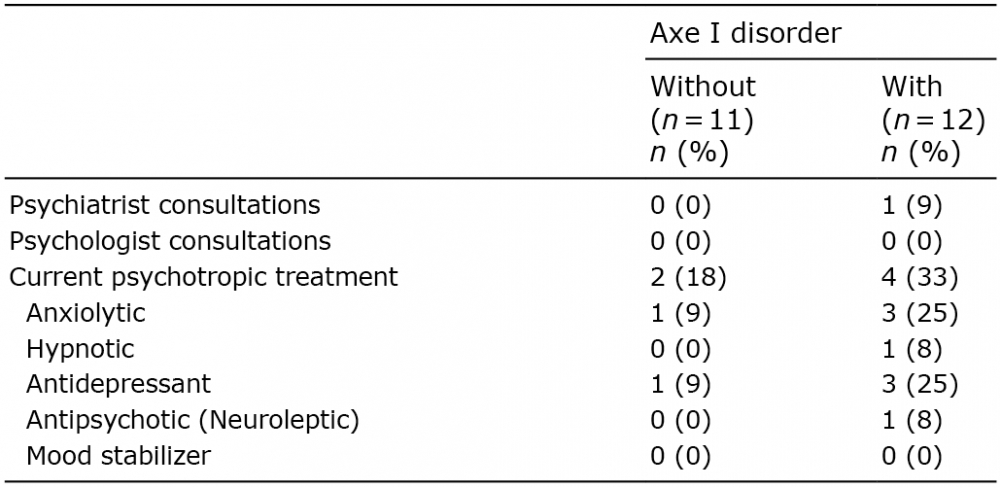 Click to show fullsize
Click to show fullsize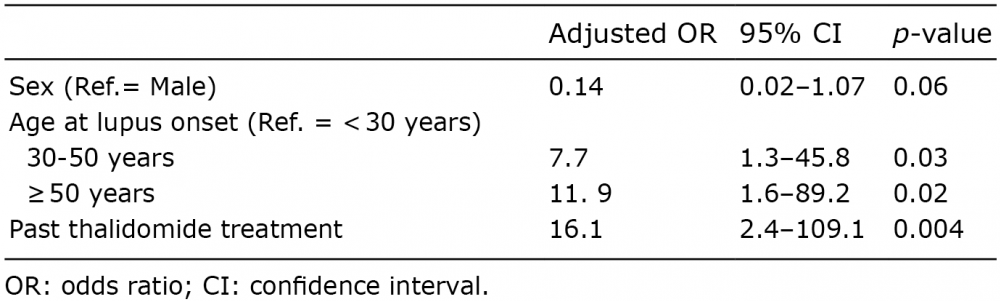 Click to show fullsize
Click to show fullsize