


1Dermatology, Department of Experimental, Diagnostic and Specialty Medicine, University of Bologna, Bologna, and 2Section of Dermatologic Surgery, Department of Oncology, Città della Salute e della Scienza di Torino Hospital, Turin, Italy
The introduction of dermoscopy has improved the accuracy of diagnosis of melanoma. However, early stage melanoma can be difficult to diagnose. Eighty-nine cases of thin melanoma with a Breslow thickness ≤1 mm located on the lower limb and diagnosed between 2008 and 2016 were assessed using 4 dermoscopic algorithms: (i) modified pattern analysis; (ii) ABCD rule of dermoscopy; (iii) 7-point checklist; and (iv) Menzies’ method. Two groups of early stage melanomas of the legs were identified: “difficult to diagnose melanomas” (DDM) and “non-difficult to diagnose melanomas” (NDDM). In our series the dermoscopic features of DDM were difficult to differentiate from melanocytic naevi, and the reticular pattern was the most frequently observed. “Depigmentation” was the only specific criterion associated with DDM. The sensitivity of diagnostic systems for thin melanomas of the lower limbs was lower than in previous studies. This result could be related to the lower mean Breslow thickness of the invasive melanomas in our sample and the high number of melanomas in situ. In conclusion, early stage
melanoma of the legs may be difficult to detect at clinical examination or with dermoscopic examination alone. Focusing on depigmentation in dermoscopy associated with anamnestic features could be a useful tool to detect difficult thin melanomas. In addition, sequential dermoscopy is recommended for high-risk patients with previous melanomas or atypical mole syndrome.
Key words: melanoma; leg; lower limb; dermoscopy; clinic; feature; characteristics.
Accepted May 16, 2017; Epub ahead of print May 17, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Emi Dika, Dermatology, Department of Experimental, Diagnostic and Specialty Medicine, University of Bologna, Via Massarenti, 1, IT-40138 Bologna, Italy. E-mail: emi.dika3@unibo.it
Cutaneous malignant melanoma is the most rapidly increasing cancer in white populations. The highest incidence rates are reported in Australia and New Zealand, with 30–60 cases per 100,000 inhabitants every year (1–2). Incidence rates of melanoma are also increasing in Europe and the USA (3–7). In Italy, the incidence of melanoma has increased in both sexes by more than 4% per year for the last 20 years, and a similar increase in mortality has been shown, especially in males. In Italian individuals younger than 45 years, melanoma is the third most commonly diagnosed cancer (8).
The increasing incidence of early stage melanoma (ESM) may be due to enhanced dermatology-led mass screening surveillance and improved digital technologies (3, 4, 7, 9–12).
Regarding the latter, dermoscopic criteria and algorithms have been developed in order to increase the sensitivity and specificity of melanoma diagnosis, al-though the detection of ESM can still present difficulties (13). Thin melanomas have a better prognosis than thick melanomas, therefore early diagnosis results in longer survival and lower morbidity and mortality. However, there are still some concerns regarding the use of dermoscopy that must be taken into account: (i) melanoma may present specific risk factors, clinical and dermoscopic features in different body sites (14, 15); (ii) dermo-scopy alone presents difficulties while dealing with ESM with respect to intermediate and thick melanomas (16). Difficult to diagnose melanomas (DDM) are detected more frequently in thin melanomas especially in those with a Breslow thickness ≤ 1 mm (17–20). In a recent study realized by Pizzichetta et al. (17) 97.95% of DDM were melanomas with a Breslow thickness ≤ 1 mm. In addition, the study stratified DDM by anatomical site. The percentage of DDM in the lower limbs was 21.3% (36/169), in the trunk/abdomen 16.05% (44/274), and in the upper limbs 13.84% (9/65) (17). Furthermore, in a study of the clinical, dermoscopic and histopathological evaluation of thin melanomas (Breslow < 1 mm) of the limbs in high-risk patients (previous melanoma or atypical mole syndrome), Carrera et al. (19) reported that 92% (33/36) of thin melanomas were located on the lower limbs, mostly below the knee (28/36, 78%). Furthermore, none of the DDM cases showed typical features of melanoma on dermoscopic analysis. Based on this information, and our institutional experience, we considered lower legs to be the most likely localization of DDM. This anatomical site was therefore considered in order to evaluate the most represented dermoscopic pattern, histological features, and the diagnostic sensitivity of 4 clinical and dermoscopic algorithms in ESMs with a Breslow thickness ≤ 1 mm.
All cases of early stage melanomas (l-ESM) on the leg diagnosed between June 2008 and September 2016, at the Skin Cancer Unit and the Laboratory of Histopathology, Dermatology, University of Bologna, were analysed retrospectively.
All melanomas were revisited blinded by 3 histopathologists of the dermopathology unit of Sant’Orsola Malpighi. The concordance rate between dermopathologists was considered when 2 out of 3 agreed on the classification of a lesion as melanoma. Each blinded pathologist expressed his or her opinion on the lesion.
Six dermatologists, 3 with considerable experience in dermo-scopy (10–20 years of experience) and 3 with moderate experience (less than 5 years of experience) used 4 different dermoscopic algorithms: (i) modified pattern analysis (11); (ii) ABCD rule of dermoscopy; (iii) 7-point checklist (13); and (iv) Menzies’ method (12).
On the basis of the clinical and dermoscopic images l-ESM were divided into 2 groups:
DDM, defined as melanomas presenting: (i) dermoscopic patterns indistinguishable from those of common naevi; or (ii) lacking specific melanoma criteria; (iii) with features similar to benign tumours (16–20).
Non-difficult to diagnose melanomas (NDDM): tumours featuring at least 2 dermoscopic melanoma specific criteria chosen by the observers (referred to in the text and tables as DS), and selected as follows: irregular network, depigmentation, multiple colours, veil, peppering, scar-like depigmentation, streaks or pseudopods, atypical vascular pattern and irregular multiple brown dots and globules.
The concordance rate between observers was considered when 4 out of 6 dermatologists agreed on the classification of the lesions in the 2 groups.
We consider DDM or NDDM only in the cases of l-ESM analysed in this paper.
The following selection criteria were used:
Lesion classified as melanomas by 2 out of 3 histopathologists were included in the study. Lesions considered as dysplastic naevi by at least 2 out of 3 histopathologists were excluded.
Only primary melanomas, stage IA or IB, with Breslow thickness ≤ 1 mm were included.
Melanoma arising on areas other than the upper and lower part of the leg, such as buttocks and foot, were excluded.
Patients with non-available dermoscopic images were excluded.
Anamnestic and clinical data that led to surgical excision of the suspicious lesions were evaluated and tabulated. Regarding medical history, 2 main reasons were reported: the positive anamnesis for melanoma and the previous excision of dysplastic naevi. With regards the clinical and dermoscopic evaluation we considered: (i) patient’s concern (“recent onset” and/or “rapidly changing of the neoplasms in dimensions or colour” “sensation of pruritus on the lesion’), (ii) the evaluation by clinicians of the “ugly duck sign” or “the presence of a single lesion”, categorized as clinician’s suspicion, (iii) dermoscopic change in lesions at follow-up.
All dermoscopic images (20× and 40×) were obtained using FotoFinder Medicam 800HD (FotoFinder Systems GmbH, Bad Birnbach, Germany), with alcohol-gel as linkage fluid.
All histopathological specimens were re-assessed considering American Joint Committee on Cancer 2009 final criteria (21).
This study considered 4 endpoints in the assessment of l-ESM in the 2 groups of patients (DDM/NDDM):
Endpoint 1: to evaluate patients’ demographic, clinical and histopathological data.
Endpoint 2: to detect the prevalent dermoscopic pattern of DDM/NDDM in thin melanomas with Breslow thickness ≤ 1 mm. Furthermore, the “2 most suggestive” dermoscopic diagnostic criteria for melanoma (DS1; DS2) were identified for each case and their frequency of distribution comparing the 2 groups.
Endpoint 3: to evaluate the diagnostic sensitivity of each diagnostic algorithm (modified pattern analysis, ABCD rule of dermoscopy, 7-point checklist, and Menzies’ method) in thin melanomas with Breslow thickness ≤1mm.
Endpoint 4: to assess the medical history and clinical data, which have proven useful in the identification of DDM.
Baseline characteristics were assessed and the patients were divided into 2 groups: with and without difficult melanomas. In these 2 groups differences in proportions, such as sex, diameter of lesion (larger or smaller than 6 mm according to the ABCD rule) and association between dermoscopic features, were evaluated using χ2 test. In addition, χ2 test for trend was used to evaluate DDM depending on the age of the patient and the thickness of melanomas. Fischer’s exact test was applied if any expected cell value in the 2 × 2 table was < 5. Finally, continuous variables, such as age and thickness, were also tested with t-test.
In addition, a univariate analysis was computed. Variable selection for the regression model was made on the basis of the literature reports. The group most represented in the sample was used as the reference category. In the logistic regression model the dependent variables were DDM or non-DDM, while the independent variables were age, sex, thickness and diameter of melanoma at diagnosis. Successive multivariate analysis was performed in order to show how the effects were modified when implementing the models with all independent variables. Enter function was used in the multivariate model and, finally, statistically significant and non-significant results were reported. Associations between the covariates and outcome were presented as odds ratios (OR) with 95% confidence intervals (95% CI).
Med Calc version 14.8.1 (http://www.medcalc.org) was used in the statistical analysis; a confidence interval of 95% and statistical significance of p < 0.05 were considered.
A total of 252 patients with melanoma located on the lower limbs were considered.
The following cases were excluded from the present study: 37 patients with a Breslow thickness > 1 mm; 35 with a diagnosis of acral lentiginous melanoma (ALM) of the foot and/or nail apparatus; 91 with unavailable dermoscopic images. A total of 89 (68 females and 21 males) with l-ESM entered the study (Table I). Thirty-six cases were defined as DDM (40.45%) and 53 as NDDM (59.55%).
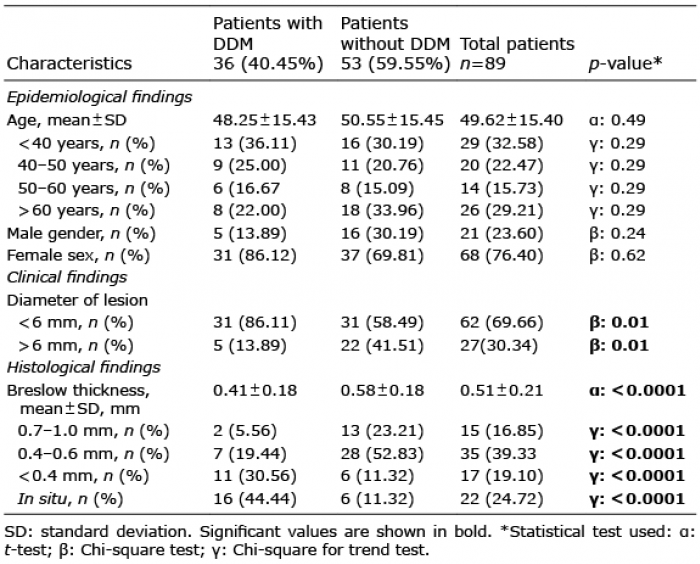
Table I. Epidemiological, clinical and histological differences between patients with and without difficult to diagnose melanomas (DDM) of the lower limbs
The results of the previously defined endpoints are:
Endpoint 1: prevalence of DDM was not correlated with age. The difference between these 2 groups in terms of mean age ± standard deviation (SD) was not statistically significant (p = 0.49). How-ever, the prevalence of DDM was 6 times higher in women than in men, although this difference was not statistically significant and was probably due to the high number of women in our sample. Clinically, 86.11% of DDMs were smaller than 6-mm diameter at the time of excision (χ2 test; p = 0.01). In addition, the percentage of DDM tended to increase with decreasing melanoma thickness; in our sample 75% of DDM were represented by in situ melanomas and invasive melanomas with a Breslow thickness <0.4 mm (χ2 test for trend; p < 0.0001) (Table I). Moreover, in the multivariate regression, implementing the models with all independent variables, Breslow thickness was the only risk factor correlated with DDM, especially in situ melanomas (adjusted OR 12.61; 95 % CI 1.92–82.65) and in melanomas with a Breslow < 0.4 mm (adjusted OR 8.58; 95 % CI 1.27–58.00). In contrast, the dimension of lesion (> 6 mm vs < 6 mm) did not prove statistically significant in the multivariate analysis (Table II).
Table II. Logistic regression of multiple independent variables with difficult to diagnose melanoma as outcome
Endpoint 2: regarding dermoscopy, the reticular pattern was the most frequently detected in l-ESM, observed in 66.67% of DDM and 66.04% of NDDM, respectively. Reticular/globular pattern was detected in 19.44% of DDM and only 9.43% of NDDM. Finally, multicomponent pattern was found in only 8.99% of NDDMs (p = 0.024) and was not observed in DDM group (Fig. 1, Table III). At least 3 suggestive dermoscopic melanoma criteria (DS1/DS2) were found in non-DDM, with a statistically significant association (Table III). The dermoscopic criterion “multiple colours” was seen in 45.28% of cases (p < 0.000001), the presence of irregular network was detected in 39.62% of cases, “veil” in 30.19% of cases (p = 0.017) and “scar-like depigmentation” in 15.09% of cases (p = 0.005) (Fig. 2). Depigmentation was the only dermoscopic criterion with a statistically significant association (p = 0.0016) with DDM. In addition double dermoscopic criteria suggestive for melanoma were not identified in 43.05% of DDM (p < 0.001) (Fig. 3, Table III).
Fig. 1. The most suggestive dermoscopic criteria (DS1 and DS2) in 89 cases of melanoma of the lower limbs. DS1: the first dermoscopic criterium suggestive for melanoma. DS2: the second dermoscopic criterium suggestive for melanoma.
Table III. Prevalent dermoscopic patterns detected and 2 main dermoscopic criteria (DS1 and DS2) of 89 cases of lower limbs melanomas
Fig. 2. Four cases of non-difficult to diagnose melanoma (NDDM). (a, d, g, l) Clinically atypical melanomas located on the lower limbs. Melanoma features detected at dermatoscopic evaluation: (b) irregular network with dermatoscopic island; (e) irregular network in an asymmetric lesion on 2 axes; (h) multiple colours; (m) scar-like depigmentation and veil. Melanoma features detected at histopathology: (c) the melanocytes at the epidermal-derma junction are atypical and aligned both as single units and nests. Nests are irregularly shaped, are close together in some foci and far apart in others and a few are confluent (haematoxylin and eosin (H&E) 10×); (f) single atypical melanocytes are scattered in the epidermis (H&E 10×); (i) irregular distribution of nests and single melanocytes at epidermal-dermal junction (H&E 4×); (n) melanocytic lesion with irregular junctional growth pattern and 1-mm Breslow thickness (H&E 2×).
Fig. 3. Three cases of difficult to diagnose melanoma (DDM). At clinical examination: (a) naevus larger than the others and reported as recdently grown; (d) naevus of recent onset with unremarkable aspect (arrow) in patient with a previous melanoma (arrowhead); (g) rapidly growing naevus with unremarkable aspect. Features detected at dermatoscopic evaluation: (b) reticular network with asymmetrical distribution; (e) reticular pattern without dermoscopic features of melanoma; (h) reticular pattern with depigmentation areas. Melanoma features detected on histopathology: (c) singular melanocytes migration upwards through the epidermis (H&E10×); (f) increased number of melanocytes are aligned in a continuous and contiguous row along the basis of the epidermis (H&E 10×); (i) irregular junctional growth pattern (H&E 2×).
Endpoint 3: regarding the diagnostic sensitivity of the dermoscopic algorithm: pattern analysis showed the best sensitivity (64.05%), whereas the 7-point check-list and Menzies’ method revealed similar sensitivities (61.08% and 57.30%, respectively). The ABCD dermoscopic algorithm showed the lowest sensitivity (42.70%) in our series (Table IV).
Table IV. Sensitivity of diagnostic systems in thin melanomas of the lower limbs
Endpoint 4: In addition, anamnestic data, such as previous melanoma or excision of dysplastic naevi, were related to one-third of DDMs.
Finally, the evaluation of data reported by patients or clinicians (categorized as “patient’s concerns” or “clinicians’ suspicion”) were frequently associated with DDM in our patients (33/36 = 88.65% of cases; Table IV); of the latter, when a DDM was diagnosed, a clinical doubt was reported in 100% of cases. Finally, 8 DDM were detected because of change in a lesion at dermoscopic follow-up (Fig. 4, Table V).
Fig. 4. Three cases of melanomas detected at dermoscopic follow-up; at (a–f) 3 months and (g–i) 6 months, respectively.
Table V. Anamnestic, clinical features and dermoscopic follow-up of studied patients
In the past 3 decades the development of new technologies has improved the diagnostic accuracy of pigmented lesions and melanoma (22–25). Digital dermoscopy is currently the most used technology, although novel non-invasive methods, such as spectrophotometric intracutaneous analysis and confocal microscopy, show promising results (26–28). Since the conception of the ABCD criteria for the clinical evaluation of melanoma, several studies have attempted to develop specific dermoscopic criteria and diagnostic algorithms that may facilitate diagnosis of melanoma. Data from the current literature and several meta-analyses have assessed the role of dermoscopy alone in ameliorating the diagnostic accuracy of pigmented lesions and melanoma (28–30). The detection of ESM, irrespective of the location, is one of the most important objectives of dermatological screening, due to the positive prognosis associated with early and prompt diagnosis of melanoma. In our experience, l-ESM may not present “evident” or “suggestive for melanoma” dermoscopic criteria, as described in advance stages of melanoma of the same region (9, 31). The most frequently reported patterns, such as the multicomponent or structureless pattern, in the presence of distinct melanoma criteria, such as the presence of “veil”, “multiple colours”, “atypical vessels” and “scar-like depigmentation” were not observed in our series of DDM. In our series the dermoscopic features of DDM were difficult to differentiate from melanocytic naevi and the reticular pattern is the most frequently observed (Fig. 3b, e, h). These observations might explain the diagnostic difficulty in the detection of this subset of melanomas. “Depigmentation” was the only specific criterion identified in DDM, and this association proved statistically significant (p = 0.0016).
The association between the dermatoscopic criteria and thickness of melanomas has not always been reported. Ciudad-Blanco et al. (32) did not point out any differentiation between invasive melanoma and melanoma in situ of difficult and simple diagnosis in order to detect a possible correlation between dermoscopic criteria and Breslow thickness. However, in melanoma in situ white areas, blue-white veil structures were reported in 2% of lesions, in accordance with our results. With regards to invasive melanomas, dermoscopic criteria have been associated with all invasive melanomas without any differentiation according to Breslow thickness.
In contrast, Carrera et al. (19) included only thin melanomas (< 1 mm of Breslow) located on the limbs. In this study melanomas were divided into 4 groups and those of the second group were characterized by depigmentation as typical dermoscopic finding. This result could be comparable to the depigmentation criterion found in the DDM of our sample. The term “depigmentation” should be differentiated from the terms “regression”, used by many papers, as “regression” is a histopathological event, and “scar-like depigmentation”. We found a significant difference in the distribution of these 2 criteria in patients affected by l-ESM, assessing that “depigmentation” represented a distinctive clue in the dermoscopic presentation of DDMs. On dermoscopy “scar-like depigmentation”, was considered as the presence of whitish areas (white scar-like areas) that may be associated with a white veil or the so called “crystalline structures”, and “depigmentation” as the detection of an area characterized by a loss of the pigmented network, not necessarily whitish, but also a lighter brown in colour with respect to the rest of the lesion (Fig. 2m).
Wolf et al. (33) pointed out that thick melanoma lesions were clinically more difficult to diagnose than thinner ones. In contrast Pizzichetta et al. (17) hypothesized that dermatoscopic visible features of melanoma become evident with the growth of the lesion. Our study, through a multivariate analysis, supported this statistical correlation between DDM and lower Breslow thickness. In fact, 94.44% of DDM presented a thickness of Breslow thickness or equal to 0.6 mm. Seventy-five percent of melanomas DDM have a Breslow thickness less than 0.4 mm. Almost half of melanomas were in situ melanomas (Table II).
In our sample the dermoscopic sensitivity score was lower than in previous studies (Table V). This result could be related to the lower mean Breslow thickness of invasive thin melanomas in our sample. As an example, we can consider that Menzies’ criteria were tested on 45 invasive melanomas with a median Breslow thickness of 0.7 mm; the sensitivity reported was 92% (12). In contrast, in our sample, the median Breslow thickness of invasive melanomas was 0.51 ± 0.21 mm (SD) and the sensitivity was 57.30%. In addition, in our sample almost half of DDM were melanomas in situ.
Moreover, also at histological examination, the diagnosis was more difficult for DDM than for NDDM, as the histological characteristics that allow the differentiation of a melanoma from a dysplastic naevus were less pronounced (Fig. 3c, f, i).
Anamnestic features were considered to cut off melanocytic lesion in 40% of cases. Clinical features, such as patient’s concern and clinicians’ suspicion, were useful in approximately 57% of cases (Table IV). Finally, some lesions, especially in high-risk patients with previous melanomas or atypical mole syndrome, were excised because of change at dermatoscopic follow-up (Fig. 4).
In our experience, considering the statistical correlations on l-ESM diagnosis, the clinical and anamnestic data appeared as useful and important as the assessment of various dermoscopic algorithms.
This study has some limitations. First, it is a retrospective study. Secondly, there is a possible lack of objectivity in interpreting the dermoscopic findings of melanocytic lesions because the histological confirmation of melanoma was known in all cases. Thirdly, the patients’ phototype was not evaluated, although the latter might influence or correlate with the dermoscopic pattern of melanomas.
For very early melanomas (in situ and invasive melanomas with a Breslow thickness < 0.4 mm) and featureless melanomas, clinical examination or dermoscopic evaluation alone may not be sufficient for diagnosis. Follow-up dermoscopy is important for these lesions showing depigmentation with reticular pattern, as in patients at high risk with atypical mole syndrome the immediate systematic removal of these lesions would lead to a lot of unnecessary biopsies. It is also important to assess the signature of naevi in high-risk patients, as these may show some areas of depigmentation in many of their atypical nevi, which would be regarded as less suspicious if present in many lesions (34, 35). Further studies on larger samples are needed to confirm these data and to assess the dermoscopic findings of thin melanomas in specific locations, such as the face or mammary region, and in special sites, such as mucosal or acral sites. We hypothesize that early thin melanomas may differ clinically and dermoscopically depending on their anatomical background.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize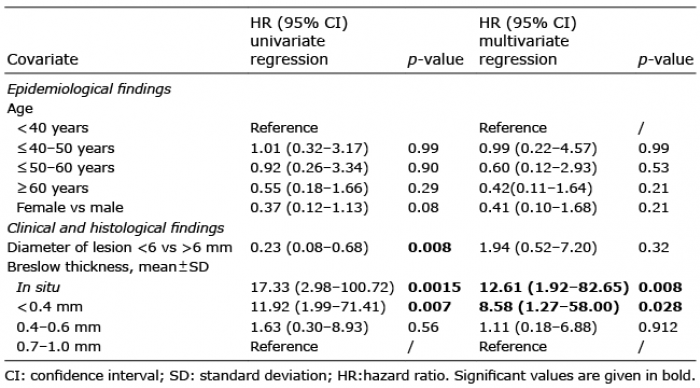 Click to show fullsize
Click to show fullsize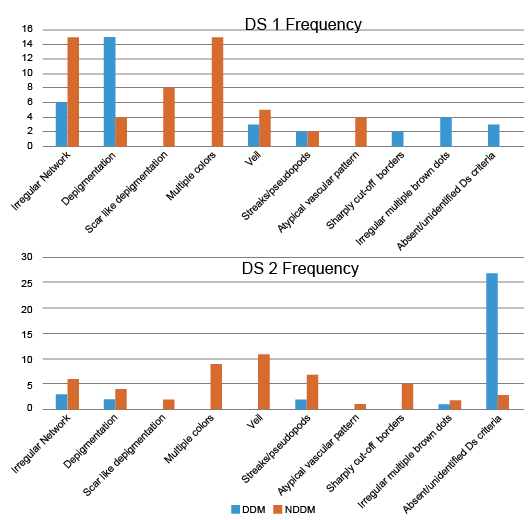 Click to show fullsize
Click to show fullsize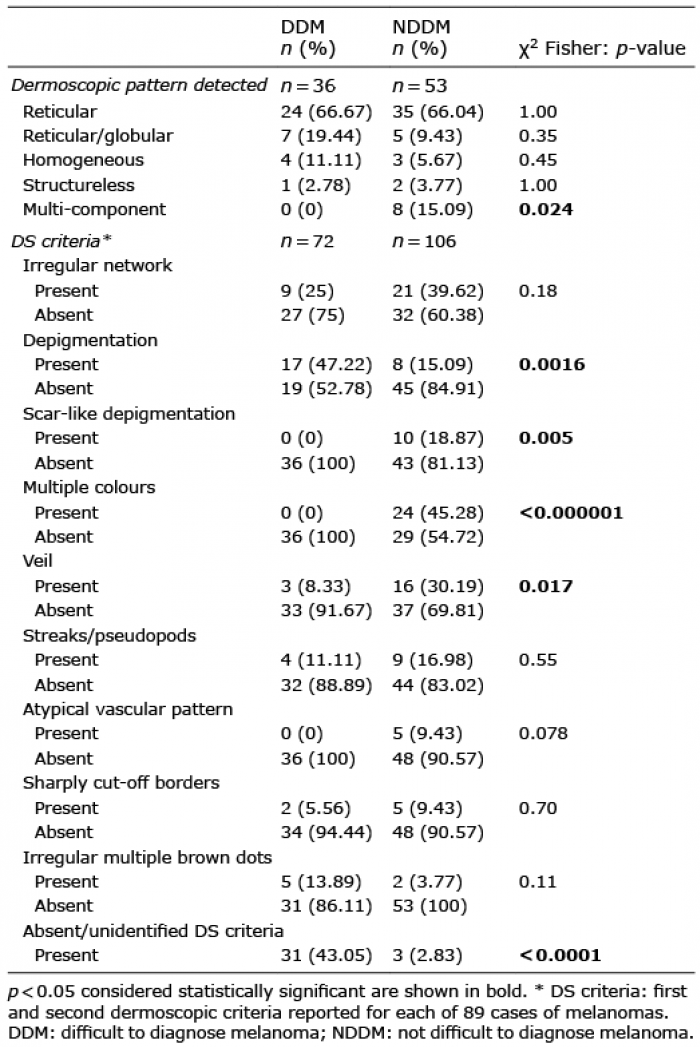 Click to show fullsize
Click to show fullsize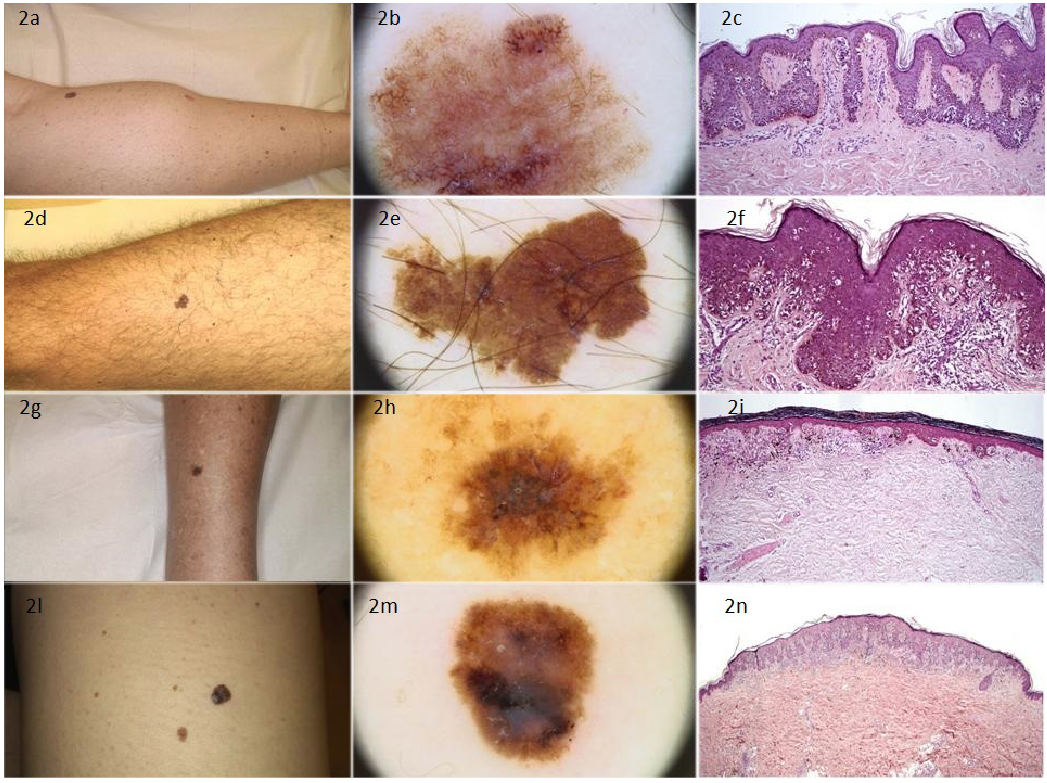 Click to show fullsize
Click to show fullsize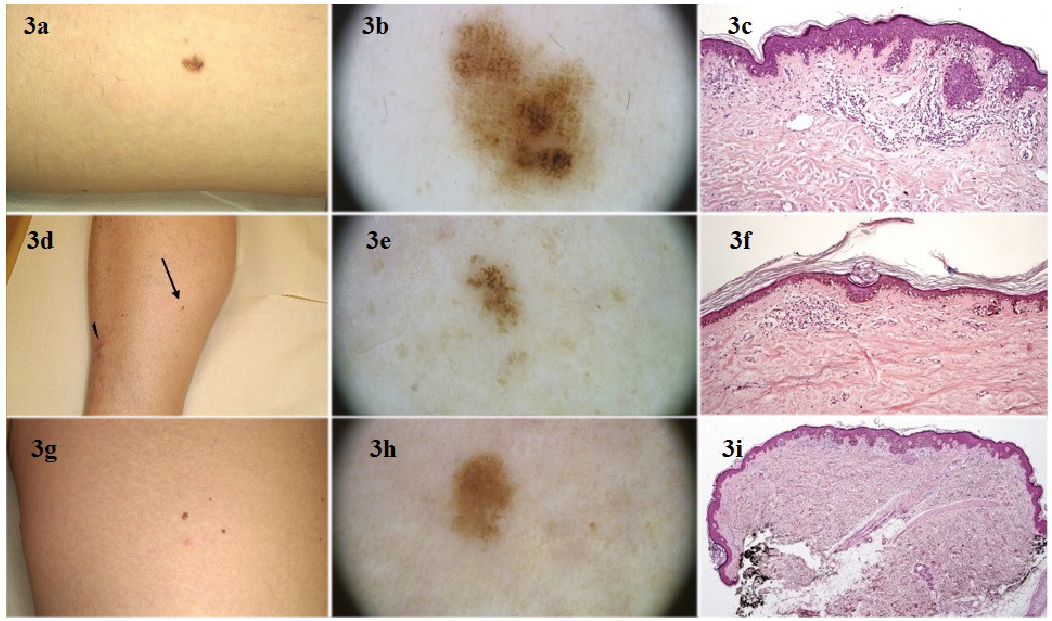 Click to show fullsize
Click to show fullsize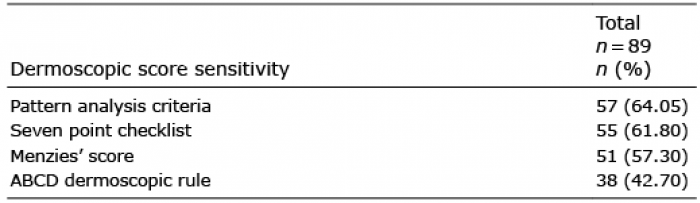 Click to show fullsize
Click to show fullsize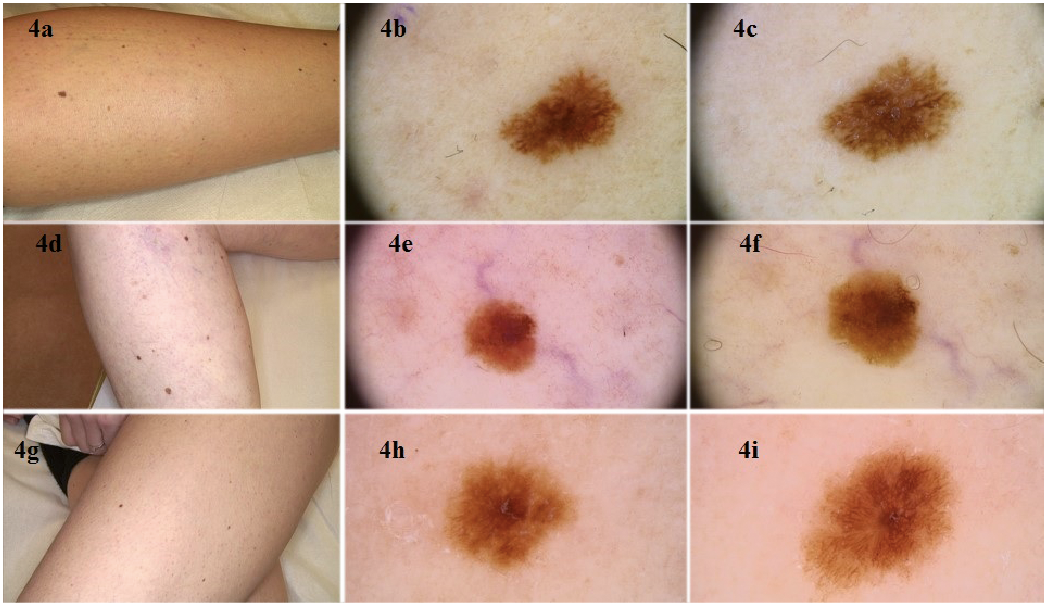 Click to show fullsize
Click to show fullsize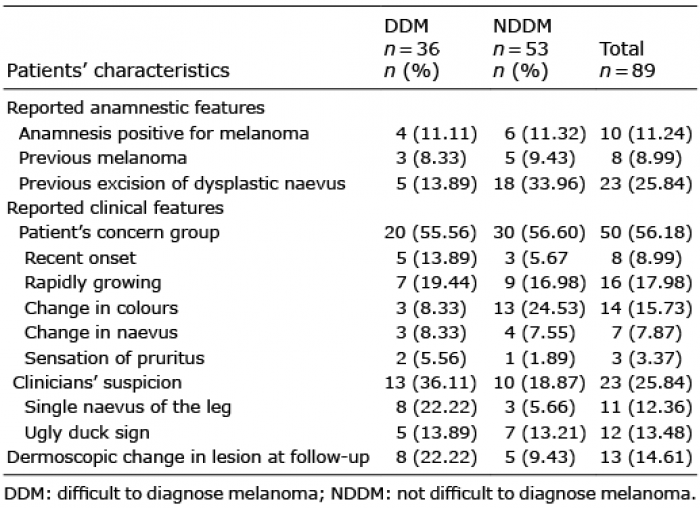 Click to show fullsize
Click to show fullsize