


1Cutaneous Imaging Clinic, Department of Medicine, Vanderbilt University Medical Center, 2Vanderbilt University Department of Biomedical Engineering, and 3Dermatology Service, Nashville VA Medical Center, Nashville, USA
Most dermatologists are aware of the benefits of dermoscopy, and a few are familiar with laser-scanning confocal microscopy. Beyond confocal, there are fully 11 different categories of optical techniques that have been applied to clinical dermatology. This article first provides a comprehensive tabular overview of all these optical diagnostic technologies and then details 4 of the lesser known innovations that are already available or still in development (laser Doppler and speckle imaging, Raman spectroscopy, multiphoton microscopy, photoacoustic tomography), with some potential applications in clinical dermatology (blood flow monitoring, skin cancer diagnosis, composition measurements in atopic dermatitis, skin rejuvenation measurement, and noninvasive sentinel lymph node assessment in melanoma). These methods present many advantages, being non-invasive, portable, and rapid. The development of optics in biological and biomedical sciences (i.e. biophotonics) requires not only deep insight into the applications but also synergistic collaboration be-tween engineers and clinicians.
Key words: non-invasive imaging; laser Doppler and speckle imaging; Raman spectroscopy; multiphoton microscopy; photoacoustic tomography; melanoma.
Accepted May 22, 2017; Epub ahead of print Jul 3, 2017
Acta Derm Venereol 2017; Suppl 218: 5–13.
Corr: Dr. Eric Tkaczyk, One Hundred Oaks Suite 26300, 719 Thompson Lane, Nashville, TN 37204, USA. E-mail: eric.tkaczyk@vanderbilt.edu
Optical instrumentation for imaging is an important component of biological and medical science progress. The range of applications of biomedical optics devices is very broad, from medical diagnostics, monitoring treatment to clinical research (1). Medical imaging has already dramatically transformed the practice of medicine in a variety of clinical settings. Optical methods and devices are indeed advantageous, because they are non-invasive, portable, relatively inexpensive, and they can provide rapid information to the physician (2).
In the field of dermatology, non-invasive imaging technologies are particularly useful for skin disease diagnosis and monitoring, including skin cancer detection. This is especially the case when cutaneous conditions present ambiguous features, leading to delays in treatment. Many optical imaging methodologies are currently developed to improve the diagnosis of a variety of skin conditions without the need for biopsy, which remains the gold standard for skin neoplasms (3–5). Patient burden would be greatly reduced if biopsy could be avoided for even a subset of benign lesions through reliable non-invasive optical tools. Recent breakthroughs in morphological and physiological diagnostic methods enable imaging with higher resolution and functional data. Advances in imaging devices (6) such as dermoscopy, ultrasound, optical coherence tomography, and most notably reflectance confocal microscopy (7) have allowed these techniques to be applied to skin neoplasms and inflammatory disease management. Other dermatologic applications include assessment of moisture, burn depth, wound healing, UV damage and atrophy. In fact, no fewer than 11 fundamentally different optical technologies have been applied to dermatology patients. For the reader, a convenient and annotated overview table is provided in Table I for reference of all of these different techniques.
In addition to the overview provided in the Table I, this paper will review the potential applications of 4 optical devices and imaging techniques that are not widely known in clinical dermatology. Applications that will be discussed include blood flow monitoring with laser Doppler and speckle imaging, mapping chemicals and water in skin with Raman spectroscopy, visualization of the composition and structure of the skin in high-resolution by multiphoton microscopy, and deep imaging of melanin by photo-acoustic tomography. Considerations for selecting the most appropriate existing or emerging imaging technique for evaluating specific cutaneous conditions will also be presented.
Two techniques, laser Doppler and laser speckle imaging, can be used for blood flow mapping and imaging in the skin (8). Laser Doppler velocimetry measures velocity of blood flow by using the frequency shift induced by the Doppler effect. It has already been used in many medical and surgical situations to monitor blood flow or other tissue movements in the body. Laser speckle is a random interference effect that gives a granular aspect to objects illuminated by laser light. For individual moving scatterers (such as blood cells), the speckle pattern waves lead to so-called time-varying laser speckle. These fluctuations reflect the velocity distribution of the scattering particles. Both techniques perform measurements at a single point and in this regime can be shown to be mathematically equivalent results of interference. The single point imaging drawback can be overcome to measure blood flow in real time by coupling the technique with scanning of the area (8). With the speckle technique it is also possible to apply a full-field technique that gives an instantaneous map of velocities in real time. In dermatology, blood flow imaging can be used to evaluate inflammation and erythema, by measuring quantitatively velocity and haemo-globin content in capillaries of the skin. Numerous autoimmune, drug-induced, genetic, and inflammatory skin diseases and even scars can benefit from such assessment. Herein we will discuss two examples: patch test quantification used in the diagnosis of contact dermatitis, and monitoring the efficacy of vascular lesion treatments.
In medical practice, blood flow measurement can be applied to patch testing, which is used to diagnose contact allergy. Indeed this in vivo test aims to mimic allergic contact dermatitis by reproducing the triggering step of the reaction to a contact allergen (9). The methodology is simple and consists in applying allergens under occlusion on the skin under standardized conditions. However it requires adequate training for the results to be correctly interpreted and used, especially when a too weakly positive reaction appears. In this case, an objective and user-independent assessment of the test reaction can be obtained using blood flow measurement by either laser Doppler or speckle imaging. Both technologies allow quantifying the amount of inflammation at each test site (10), thereby driving dermatologists’ final decision (Fig. 1).
Fig. 1. Laser doppler imaging of blood flow in a patch test. Printed with permission from Fullerton et al. (2002) (10). The perfusion image can be analysed by an integrated system software. The relative colour scale extends from the smallest and the largest perfusion value (from green to red). (https://www.perimed-instruments.com/skin-patch-testing).
For cosmetic procedures, laser Doppler and speckle imaging can also be used to evaluate the performance of skin treatment by laser therapy, with the aim to improve its efficacy (2). In particular, in the treatment of port wine stain birthmarks, the efficacy of laser therapy is limited, with only 10% of cases resulting in complete disappearance of redness after ten laser sessions (11). One factor is that the procedure relies on the subjective impression and overall experience of the clinician. Therefore Doppler/speckle imaging may serve as a metric of the degree of photocoagulation after laser surgery of port wine stain, and will identify areas with persistent perfusion that are not visible to the naked eye. The Speckle Flow Index (SFI), obtained with laser speckle imaging instrumentation by converting raw speckle reflectance images to speckle contrast images, is a numerical value proportional to the degree of scatterer motion and is higher in feeding vessel regions (Fig. 2). This indicator of microvasculature provides real-time, quantitative feedback during laser surgery, enabling the clinician to go back to the persistent perfusion areas until complete blanching is reached. Both laser Doppler and speckle imaging are innovative and individualized methods that could reduce the number of laser treatment sessions, hence optimizing results and diminishing the cost and potential risks associated with general anaesthesia for this intervention.
Fig. 2. Laser Speckle Imaging (LSI) of a Caucasian female patient with a port wine stain involving the V2 dermatomal distribution. Printed with permission from Huang Y.C. et al. (2008) (11). (a) Photograph. (b) Speckle Flow Index images taken from the marked region of interest immediately before and (c) 15 min after laser therapy. Colour range indicates the level of blood flow in this area.
Overall, these approaches are low cost technologies and offer a non-contact method of mapping ?ow ?elds such as capillary blood ?ow, avoiding skin blanching by pressure which is a common drawback of measurement devices requiring skin contact (2). Meanwhile they present two main limitations: a low spatial resolution and a relative measurement of the blood flow only at a top surface view. Another potential limitation of laser speckle imaging is that the SFI values also are dependent on tissue optical properties. Some alternatives to improve resolution and sensitivity are to combine these techniques of visualization of tissue function, with optical coherence tomography or diffuse optic techniques, such as spatial frequency domain imaging (SFDI), which also enable visualization of changes in skin structure (see references in Table I, Overview of optical imaging techniques).
Laser Doppler imaging is on the market and has been for some time, whereas laser speckle contrast imaging is still used mostly in the research setting. It may be worth further developing laser speckle technique for commercialization, because of 3 main advantages over laser Doppler imaging: lower cost, truly real-time operation enabling movies of perfusion changes (8) and potential ease of integration into current laser systems (11).
In clinical dermatology research, it is important to evaluate the efficiency of topical therapeutic interventions and decipher the mechanism underlying their effect, how they distribute and at which concentration in the skin. For this purpose, it is necessary to quantify and follow the mapping of chemicals or biological compounds in the outermost layers of skin. However, most approaches that are able to provide direct information about skin components or the depth profiles of water content, such as tape-stripping and micro-dialysis, are invasive and/or time-consuming. Raman spectroscopy by contrast can identify skin constituents and provide spatially resolved molecular information under in vivo conditions in a non-invasive and rapid manner. It is based on depth-resolved vibrational spectra of molecules at optical wavelengths and can monitor conformational changes in lipids and proteins of the skin. Thus, Raman is accepted as a reliable method to quickly and noninvasively measure skin hydration, retinol, lactate and many other molecules (12, 13).
Natural moisturising factor (NMF) is a breakdown product of filaggrin (encoded by the gene FLG) consisting mainly of a range of hydroscopic amino acids (14). It has been shown that FLG mutations are a major predisposing factor for atopic dermatitis (AD), with approximately 50% of moderate-to-severe AD cases harbouring filaggrin null-alleles (15). These mutations have a clear permissive effect in the early inflammatory phenomena that characterize eczema and affect both priming of disease and chronicity. Treating newborns with filaggrin mutations and low NMF levels with daily full-body emollient therapy was found to reduce the incidence of AD at 6 months of age by 50% (16). The early follow-up of NMF levels might therefore allow timely prophylactic treatment and appropriate surveillance.
Raman spectra can provide specific signatures of NMF levels that predict FLG mutation status, overcoming the need for the more technically demanding genotyping or invasive investigation. This technique accurately predicted newborn infants’ filaggrin genotype with 98–96% sensitivity and 87–67% specificity (Fig. 3). Raman spectroscopy could also be applied to give fast and quantitative information before and after emollient application.
Fig. 3. Cloud plot of natural moisturising factor (NMF) values in newborns, obtained from Raman spectra and categorized by filaggrin (FLG) genotype (final genotype after full screening: FLG+/+, FLG+/–, FLG–/–). From O’Regan GM et al. (2010) (15). For each group, the number of patients and NMF level (mean ± SD) are indicated in the figure. a.u.: arbitrary units.
A wide range of research applications for in vivo Raman spectroscopy is now available (13). However, unlike other techniques that produce images, Raman is at present mainly used for single point measurement. One significant limitation is that the weak Raman effect gives insufficient signal strength to quickly acquire an image. This drawback can be overcome in the future through nonlinear implementations. In particular, multiplex stimulated Raman scattering microscopy may provide rapid dynamic imaging at video rate to monitor delivery and diffusion of topical agents, such as sunscreens, moisturizers, tretinoin and metronidazole, through skin tissue in vivo (17). As most chemicals of interest have known Raman spectra, nonlinear Raman technology should enable real-time ascertainment of their distribution without labelling and at the cellular scale in the skin.
Multiphoton microscopy (MPM) is a femtosecond laser scanning microscopy technique based on nonlinear light-matter interactions to produce 3-dimensional (3D) images with submicron resolution (18). The most important signals are two-photon excited autofluorescence (AF) and second harmonic generation (SHG). By this way, images of endogenous biomolecules within tissue can be obtained without using specific fluorescent labels. Indeed, autofluorescence resulting from the distribution of endogenous fluorophores in tissue yields structural and biochemical information without fixation or staining procedures. The main compounds present in skin with two-photon autofluorescence are reduced nicotinamide adenine dinucleotide (NADH), flavine adenine dinucleotide (FAD), keratin, melanin, collagen, and elastin fibres (Fig. 4). Furthermore, SHG is able to visualize collagen fibres in the dermis. Therefore, MPM provides non-invasive in vivo imaging of the epidermis and superficial dermis, providing useful morphological and label-free molecular information (18).
Fig. 4. In vivo MPM imaging of normal human skin. Left, horizontal sections of MPM images (x–y scans) at different depths showing images of: the stratum corneum (z = 0 μm), keratinocytes normally distributed in the stratum spinosum (z=25 μm), basal cells (green) surrounding dermal papilla (blue; z=65 μm), collagen (blue) and elastin fibers (green) in the dermis (z=100 μm;). Right, cross-sectional view (x–z scan) corresponding to a vertical plane through the horizontal sections on the left. Scale bar is 20 μm. Image kindly provided by Dr Mihaela Balu from University of California, Irvine/Beckman Laser Institute.
One potential MPM application is melanoma, for which new and better treatments are now available but are also very expensive (as much as 36,000 USD/patient/month or more depending on the treatment (19)). In addition, melanoma incidence has been increasing for 30 years and is responsible for around 72% of skin cancer deaths in the USA (20). Early detection and accurate diagnosis of melanoma is therefore critical for a good prognosis and appropriate treatment. Current standard diagnosis is based on invasive biopsy and histopathologic examination. In addition, significant discordance among pathologists has been often documented for the classification of melanocytic neoplasms (21), resulting in meaningful change in clinical management in about 18% of cases (22). This observation has highlighted the urgent need to find more consistent skin tumour staging parameters to improve the accuracy of diagnosis decisions by dermatologists.
A few groups are exploring the ability of MPM to provide qualitative and quantitative information for diagnosis of skin lesions. In a small pilot clinical study, Balu and colleagues (18) derived a quantitative algorithm to distinguish multiphoton features of melanocytic naevi at different stages. The authors managed to derive a numerical multiphoton melanoma index (MMI), combining 3 main criteria, the melanocyte dendrite density, SHG signal strength (from collagen) and the autofluorescence, which was able to distinguish benign from atypical naevi or melanoma.
Studies in larger patient populations are still necessary to validate the diagnostic performance of MPM for both melanocytic and non-melanocytic tumours (23). Current MPM are unfortunately not suitable for wide-spread clinical use due to several limitations. Practical limitations include firstly an extraordinary high cost (> 400 000 EUR, quotation obtained by the author of this article in 2015 from Dermainspect), which is partially driven by the expense of the required femtosecond laser and so may fall with inevitable laser technology advances. Secondly, scan times are several orders of magnitude larger than for reflectance confocal microscopy, which provides similar resolution but no compositional information due to lack of discrimination of autofluorescence. Finally, technical challenges include limited field of view (about 250 × 250 µm2) and penetration depth (about 200–300 µm) (23). The penetration depth is non-inferior to confocal microscopy and much less of a concern in practice than the tiny sampled area accommodated by the fraction of a mm2 field of view. Indeed, since skin lesions are often non-uniform, presenting focal dysplasia, skin areas in excess of a couple mm often have to be examined microscopically in order to avoid false-negative diagnoses. The scanning field can be increased by either acquiring mosaic images (i.e. adjacent field of views) or redesigning the optical parts of the microscope. However MPM is unlikely in the foreseeable future to be able in a matter of minutes to capture entire lesions on the skin that are several mm2, which by contrast is the case for confocal imaging. Therefore, MPM will need to undergo substantial advances before it can be used clinically for cancer diagnosis.
Multiphoton microscopy is increasingly used in applied dermatological research, in the fields of skin aging, nanoparticle imaging, tissue engineering, and in situ screening of pharmaceutical and cosmetic products. It is particularly useful in skin aging clinical studies to obtain quantitative information on extracellular matrix components under physiological conditions, by measuring both the two-photon autofluorescence of elastin and the SHG of collagen. The SAAID (SHG-to-AF Aging Index of Dermis) of skin is an indicator deduced from MPM data and calculated as the (Intensity of Collagen – Intensity of Elastin)/(Intensity of Collagen + Intensity of Elastin) (24). This index is well correlated with skin photo-aging in vivo, and is a valuable tool, e.g. to monitor anti-aging cosmetic treatments.
Photo-acoustic tomography (PAT), also referred to as opto-acoustic tomography, is an emerging imaging technique with significant promise for biomedical applications. PAT is defined as 3D-imaging of a material based on the photo-acoustic effect and its principle can be summarized as “light in, sound out” (25). In this technology, light is absorbed by biological tissue and converted to transient heating, which subsequently creates an ultrasonic wave by thermo-elastic expansion. Ultrasound can then be detected by broadband ultrasonic transducers, and converted into tomographic images. Photo-acoustic imaging can be performed either by (i) relying on intrinsic tissue contrast alone (e.g., mapping endogenous chromophores such as melanin, haemoglobin, and lipids); or by (ii) using exogenous molecular imaging agents (25). This technology has the unique combined ability to make use of endogenous contrast alone to provide real-time images, at clinically relevant depths, with relatively high spatial resolution, all without the use of ionizing radiation. It can also be portable, is relatively cheap and safe, making it even more adoptable and integrable for clinicians. It can additionally monitor anatomical, functional, molecular and metabolic parameters that can potentially provide more comprehensive information for diagnosis, staging, and treatment of diseases (26).
In dermatology, PAT is most frequently explored for deep imaging of melanin to determine melanoma prognosis and staging. Most melanomas, even those that clinically appear pale and are classified as “amelanotic” actually contain melanin. This highly light-absorbing pigment naturally provides strong contrast for photo-acoustic imaging. PAT can distinguish and image both haemoglobin and melanin based on their respective absorption spectra, thereby allowing identification of early melanoma and angiogenic vessels. One implementation of PAT, sub-wavelength-resolution photo-acoustic microscopy (SW-PAM), has been developed to resolve subcellular organelles, and can image individual red blood cells and quantify individual melanosome melanin distribution in vivo (27). PAT can also accurately measure the metabolic rate of oxygen in melanoma, potentially improving early detection of this cancer (25). A handheld clinic-ready device has recently been pioneered as well, which is able to quantify the volume of pigmented lesions. This may herald photo-acoustic adaptation in high-risk melanoma clinics (28, 29).
PAT could some day in the future replace conventional sentinel lymph nodes excision. This important diagnostic procedure for metastatic melanoma, in the traditional method, is highly invasive and requires radioactive tracing. However, the sensitivity of PAT for melanin is roughly 50 times higher contrast than by light microscopy (27). This is so high that PAT can detect melanocytes in vivo in human lymph nodes, identifying microscopic metastatic disease. Combining the contrast agent indocyanine green, which tracks the lymphatic drainage, with PAT imaging of melanin has shown early promise in a clinical trial for sentinel lymph node detection (Fig. 5). In a trial of 20 melanoma patients, this approach identified all positive sentinel lymph nodes in vivo and ex vivo without a single false negative (189 total lymph nodes), with 100% sensitivity and 48 to 62% specificity (30). The low specificity means that half of the time, the PAT-positive lymph nodes were false positives due to nonspecific haemorrhage or melanin in lymph nodes. However, the high sensitivity nevertheless indicates that a non-invasive, non-radioactive photo-acoustic approach can confidently rule out the presence of lymph node metastases in patients who test negative. This approach could potentially spare 50% of patients an unnecessary and inconvenient surgical procedure in the future (30). In the aforementioned study, lymph node metastasis of amelanotic melanomas contained enough melanin to be detected. However, this needs further validation as amelanotic melanomas have the risk to be the Achilles heel of this absorption-based technique.
Fig. 5. Preoperative assessment of sentinel lymph node melanin content using multispectral opto-acoustic tomography (MSOT). Printed with permission from Stoffels I. et al. (2015), (30). Sentinel lymph node of a patient with metastasis per a combined 3D rendering of an MSOT image taken by the 3D detector that shows both melanin (red) and indocyanine green (ICG) localization. The skin pigment appears in yellow. MSOT imaging was able to localize sentinel lymph node and melanin to provide information on the metastatic status of the lymph node.
Circulating tumour cells have proven to have important prognostic implication in most major cancers and have driven the birth of the field of non-invasive flow cytometry (31). Melanoma is no exception. PAT has been applied to basic science studies of in vivo flow cytometry. Photo-acoustic flowmetry can perform label-free imaging of single flowing red blood cells and circulating tumour cells in skin capillaries with millisecond-scale temporal resolution and micrometer-scale spatial resolution. Thus, it is able to provide a reliable enumeration of melanoma cells in blood samples (32). Up to now, photo-acoustic flow imaging has not been applied clinically, but it could be a significant step toward both an efficient disease monitoring technique and a diagnostic tool. It will also enable scientists to study melanoma metastatic cells at the molecular and genetic levels in hope of better understanding the processes by which they metastasize, which could result in the development of more efficient therapies for cancer patients, including the prevention of metastatic cancer by novel targeted destruction of circulating melanoma cells.
Technologies based on photo-acoustics are still in their early research phase and face some limitations. For instance, light attenuation limits the ultimate imaging depth. To address this limitation, novel light illumination schemes have to be explored, such as illuminating the object from both sides or internal delivery of light (26). Quantitative PA imaging also faces challenges because of the difficulty in measuring local ?uence distribution. Advanced spectral separation algorithms have been proposed to address this issue.
With its unique combination of optical absorption contrast and ultrasonic imaging depth and resolution scalability, PAT shows great potential in the future for both biomedical research and clinical practice, and more specifically, for facilitating the diagnosis of both primary and metastatic melanoma.
Medical imaging has dramatically transformed how clinicians evaluate, diagnose, monitor, and treat disease. The highly visual nature of cutaneous diseases makes digital imaging valuable in everyday practice of dermatologists. Thus, biophotonics has become a useful tool to assess a variety of skin conditions. Table I summarizes the clinical uses, advantages and limitations of all optical imaging technologies that we are aware of in dermatology, including the 4 techniques reviewed here. In practice, no single imaging method will be ideal for all skin conditions. Many clinical problems will require multimodal in vivo imaging. With advancements and improved standardization of non-invasive imaging in dermatology, clinical practitioners may be able to better capture and monitor skin conditions over time and achieve better diagnostic accuracy, resulting in fewer biopsies, decreased morbidity, and ultimately less cost. Moreover, since great innovations for skin imaging have often been the result of the interplay between engineers and clinicians, they have to continue to work together and to define common roadmaps to maximize the benefit of innovative technologies for actual clinical needs.
Dr. Tkaczyk is grateful for support from NIH K12 CA090625. Cécile Desjobert and Marielle Romet (Santé Active Edition) provided medical writing assistance funded by Pierre Fabre Dermocosmetique. We are grateful to Dr Mihaela Balu from University of California, Irvine/Beckman Laser Institute for providing multiphoton microscopy images.
The author declares no conflicts of interest.


 Click to show fullsize
Click to show fullsize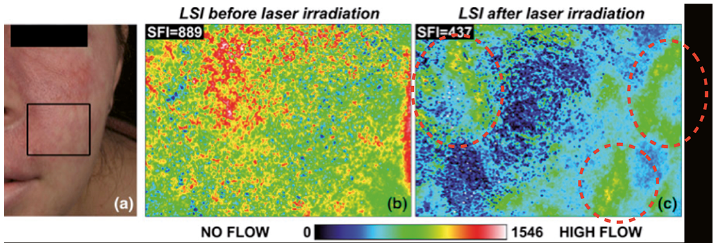 Click to show fullsize
Click to show fullsize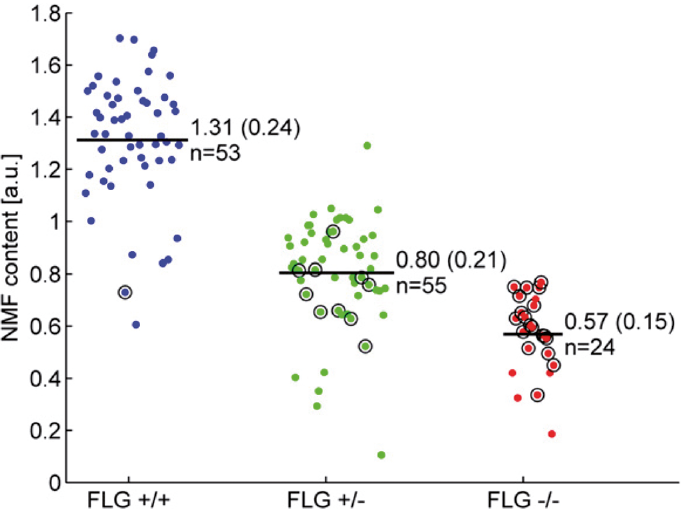 Click to show fullsize
Click to show fullsize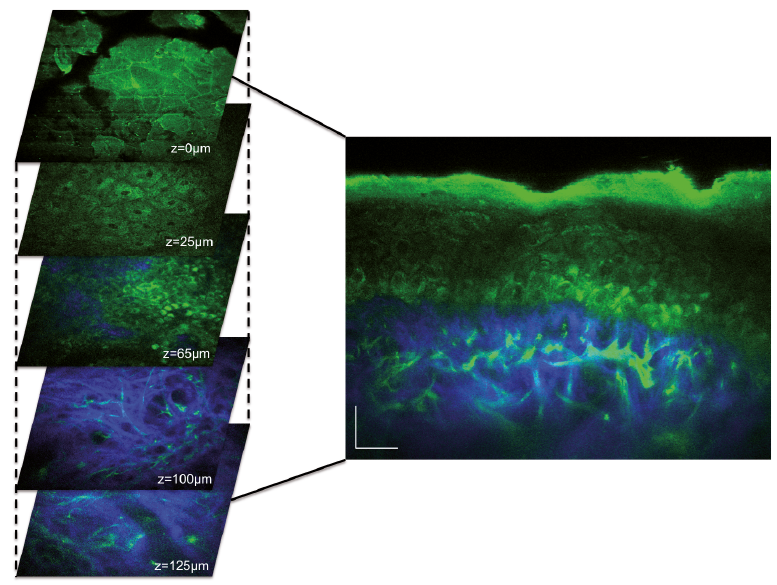 Click to show fullsize
Click to show fullsize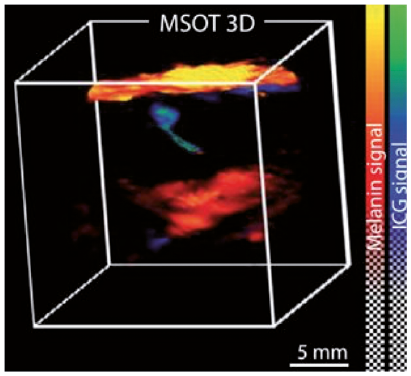 Click to show fullsize
Click to show fullsize