


Departments of 1Dermatology, 2Hematology and Oncology, and 3Radiology, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya 466-8550, Japan. *E-mail: takeichi@med.nagoya-u.ac.jp
Accepted Jun 8, 2017; Epub ahead of print Jun 9, 2017
The term “abscopal” was defined by Mole in 1953 in the context of radiotherapy as relating to tumour events occurring “at a distance from the irradiated volume but within the same organism” (1). Although the exact mechanism by which the abscopal effect occurs is un-known, several theories have been proposed regarding the abscopal anti-tumour effect (2). Clinical reports of the abscopal effect after radiotherapy are not numerous, although this phenomenon has been detected in several different tumours, including lymphomas, melanomas and various carcinomas (2). For example, there are several reports of the abscopal effect detected in patients with advanced melanoma who were receiving ipilimumab treatment and radiation (3, 4). In addition, Grimaldi et al. (5) reported that administering radiotherapy after melanoma has progressed under ipilimumab treatment may lead to abscopal effects in some patients, and that these responses appear to be associated with prolonged survival. Thus, the abscopal effects of radiotherapy are commonly reported in combination with immunotherapies or chemotherapies. In this report, we describe the useful abscopal effect of topical irradiation, without any combination therapies, to treat lesions distant from the irradiated sites in a patient with diffuse large B-cell lymphoma (DLBCL).
An 88-year-old Japanese male was referred with multiple erythematous eruptions. Physical examination showed a large number of variously sized, circumscribed erythema and nodules on his chest, abdomen and extremities (Fig. 1a–c). He had moderate pain at the largest erythematous nodule (6 × 6 cm2) on the left buttock (Fig. 1c). His history included chronic obstructive pulmonary disease that had been treated with continuous nasal oxygen therapy (O2, 2 l/min), pulmonary hypertension, chronic heart failure, colon polyps, cholelithiasis and hyperlipidaemia. Laboratory tests revealed a white blood cell count of 4,400/mm3 (normal range 3,800–8,500; 57.9% neutrophils, 2.5% eosinophils, 11.3% monocytes, 26.5% lymphocytes and 0% atypical lymphocytes), a haemoglobin concentration of 12.9 g/dl (normal 13–18 g/dl), a platelet count of 231,000/µl (normal 160,000–410,000/µl), soluble interleukin-2 receptor of 1,410 U/ml (normal 124–466 U/ml) and lactate dehydrogenase (LDH) of 747 U/I (normal 119–229 U/I). Positron emission tomography-computed tomography (PET-CT) showed masses on the left buttock and the anterior chest (Fig. S1a, b). In addition, numerous nodules were detected on the lower legs (Fig. S1c). A skin biopsy specimen from the left buttock demonstrated dense infiltration of atypical lymphocytes in the reticular dermis with a grenz zone in the papillary dermis (Fig. S2a, b). Immunohistochemical analyses showed the infiltrating atypical lymphocytes to be positive for anti-CD20, BCL-2 and MUM-1 antibodies, and negative for anti-CD3, CD5, CD10, BCL-6 and TdT antibodies (Fig. S2c–e). In addition, the Ki-67 labelling index was approximately 70% (Fig. S2f).
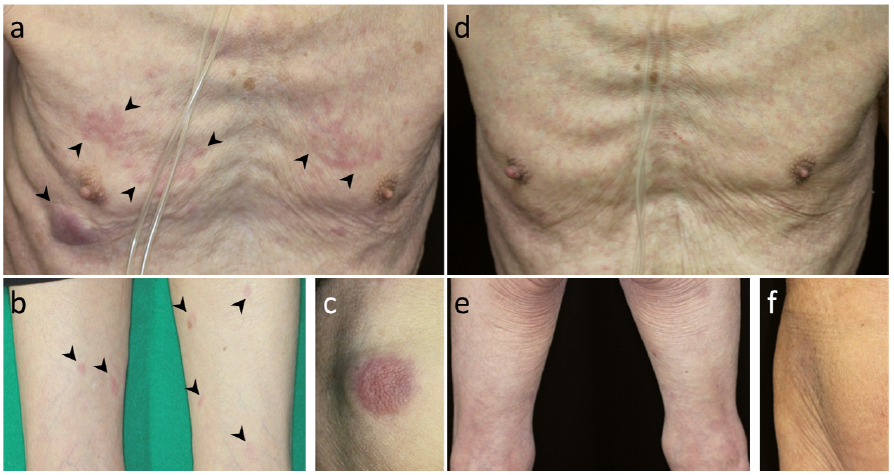
Fig. 1. Cutaneous features of the patient before (a–c) and after (d–f) treatment with local irradiation. (a) An erythematous nodule on the right hypochondrium and multiple small erythemas on the chest. (b) Variously sized pinkish erythemas on the thighs. (c) An erythematous nodule on the left buttock. Arrowheads indicate non-irradiation eruptions. (d–f) After 32 Gy (4 Gy × 8 times) of irradiation to the left buttock and 24 Gy (4 Gy × 6 times) of irradiation to the left upper arm, no eruptions are seen on the non-irradiated (d) chest, (e) thighs and (f) left buttock.
The patient was diagnosed with cutaneous involvement of DLBCL, non-germinal centre B-cell-like (GCB) type. Given the patient’s general condition, we started local irradiation treatment as palliative care. He received fractionated irradiation to the left buttock (4 Gy × 8 times) and the left upper arm (4 Gy × 6 times). Surprisingly, one month after these treatments, all eruptions including those in non-irradiation areas disappeared completely with normalization of the serum LDH levels (Fig. 1d–f). The disappearance of non-irradiated eruptions was also confirmed by computed tomography (CT) images 3.5 months after the irradiation treatment (Fig. S1d). Al-though the patient had been disease-free for 6 months from the irradiation, a few erythemas appeared on the abdomen, accompanied by elevated serum LDH levels. Nine months after the radiation treatment, the patient died, probably due to recurrence of the lymphoma.
The patient was diagnosed with non-GCB DLBCL (stage I, without B-symptoms) (6). In 2008, DLBCL was classified by the WHO as an aggressive lymphoma. Therefore, spontaneous regression of DLBCL is extremely rare. In the present case, simple palliative fractionated irradiation produced an abscopal effect on remote lesions and improved the patient’s prognosis. To our knowledge, this is the first report of palliative radiotherapy having an abscopal effect on DLBCL. In the literature, the median time from radiation therapy to a documented abscopal response was 5 months (range < 1–24 months) (7). Our case showed the abscopal response one month after irradiation, which is earlier than in the previous reports.
Levy et al. (8) reported that the biological mechanisms of the abscopal effect are thought to rely on the ability of radiation therapy to elicit an immune response. In brief, irradiated tumours release danger signals, which activate dendritic cells (DC) (8). Radiation therapy can also induce a dose-dependent increase in major histocompatibility complex (MHC) class I presentation in human tumour cells, leading to tumour recognition (8). Activated DC can then prime T cells and cause an appropriate level of CD8+ T lymphocyte cytotoxicity (8). Although it is not easy to clarify the abscopal mechanism in the current case, we speculate that immune responses induced by the radiation therapy and might have caused the remote tumours to be attacked.
The case reported here showed disease recurrence 6 months after irradiation. Levy et al. (9) noted that the abscopal effect rarely remained for a long period when radiation therapy was used alone. Indeed, the high frequency of in-field and distant relapses in locally advanced tumours treated with irradiation alone suggests that this radiation-induced anti-tumour immunity is inadequate and remains to be improved in order to obtain a long-term anti-tumour effect (9). In conclusion, the current case suggests that the abscopal effect of radiotherapy may also be possible in DLBCL.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize