


1Department of Dermatology, Tel Aviv Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, 2Central Compounding Laboratory, Petach-Tikva, and 3Department of Human Molecular Genetics & Biochemistry, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Limited efficacy, costs, side-effects and complications are issues of concern for most current therapeutic modalities for focal hyperhidrosis. This study evaluated the efficacy of topical oxybutynin 10% gel in treating 61 patients with primary focal hyperhidrosis. The gel was applied to the right or left axilla, palms or soles vs. a placebo compound to the contralateral side for 30 days. A blinded visual grading of the change in starch-iodine tests was performed by 2 non-involved physicians. The Hyperhidrosis Disease Severity Scale (HDSS) and Dermatology Life Quality Index (DLQI) questionnaires were administered before and after treatment. The patients rated their satisfaction with treatment. Fifty-three patients completed the 4-week treatment. Sweat reduction in the drug-treated sweating areas was higher than in the control-treated areas. There was a significant mean improvement in pre- and post-treatment HDSS and DQLI (p = 0.001 for both). Thirty-nine subjects (74%) reported moderate-to-high satisfaction. Twice-daily topical application of oxybutynin 10% gel appears to be an effective, safe and well-tolerated treatment for focal primary hyperhidrosis.
Key words: focal hyperhidrosis; axillary; palmar; plantar; topical oxybutynin.
Accepted Jun 22, 2017; Epub ahead of print Jun 27, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Ofir Artzi, Department of Dermatology, Tel Aviv Medical Center, 6 Weizman Street, Tel Aviv, 6423906, Israel. E-mail: ofira@tlvmc.gov.il
Hyperhidrosis is a common condition, affecting up to 3% of the population, and has a significant impact on many aspects of the affected individual’s life (1–3). Primary hyperhidrosis manifests mainly in the axillae, palms, soles and facial regions (3). Treatment options include surgical interventions (e.g. surgical en bloc excision, liposuction or endoscopic thoracic sympathectomy) and non-surgical modalities, such as topical drugs, botulinum toxin injection, systemic drugs, iontophoresis and energy-based treatments (3). Hypohidrosis is associated with systemic anticholinergic drugs (4), which led to their use as topical agents for hyperhidrosis. For example, topical application of the anticholinergic drug glycopyrrolate (5–10) resulted in focal improvement in sweating, although that effect may have been due in part to systemic absorption of the medication (11–13).
Oxybutynin is another anticholinergic-muscarinic receptor antagonist (14). Topical application of oxybutynin chloride gel has proved effective for the treatment of overactive bladder via transport into the circulation by passive diffusion across the stratum corneum (15). The purpose of the present study was to evaluate the efficacy of oxybutynin chloride gel 10% in the treatment of primary focal hyperhidrosis.
This study was performed at the Tel Aviv Medical Center and approved by the Institutional Review Board. Written informed consent was obtained from all participants prior to entering the study. Sixty-one patients with confirmed primary focal hyperhidrosis who had received no topical or oral anticholinergics, iontophoresis treatment or botulinum toxin injections during the 6 months prior to study entry and had not undergone sympathectomy were recruited. Twenty-two of those 61 patients (36%) had palmar hyperhidrosis, 23 (38%) had axillary hyperhidrosis, and 16 (26%) had plantar hyperhidrosis. Demographic data, including sex, age and medical history were collected before enrolment in the study, and the following patients were excluded: pregnant or lactating women, individuals with conditions that may cause secondary hyperhidrosis, individuals with an active skin disease affecting the treated areas (e.g. eczema, seborrhoea, psoriasis), glaucoma, urinary retention, gastric retention, myasthenia gravis, angioedema, Sjögren’s syndrome, or Sicca syndrome, and candidates > 60 years or < 18 years of age.
The study followed a prospective, randomized, double-blind, placebo-controlled design. Each participant was given a pair of test jars (designated “gel A” and “gel B”). A designated software was used to randomize the jars (either A or B) which contained 10% oxybutynin gel or a placebo aqueous gel. The 2 jars were identical in shape, size and weight, as well as colour, odour and consistency. The patients were instructed to apply 1 cm of gel A or B on clean, dry and intact skin of one sweating area (right or left palms, soles or axillae) twice daily for 30 days. This was estimated to provide 50 mg of active oxybutynin in each application. The patients with axillary or plantar hyperhidrosis were asked to use the contralateral hand to apply the drug/placebo. The patients with palmar hyperhidrosis were instructed to use disposable transparent gloves while applying the drug/placebo. In addition, they were instructed to avoid contact of the gel with the eyes, nose, mouth, and not to wash the areas for 4 h post-application. They were also instructed not to use any concomitant topical or systemic medication during the entire treatment period. Each jar was weighed on a digital scale before treatment initiation and on the 30th day of treatment.
All patients underwent the Minor starch-iodine test (16) on the oxybutynin- and placebo-treated sides. The tested areas were photographed under standard conditions using the Galaxy Camera (3G) EK-GC100 photography system. A blinded visual grading of the photographs taken before and after 30 days of treatment was the primary endpoint. The photographs were independently assessed by 2 dermatologists who were unaware of the study design. All pairs of photographs were graded as 0 = no change, 1 = minor change of < 25%, 2 = moderate change of 25–50%, 3 = major change of 50–75%, and 4 = absence or near absence of sweating.
The patients were interviewed twice; first at the time of screening before the initial application and then following completion of the 30th day of treatment. They were asked to rate the severity of their condition using the Hyperhidrosis Disease Severity Scale (HDSS) (2, 17) in which a score of 3 or 4 indicates severe hyperhidrosis, while a score of 1 or 2 indicates mild or moderate hyperhidrosis. The therapeutic results were considered as “excellent” or “good” if the patient indicated a reduction of 2 or 1 points, respectively, on the HDSS score. In addition, quality of life was assessed with the Dermatology Life Quality Index (DLQI) (2, 18) (permission by Dr A. Finlay). The word “symptomatic” was changed to “sweaty” in the first question to make it more applicable to hyperhidrosis. The DLQI is a validated 10-item questionnaire on leisure, personal relationships, daily activities, and treatment. The maximum score is 30, with 0 indicating a negligible effect of the disorder on the patient’s quality of life and 30 indicating a significant impact. A change of 0–1 points on the DLQI score was interpreted as reflecting no effect on the patient’s life, a change of 2–5 points as a small effect, 6–10 points as a moderate effect, 11–20 points as a very significant modification, and 21–30 points as the most significant impact possible.
At the end of the treatment, patients completed a questionnaire evaluating the following: (i) sweat reduction in the treated and in the control sweating areas (0 = no change, 1 = poor (limited improvement with the patient being very much aware of sweating), 2 = fair (marked improvement, with noticeable sweating under stressful conditions only), 3 = good (marked improvement with minimal sweating under stressful conditions), and 4 = excellent improvement, with cessation of sweating). (ii) Global patient satisfaction (0 = dissatisfied, 1 = partially satisfied, 2 = satisfied, and 3 = highly satisfied). (iii) Side-effects: dry mouth, headache, dizziness, urine retention, constipation and application site reactions (pruritus or dermatitis).
Both the study and control gels were compounded in an Israeli compounding pharmacy. The composition of the study gel was as follows: oxybutynin chloride 10% (active gel) dissolved in ethanol 95%, glycerin, tween-80, medium chain triglycerides oil, apple scent and hypromellose gel. The placebo gel contained the same ingredients excluding oxybutynin chloride.
Continuous variables were fed into a tabular format as means ± standard errors and compared using the Wilcoxon paired test. Categorical variables were tested using the Fisher’s exact test. Correlation between raters was evaluated using Spearman’s correlation. The level of significance was defined as α = 0.05. All analyses were carried out using SPSS 23.0.2.
Twenty of the 22 patients with palmar hyperhidrosis, 21 of the 23 patients with axillary hyperhidrosis, and 12 of the 16 patients with plantar hyperhidrosis completed the 4 weeks of treatment. Forty-one patients (77%) were female and 12 patients (23%) were male. The mean ± SD age of patients ranged from 18 to 52 years (31.6 ± 1.4 years). They reported having hyperhidrosis for 1.5 to 40 years (15.2 ± 1.4 years). Thirty-six patients (67.9%) had never been treated for their condition, 6 (11.3%) had tried several topical anti-perspirants with variable efficacy, and 11 (20.8%) had undergone effective treatment with botulinum toxin injections.
No serious systemic side-effects were encountered during the study period. Two patients reported transient headaches in the first week of treatment. Eleven of the 23 patients with axillary hyperhidrosis reported erythema and pruritus upon applying the study gel. Instructing those patients to wait 2 days between shaving and first use as well as application of the gel on a clean and dry skin at room temperature attenuated these side-effects. Eight of the 16 patients with plantar hyperhidrosis reported that the product was “sticky” and unpleasant to use. A total of 8 patients withdrew from the study for the following reasons: 2 due to time constraints, 2 due to recurrent erythema and itching, and 4 who reported that the product was “sticky” and inconvenient to use. The mean ± standard deviation (SD) consumption per application of the studied material (oxybutynin containing gel) was 41 ± 9.98 mg.
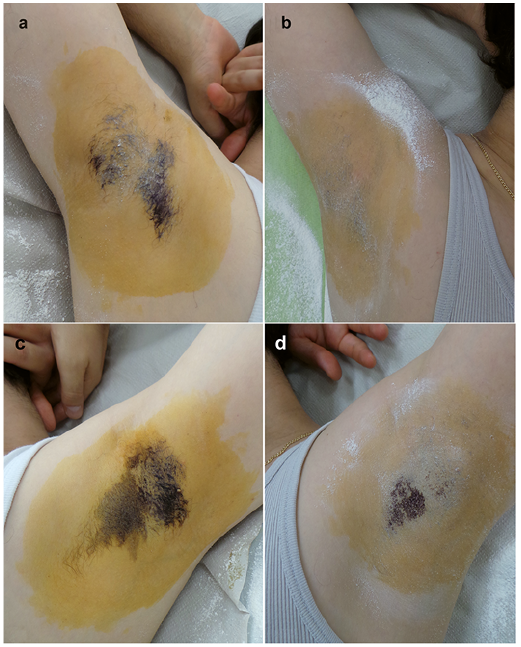
Photographic comparisons (Fig. 1) of the Minor starch-iodine test results before and after 30 days of treatment were blindly evaluated by 2 independent raters. The raters’ evaluations were highly concordant for both the treated and control sides (rsTx = 0.83, p < 0.001 and rsCtr=0.92, p < 0.001, respectively). The mean score for axillary hyperhidrosis in the study gel sweating areas was 3.4 ± 0.2 compared with the control sweating areas (2.5 ± 0.3, p = 0.002). The mean score for palmar hyperhidrosis in the study gel sweating areas was 3.1 ± 0.2 compared with the control sweating areas (1.4 ± 0.3, p = 0.001). The mean score for plantar hyperhidrosis in the study gel sweating areas was 2.9 ± 0.4 compared with the control gel sweating areas (1.9 ± 0.4, p = 0.007).
Fig. 1. Primary focal hyperhidrosis. The Minor starch-iodine test was performed (a, c) before and (b, d) after 30 days of twice daily application of aqua-based (d) placebo gel or (b) oxybutynin 10% gel.
At the end of the study, 42 out of 53 patients (79 %) correctly indicated the side that had been treated by active oxybutynin gel. The patients’ grades for sweat reduction in the drug-treated sweating areas vs. the control-treated sweating areas are shown in Fig. 2. The mean sweat reduction was 2.49 ± 0.1 for the drug-treated area and 1.53 ± 0.1 for the control-treated area (p < 0.001).
Fig. 2. Primary focal hyperhidrosis. Patients’ grade for sweat reduction in the drug-treated compared with the control-treated sweating areas.
A change in perspiration was noted in the treated and control areas as well as in other distant sites (face, back). The changes as reported in the HDSS score are shown in Fig. 3. Most of the patients (66%) reported a 1-point reduction in their HDSS score. The mean DLQI before treatment was 14.9 ± 0.8 (palmar 13.7 ± 1.2, plantar 16.4 ± 2.0, and axilla 15.1 ± 1.4). At the end of the treatment period, the mean post-treatment DLQI was 7.3 ± 0.6 (palmar 6.9 ± 0.9, plantar 8.2 ± 1.4, and axilla 7.2 ± 0.8, p < 0.003) (Fig. 4). Out of the 53 patients who completed the study, 5 (9.4%) reported no change in DLQI, 15 (28.3%) reported a small effect, 18 (34%) reported a moderate effect, and 15 (28.3%) reported a large effect. The change was most noticeable among patients with axillary hyperhidrosis (Fig. 5). Thirty-nine subjects (74%) were moderately to highly satisfied. The degree of satisfaction for the different treated areas is shown in Fig 6.
Fig. 3. Primary focal hyperhidrosis. Changes in the Hyperhidrosis Disease Severity Scale (HDSS) following 30 days of twice daily application of 10% oxybutynin gel.
Fig. 4. Primary focal hyperhidrosis. The Dermatology Life Quality Index (DLQI) ratings at baseline and following 30 days of twice daily application of 10% oxybutynin gel.
Fig. 5. Primary focal hyperhidrosis. Changes in the Dermatology Life Quality Index (DLQI) ratings following 30 days of twice daily application of 10% oxybutynin gel.
Fig. 6. Primary focal hyperhidrosis. The degree of satisfaction in the 10% oxybutynin gel-treated areas following 30 days of twice daily application.
Hyperhidrosis is defined as excessive sweating beyond normal thermoregulatory needs and environmental conditions. It is a relatively common disorder, with a prevalence of 3% in the US (1), and one that significantly impairs the affected individual’s quality of life (2, 3). Treatment of primary focal hyperhidrosis remains challenging. The use of topical agents that occlude sweat ducts, such as aluminium chloride, formaldehyde, glutaraldehyde and potassium permanganate preparations, is limited by short-term effect, limited efficacy and irritation (19–21). The use of oral anticholinergics is associated with systemic adverse effects (4, 22–25). Other oral medications, such as diazepam (25) and clonidine (26, 27), are limited by their neurocardiovascular side-effects. Iontophoresis for the treatment of palmar and plantar hyperhidrosis is time-consuming (3, 28) and might cause several side-effects, ranging from tingling and erythema to painful stinging, itching, blistering and mild electric shock sensations. Injections of botulinum toxin (29–31) for axillary, palmar or plantar hyperhidrosis is efficacious, but entails high costs and pain, in addition to its being potentially linked to possible neurologic side-effects. Surgical procedures (surgical en bloc excision, liposuction or endoscopic thoracic sympathectomy) offer a permanent solution, but are associated with significant and sometimes irreversible side-effects (32–35). Laser- (36–38) radiofrequency thermotherapy- (39) and microwave- (40–43) based therapies have been suggested recently as possible treatment modalities, but data on their long-term efficacy, safety and side-effects are still lacking.
The ideal treatment for primary hyperhidrosis should be one that is simple and non-invasive, with few complications and a low financial burden. Topical anticholinergic agents, such as glycopyrrolate, have had inconsistent efficacy in improving sweating (5–10) and were more effective for the sweating of the craniofacial area than other areas (7). Their effect may be partly systemic due to transdermal absorption and distant effect (11–13). Al-though many systemic anticholinergic adverse effects (dry mouth, blurry vision, constipation, difficulty in urinating, cognitive and memory impairments) can be attributed to oxybutynin, which is another cholinergic-muscarinic receptor antagonist, several peer-reviewed articles that included long-term use reported high levels of safety for its treatment of various pathologies, especially when used orally in low and incremental doses or topically (14, 44–49). Topical application of oxybutynin chloride gel is indicated for the treatment of overactive bladder where its effect is due to systemic absorption (15).
The current study evaluated a topical formulation of oxybutynin for the treatment of primary localized axillary, palmar or plantar hyperhidrosis. We found that a twice daily application of 10% topical oxybutynin gel resulted in a significant reduction in HDSS scores and a significant improvement in DLQI scores, as well as being associated with a high rate of patient satisfaction. Objective assessment by means of the Minor starch-iodine assay corroborated the subjective data collected from the patients. Of note, despite the drug having been applied in only one area, the control areas showed improvement according to the assessment of the 2 raters, a finding that could be attributed to the passive diffusion of the gel across the stratum corneum and its systemic absorption.
In conclusion, the present data demonstrated that topical oxybutynin appears to be a safe and efficient therapeutic option for focal primary hyperhidrosis. Follow-up studies are needed to measure the extent of drug absorption as well as to optimize dosage and improve drug formulation.
The authors acknowledge Ms Dvora Cohen, Ms Shimrit Tradion and Shoshi Zilber for their assistance in patient recruitment. Esther Eshkol is thanked for editorial assistance.
Conflicts of interest: At the time of study, E. Zur was the compounding pharmacist and scientific manager of the compounding pharmacy that manufactured the topical gels for the trial. However, he was not involved in the trial operation and declares no conflict of interest.


 Click to show fullsize
Click to show fullsize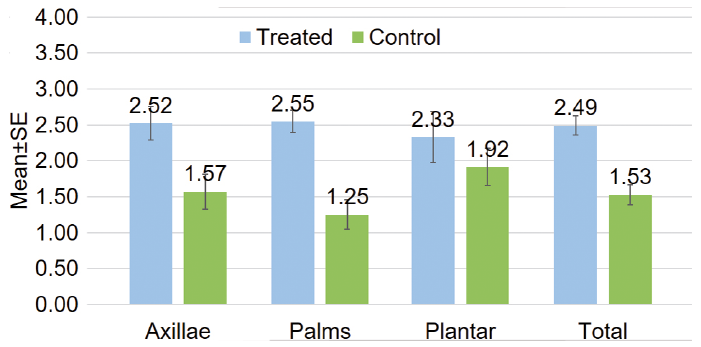 Click to show fullsize
Click to show fullsize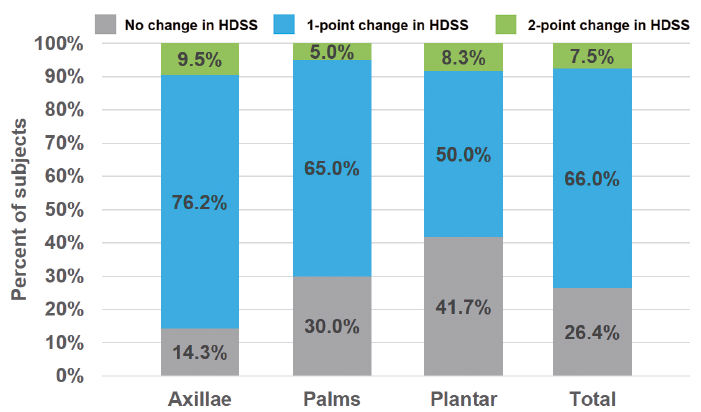 Click to show fullsize
Click to show fullsize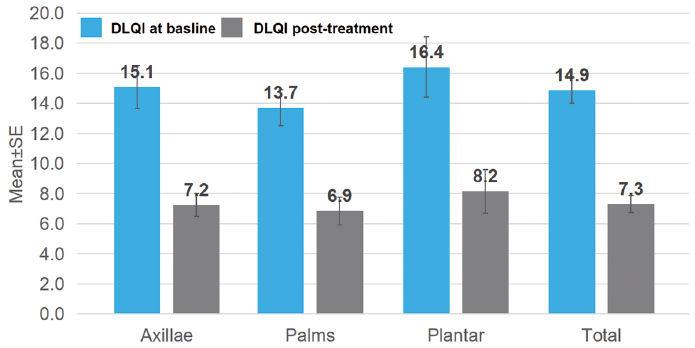 Click to show fullsize
Click to show fullsize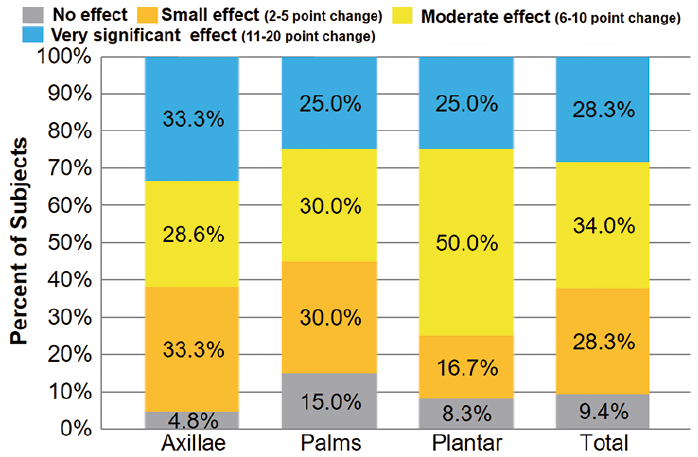 Click to show fullsize
Click to show fullsize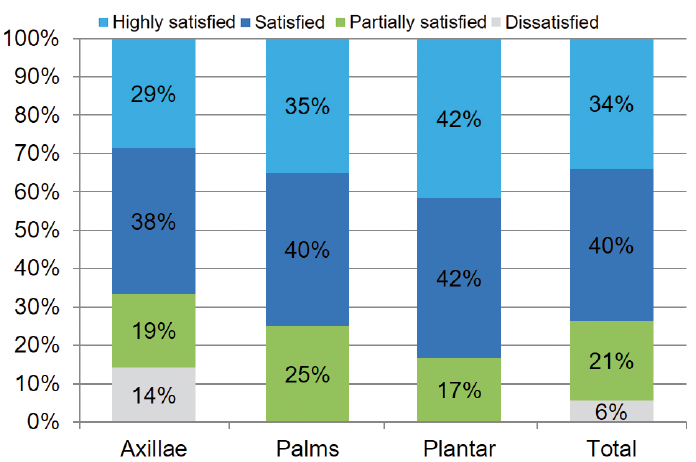 Click to show fullsize
Click to show fullsize