


1Department of Dermatology, Hokkaido University Graduate School of Medicine, North 15 West 7, Kita-ku, Sapporo 060-8638, and 2Maruyama Kouen Skin and Cosmetic Surgery Clinic, Sapporo, Japan. *E-mail: izumi55kentaro@yahoo.co.jp, natsuga@med.hokudai.ac.jp
Accepted Jul 5, 2017; Epub ahead of print Jul 6, 2017
Cutis verticis gyrata (CVG) is an unusual scalp condition characterized by the presence of convoluted folds and furrows that resemble the cerebral cortex. CVG is classified into 2 general groups: primary and secondary CVG (1). We describe here a male patient with secondary CVG associated with atopic dermatitis (AD).
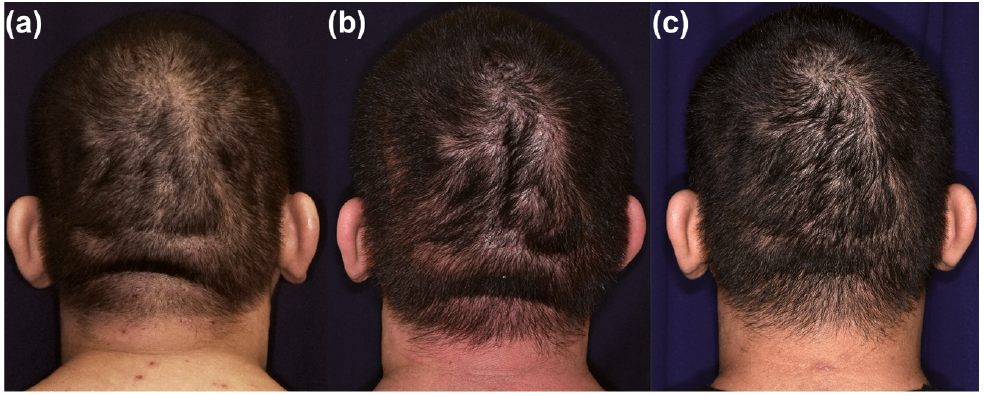
A 23-year-old man was referred to our hospital for treatment for atopic dermatitis (AD). The eruptions were consistent with AD, except for a 3-month history of scalp thickening. On physical examination, his occipital scalp was found to form circumferential and sagittal folds, which had a cerebriform appearance (Fig. 1a). He had no history of disease, including congenital disorders or mental retardation. Neither internal malignancies nor orthopaedic abnormalities were detected on computed tomography (CT) scanning or magnetic resonance imaging (MRI). Detailed examination revealed no endocrinological disturbance. The human immunodeficiency virus (HIV) antibody test was negative.
Fig. 1. Scalp thickening fluctuated with the disease activity of atopic dermatitis (AD). (a) The scalp at presentation. (b) The folds became thickened when the patient’s AD worsened. (c) The elevated scalp became flattened after 3 weeks of topical steroid therapy for AD.
His scalp folds became thickened when the AD activity worsened (Fig. 1b) and thereafter gradually became flattened after 3 weeks of topical application of betamethasone butyrate propionate lotion to the head to treat the AD (Fig. 1c). We advised him to continue with intermittent topical corticosteroids after complete remission of AD, as a proactive therapy.
Secondary CVG appears with numerous aetiologies. The associated conditions include congenital diseases (including Turner syndrome, Klinefelter syndrome, and Noonan syndrome) (1), scalp tumours and hamartomas (1, 2), internal malignancies (1), endocrine abnormalities (including acanthosis nigricans, acromegaly, myxoedema, and Graves’ disease) (1, 3), HIV-related lipodystrophy (4), and inflammatory dermatoses (including chronic eczema, atopic dermatitis, psoriasis vulgaris, and folliculitis) (1, 5).
The aetiology of CVG is largely unknown, and it is generally considered that the underlying mechanisms differ with regard to each associated factor (1). For CVG associated with inflammatory dermatoses, it is hypothesized that inflammation of the scalp leads to the corrugation; however, the details of pathogenesis of post-eczematous CVG are unknown (1, 6).
The treatment of secondary CVG should be directed at the underlying condition; however, it seldom improves the deformity of the scalp except for post-eczematous CVG (1). Thus, some cases need scalp reduction procedures for cosmetic reasons (7).
Clinicians should be aware that post-eczematous CVG, in contrast to the other aetiologies, can quickly be flattened with the treatment of causal dermatitis, which should benefit the patients who have disease-related cosmetic issues.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize