


1Hidrosis Clinic, Stockholm, and 2Department of Medical Sciences, Dermatology and Venereology, Uppsala University, Sweden
Studies on children with hyperhidrosis are sparse. This retrospective study presents clinical data and quality of life, along with treatment effect and safety of botulinum toxin (BTX). Case reports from 366 children were included to capture the medical history of hyperhidrosis. The total median score of the Dermatology Life Quality Index before treatment was 11 for children aged 16–17 years and 12 for children younger than 16 years. The children described physical, psychosocial and consequence-related symptoms. More than 70% had multifocal hyperhidrosis. BTX-A and/or BTX-B were given to 323 children, 193 of whom received repeated treatments. The highest score in a 5-grade scale concerning treatment effect was reported by 176/193 children, i.e. their “sweating disappeared completely”. No severe adverse events occurred. Focal and multifocal hyperhidrosis in children reduces quality of life considerably. Treatment with BTX-A and/or BTX-B has been performed with success.
Key words: hyperhidrosis; children; botulinum toxin; botulinum toxin type A; botulinum toxin type B; quality of life.
Accepted Jul 31, 2017; Epub ahead of print Aug 1, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Carl Swartling, Hidrosis Clinic, Warfvinges väg 35, SE-112 51 Stockholm, Sweden. E-mail: carl.swartling@svedklinikken.dk
*This study was published as an abstract and a poster at the international conference TOXINS 2017: Basic Science and Clinical Aspects of Botulinum and Other Neurotoxins in Madrid, Spain on January 18–21, 2017.
Primary focal and multifocal hyperhidrosis is a paediatric inherited disease with diagnostic criteria (1). Hyperhidrosis localized on the palms, feet and axillae is thought to be due to low thresholds to arousal in the limbic system and frontal cortex. Hyperhidrosis in the craniofacial area, trunk, inguinal region and limbs may result from low thresholds to heat/effort in the “thermostat” hypothalamus (2).
The prevalence of the disease has been estimated as 2.8% in a large American epidemiological study (3). Although the prognosis is unknown, our experience is that the condition is chronic in most cases, but that the phenotype may change over time. For example, palmoplantar hyperhidrosis in youth can change to excessive sweating from head-trunk in middle age.
Primary hyperhidrosis is a stigmatizing disease with physical, psychosocial and consequence-related symptoms. Quality of life (QoL), measured with the Dermatology Life Quality Index (DLQI), is severely affected in adults with hyperhidrosis, with results comparable to the most severely affected patients with psoriasis and isotretinoin-treated acne (2). Many elderly people with hyperhidrosis remember their childhood and youth as a troublesome period with respect to the disease, but there is little reference in the literature to QoL in children with hyperhidrosis (4, 5).
First-line treatment of focal hyperhidrosis of the palms, feet and axillae is with an antiperspirant containing aluminium chloride. Second-line treatment is multiple local injections of botulinum toxin type A (BTX-A) and botulinum toxin type B (BTX-B) over the areas affected by excessive sweating (2). Although primary focal hyperhidrosis is a paediatric disease, nearly all studies on BTX in hyperhidrosis have been performed on adults. However, BTX can be used in cerebral palsy (CP) from the age of 2 years, and primary hyperhidrosis in the axillae, cervical dystonia and blepharospasm/hemifacial spasm can be treated from the age of 12 years with Botox® (Allergan, Irvine, CA, USA).
Adverse events due to the use of BTX in the treatment of hyperhidrosis are few, local and temporary. Muscle weakness, i.e. impaired grip function or stiff forehead, is reported in the treatment of palms or head. Another reported adverse event is compensatory sweating in non-treated areas. By contrast, less sweating from non-injected areas has been reported.
BTX-B is a novel treatment for hyperhidrosis and has been used in the forehead/central face and over the thenar eminence to avoid muscle weakness (6, 7).
Other treatment options for focal hyperhidrosis are miraDry® (Miramar Labs, Sunnyvale, CA, USA), ionto-phoresis, anticholinergics, and surgery. According to guidelines from The National Board of Health and Welfare in Sweden, endoscopic thoracic sympathectomy (ETS) is the final option when all other anhidrotic treatments have failed (8).
The purpose of this retrospective 2-year study is to present clinical data, QoL, treatment effect and adverse events for children who visited the Hidrosis Clinic in Stockholm during 2009 to 2011.
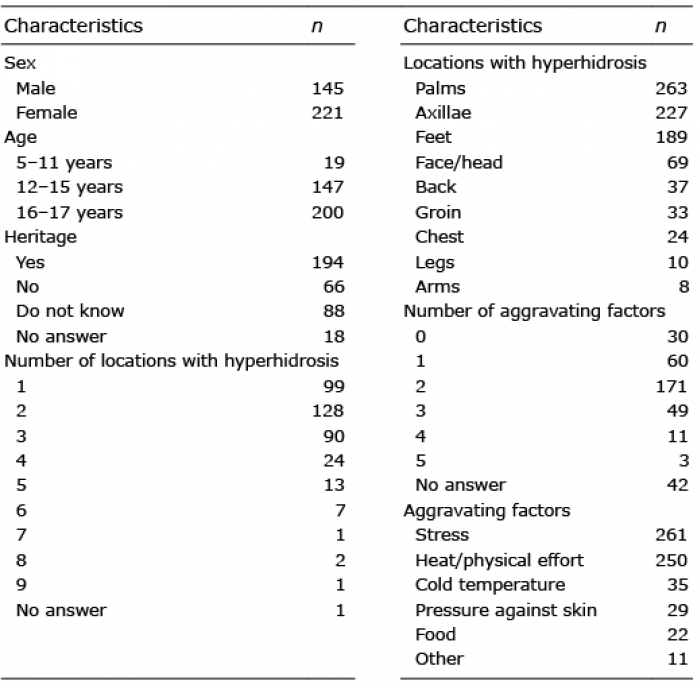
A retrospective study using medical chart notes from children visiting the Hidrosis Clinic, Sophiahemmet Hospital, Stockholm was conducted between 1 September 2009 and 31 December 2011. The criterion to be included in the study was that the child had to be under the age of 18 years at their first visit to the clinic. The exclusion criterion was absence of hyperhidrosis diagnosis at the visit. During the study period 370 children attended the clinic and met the criteria. Four children were excluded from the study due to incomplete medical chart notes, thus 366 children were included. Background data concerning the children are shown in Table I.
Table I. Characteristics of the study population: 366 children with hyperhidrosis
The children were identified by the administrative system used at the clinic (SKALPELL®, Metodika AB, Sweden). The study was approved by the local ethics committee in Stockholm.
The primary objective for this study was to determine QoL for children with hyperhidrosis aged 16–17 years old. The primary endpoint was the total score in the DLQI before treatment with BTX.
Secondary objectives were to determine QoL for children of all ages before treatment with BTX; to survey the pattern of sweating and aggravating factors for children with hyperhidrosis at different ages; to determine the circumstances and symptoms negatively affecting the child’s life due to the disease; and to present the effect and adverse events after treatment with BTX, as well as anaesthesia methods used before treatment.
Secondary endpoints were the total score in the DLQI questionnaire before treatment with BTX for all included children; the amount of free comments reported by the children, distributed in 10 different domains; frequencies of different anaesthesia methods used before BTX treatment; the score in the Global Assessment of Therapy; the duration of treatment effect after injections of BTX; and the rate of adverse events after BTX treatment.
In relation to the first consultation at the clinic, all children were asked to answer the DLQI questionnaire, which consists of 10 questions with a maximum score of 30. The result of the questionnaire can easily be translated into the effect the skin condition has on QoL, using a banding system (0–1 no effect, 2–5 small effect, 6–10 moderate effect, 11–20 very large effect and 21–30 extremely large effect) (9). The adult version of the DLQI is validated from the age of 16 years, but was also used in children < 16 years of age.
Furthermore, the children answered a questionnaire routinely used at the clinic containing questions about inheritance, number of areas of excessive sweating, aggravating factors, and free comments describing the burden of the disease.
The free comments have been categorized into 10 different domains, shown in Table SI. The domains were created in relation to the present study with support from a pilot study performed at the Hidrosis Clinic, in which 50 children’s medical chart notes and questionnaires were reviewed. In the pilot study several re-occurring adjectives and phrases were identified in the children’s free comments. The frequency of each adjective and phrase was counted and summarized in a table and the 10 domains were created at a panel meeting by physicians working at the Hidrosis Clinic, who had substantial experience in the field of hyperhidrosis.
The treatment varied depending on the location/locations to treat. Furthermore, the BTX-A product used at the clinic differed due to tendering.
Intradermal injections of BTX were given in a square pattern, with 12–15 mm between injections, using Xeomin® (Merz Pharmaceuticals, Frankfurt, Germany) 20 units/ml, 1.5–2 units per injection or Dysport® (Ipsen, Slough, UK) 100 U/ml, 3 units per injection and/or NeuroBloc® (Eisai, Hatfield, UK) 250 U/ml, 5–7.5 units per injection.
When anaesthesia was required, the most appropriate method was used depending on the location treated, the age of the child, and their individual pain threshold. Regional anaesthesia was performed in some of the patients with palmar hyperhidrosis, using mepivacaine (Carbocain®, Astrazeneca, Södertälje, Sweden) 10 mg/ml, 3–5 ml at the ulnar and median nerves at the wrist. Intravenous regional anaesthesia using low tourniquets and prilocaine (Citanest®, Astrazeneca) 5 mg/ml, 0.8 ml/kg max 70 ml was performed when treating palmar and plantar hyperhidrosis (10). Topical anaesthesia, lidocaine/prilocaine (EMLA®, Astrazeneca) was, when needed, 60 min before injections when treating the axillae and groin. Alfentanil (Rapifen®, Janssen, Sollentuna, Sweden) 0.5 mg/ml, 1–3 ml was given when required. General anaesthesia was given in some cases.
Information concerning BTX treatment was collected from the medical charts. Reported adverse events and duration of effect could be captured only for the children who had received repeated treatments with BTX, since this was stated by the child or his/her parents at the subsequent treatment session. Furthermore, the score in the 5-grade scale Global Assessment of Therapy was captured; 1 = no effect at all, 2 = slight but insufficient reduction of sweating, 3 = moderate but insufficient reduction of sweating, 4 = marked reduction, residual sweating acceptable, 5 = sweating disappeared completely (11). The chart notes from the first and second treatments were used.
Descriptive statistics have been used throughout the study. Calculations were performed in Microsoft Excel.
More than 70% of the children had multifocal hyperhidrosis (Table I). Approximately 60% had hyperhidrosis at 2 or 3 bodily locations, with the most common combination being the axillae and palmoplantar regions. As seen in Fig. 1; the pattern of sweating commonly involves palmoplantar regions before and during early puberty, continuing with an increased rate of axillary hyperhidrosis in ordinary puberty, with additional locations being the face/head, back, groin, chest, legs and arms during late adolescence. The additional locations (non-palmoplantar or axillary) increased from 9% (< 12 years) to 15% (12–15 years) to 26% (16–17 years) of the focal areas with excessive sweating.
Fig. 1. Relationship between body locations with excessive sweating. Before and in early puberty (<12 years) 19 children reported excessive sweating from 35 body locations, in ordinary puberty (12–15 years) 147 children reported excessive sweating from 336 body locations, and in late adolescence (16–17 years) 200 children reported excessive sweating from 490 body locations. The sum of all hyperhidrotic locations is 100% in each age interval. Note the increase in bothersome sweat production from the axillae and groin, in relation to late adolescence.
For the group in total; the locations most frequently affected by hyperhidrosis were palms (n=263), axillae (n = 227), and plantar area (n = 189) (Table I).
The mean ± standard deviation (SD) reported age for hyperhidrosis debut was 11 ± 3 years (n = 327).
Eighty percent of the children specified at least one aggravating factor, the most common ones being stress and heat/physical effort (Table I).
A total of 304 children had answered the DLQI questionnaire. The median (IQR) total score of the DLQI before treatment for children aged 16–17 years was 11 (8–15) and for children younger than 16 years the total score was 12 (7–15). DLQI scores for different groups and ages are further presented in Table II. The median DLQI total score indicated that hyperhidrosis has a “very large effect” (9) on QoL for males and females in total, regardless of age.
Table II. Dermatology Life Quality Index (DLQI) score by sex and age in 304 children
The investigation of QoL with DLQI was accompanied with free comments from patients (n = 325) who responded to the questionnaire. After analysing all free comments, a pattern of answers could quickly be placed into 10 domains: negative self-esteem, inhibited physical and social contacts, problems with clothing, and practical impact on school work were the most reported complaints. The number of individuals who had provided free comments that were placed in the 10 different domains is shown in Fig. 2.
Fig. 2. Number of individuals who provided free comments in one or several of the 10 domains. The children report low self-esteem with impact on clothing as well as physical and social contact. Furthermore, the disease affects practical situations, for example school work.
A total of 323 children, mean age 15 ± 2 years (age range 5–17 years), had received at least one BTX treat-ment. Details concerning used anaesthesia methods and BTX products are shown in Table SII; however, 8 children are not included in this section due to incomplete treatment (n = 2), exact dose of BTX is missing (n = 3) and anaesthesia method is unclear in the case report (n = 3). During the study period, 196 children had been given treatment in the palms; 191 axillae; 22 feet; 27 face/head; 6 back; 4 groin; 2 chest; and 5 in other locations.
Furthermore, 193 children had received repeated treat-ments (84 children: 2 treatments; 39: 3 treatments; 22: 4 treatments, 19: 5 treatments; 14: 6 treatments, 5: 7 treatments; 5: 8 treatments, 4: 9 treatments; and 1 child: 10 treatments), with a total of 673 treatments. No severe adverse events were reported from these 673 treatments, but 46 children reported 52 adverse events; local muscle weakness (n = 36), compensatory sweating (n = 7), dryness (n = 4), bruises (n = 3), increased feeling of warmth in the body for a couple of days (n = 1), and tenderness in one axillae for 2 days (n = 1).
The score in the Global Assessment of Therapy scale after BTX injections was reported by 183 children at the subsequent visit. Of these children, 176 scored the treatment effect as 5, i.e. sweating disappeared completely. Seven children scored the treatment effect as 1, 2 or 3, i.e. they had insufficient reduction of sweating.
A total of 182 children had stated the time for which they were completely satisfied with the treatment, i.e. completely dry (Table III).
Table III. Time for complete treatment satisfaction, i.e. complete dryness, after botulinum toxin injections (n = 182)
This study confirms that hyperhidrosis is a paediatric disease with a highly negative impact on QoL. The mean DLQI score for all children, as well as for children over 16 years of age, was higher than 11, which is defined as a “very large effect” on QoL (9). Children with hyperhidrosis thus suffer as much as adults or patients with severe psoriasis and acne (2, 12). Even though DLQI is a validated instrument in children from the age of 16 years, we also used the adult version of the questionnaire in younger children with similar results. The adult version of DLQI seems to be adequate in children under 16 years of age; however, there might be a risk of underestimation of the total score. The activities and expressions in the Children’s Dermatology Life Quality Index (CDLQI) are adjusted to suit younger children; thus, the impact on sexual activity is not included.
The results of the DLQI were accompanied by free comments, which could be registered in physical, psychosocial and consequence-related domains. Examples of physical symptoms are cold hands, wet clothes and eczema. Wet, cold parts of the body are impractical and uncomfortable, but, more importantly, stigmatizing leads to psychosocial symptoms, such as low self-esteem and consequence-related symptoms. Avoidance of social events, career opportunities, jobs or meeting a partner are illustrations of consequence-related symptoms mentioned by the children. Some children told us about low performance in school secondary due to hyperhidrosis. It would be desirable to create a more specific questionnaire for patients with hyperhidrosis, which captures physical, psychosocial and consequence-related symptoms.
Hyperhidrosis is considered as a disease of shame. Patients are often too ashamed to express their true feelings about the burden of the disease to physicians, partners, parents, etc. Consequently, there will be a risk that the physicians underestimate and misunderstand the burden of hyperhidrosis. Only 38% of people with the condition seek professional help (3).
BTX is used from 12 years of age in several diseases, including hyperhidrosis, and from 2 years of age in CP. However, many hyperhidrosis guidelines worldwide exclude treatment of children with BTX due to lack of information regarding safety, even though small children with CP have been given BTX for several years. It is important to bear in mind that hyperhidrosis severely affects QoL in children with the disease, but that the possible risks of treatment must always be discussed with the child and his/her parents.
Glaser et al. (13) have investigated the efficacy and safety of onabotulinumtoxinA in adolescents with primary axillary hyperhidrosis. They used QoL measures and found that health outcomes improved markedly.
In total, 803 BTX treatments were administered safely in this retrospective 2-year study, without serious adverse events. Repeated treatments were performed in 193 children. The results truly encourage physicians to treat children of all ages on different areas of the body, even though BTX is only approved by the medical authorities for one area, namely axillary hyperhidrosis.
Some dermatologists hesitate to give multiple injections to children because of the difficulty of administering proper anaesthesia. With the exception of axillary hyperhidrosis, treatment of other locations demands good skills in anaesthesia or, in some cases, requires an anaesthesiologist. However, most treatments can be performed without a physician present in the room, but with a trained nurse and a physician present at the clinic. Special considerations were made to eliminate pain during treatment and to avoid local muscle weakness in the treatment of hands and forehead. It is important that the physician can offer different types of anaesthesia in the treatment of children, including general anaesthesia.
BTX-A is the first option for all children when possible. BTX-B is used when the amount of BTX-A solution is insufficient to cover large areas, such as the trunk, or for multifocal hyperhidrosis. It is also used in the forehead and over the thenar eminences of the palms to avoid muscle weakness. Some of the children do not have any effect of BTX-A, but respond well to BTX-B. The usage of BTX-B is consequently important to be able to help all children.
Based on previous studies (6, 7, 14) diluted BTX-B may be given in relatively small doses when treating hyperhidrosis, almost equivalent to the doses of BTX-A (Table SII). The amount of protein is higher in NeuroBloc® (BTX-B) compared with the BTX-A products; however, the median doses used in this study was 250 units for small areas, such as the thenar eminences and 3,625 units for multifocal hyperhidrosis. When treating cervical dystonia doses of approximately 5,000–20,000 units are used. In some children 3 locations were treated successfully on the same day; for example, palmoplantar + axillary areas, using BTX-B. According to the results of this study, multifocal hyperhidrosis is more common than focal, and the need for treatment of several areas of the body supports the use of BTX-B.
The median time for which the children were completely satisfied with the treatment, i.e. completely dry, is shown in Table III. Many children also experienced partial effect for further weeks or even months; however, the exact time was not specified in the case reports.
In conclusion, focal and multifocal hyperhidrosis is a paediatric disease associated with severe negative QoL, which can be treated successfully with BTX-A and/or BTX-B with few and temporary adverse events. A prospective study would be valuable to confirm these results.
Conflicts of interest. CS is a shareholder in Hidroskliniken i Sverige AB. The other authors have no conflicts of interest.


 Click to show fullsize
Click to show fullsize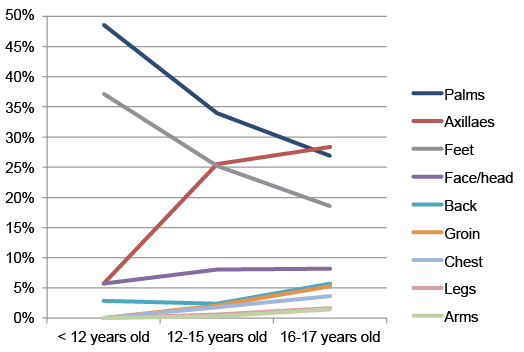 Click to show fullsize
Click to show fullsize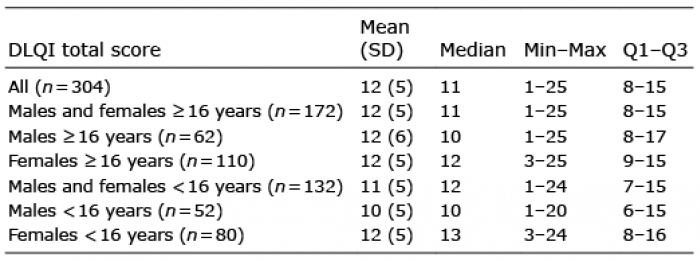 Click to show fullsize
Click to show fullsize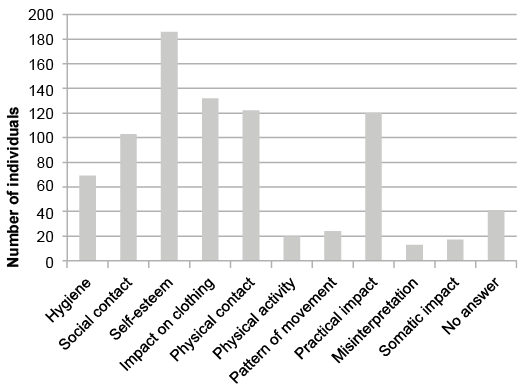 Click to show fullsize
Click to show fullsize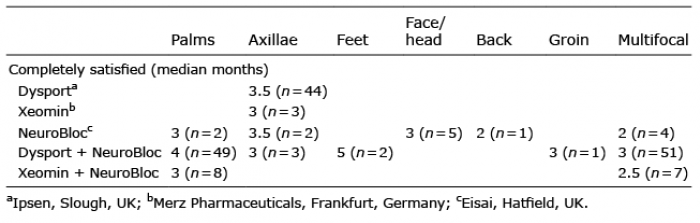 Click to show fullsize
Click to show fullsize