


1Department of Dermatology and Venereology, Institute of Clinical Sciences at the Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden, and 2Cancer Control Group, QIMR Berghofer Medical Research Institute, Brisbane, Queensland, Australia
The incidence rates of thin melanomas (≤1 mm Breslow thickness) have increased in many fair-skinned populations, prompting a need to better identify patients with thin melanomas who will eventually die from the disease. This study aimed to describe the clinicopathological characteristics of lethal melanomas in Western Sweden, with a focus on thin lesions. Population-based data on invasive melanomas diagnosed during the years 1990 to 2014 were extracted from the Swedish Melanoma Registry, and linked to the Swedish Cause of Death Registry. The age-standardized incidence (US population 2000) of thin melanomas increased from 9.1×10–5 (95% confidence interval (95% CI) 8.5–9.8) to 21.3×10–5 (95% CI 20.4–22.1) during the study period. Thin melanomas comprised 55.2% of the total and contributed to 13.5% of all melanoma deaths. Non-ulcerated melanomas 0.76–1 mm and ulcerated melanomas 0.26–1.0 mm showed a poorer survival compared with other thin melanomas.
Key words: cutaneous malignant melanoma; thin melanomas; melanoma survival; histopathological subtype; ulceration; anatomical location.
Accepted Jul 31, 2017; Epub ahead of print Aug 1, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Magdalena Claeson, Department of Dermatology and Venereology, Institute of Clinical Sciences at the Sahlgrenska Academy, University of Gothenburg, SE-413 45 Gothenburg, Sweden. E-mail: magdalena.claeson@vgregion.se
Cutaneous malignant melanoma (melanoma) is a potentially lethal tumour, arising from melanocytes of the skin. Melanoma incidence rates have been rising progressively in fair-skinned populations, primarily due to an increase in thin tumours (≤ 1 mm Breslow thickness) (1–5). The higher proportion of thin melanomas has been attributed both to a true increase in melanocytic neoplasms, as well as to the impact of early detection and public awareness campaigns (1, 6). Melanoma survival is strongly inversely associated with tumour thickness, leading to excellent 20-year survival rates of 96% in patients with thin melanomas (7). Thick lesions (> 4 mm), on the contrary, have a 20-year survival rate of approximately 50% (8). Thus, previous research has partly overlooked thinner tumours and instead focused on thicker melanomas. However, a recent study has shown that more people die from thin melanomas than from thick lesions (> 4 mm) in Queensland, Australia, because thin lesions have become so much more common (9). In that study, approximately a quarter of patients who died from melanoma were originally diagnosed with a thin primary tumour (9). This finding shows the need to better identify, at the time of diagnosis, the subset of patients with thin melanomas who will eventually develop metastases from their primary tumour.
Sweden has a fair-skinned population that experiences a high incidence of melanoma, and a high cost-to-population ratio for skin cancer (5, 10). Not only is the incidence high; male age-standardized rate (ASR) 39.7×10–5, female ASR 35.3×10–5 (Swedish population year 2000), but the annual percentage increase is also greater than 6% (11).
Sweden has a tradition of well-kept cancer registries with high coverage rates, facilitating epidemiological registry studies (12). The western parts of Sweden have, for the past decades, shown a higher incidence of melanoma than the national average, and projections show that this geographical area can anticipate greater numbers of melanoma in the future (13, 14). A few studies have investigated thin melanomas in Sweden, but none have focused on Western Sweden (4, 15–17). The aim of this study was to describe the clinicopathological characteristics of lethal melanomas in Western Sweden during the years 1990 to 2014, with a focus on thin lesions (≤ 1 mm).
In Sweden, there are 6 regions for the organization and quality control of cancer healthcare, each with a centre responsible for the prospective registration of tumours in the Swedish Melanoma Registry. The Regional Cancer Centre West collects clinicopatho-logical data on melanoma patients from the “Western Sweden healthcare region”, which corresponds geographically to the county of Västra Götaland and the northern parts of Halland county. These regions have approximately 1.8 million inhabitants, corresponding to 19% of the national population (18). The reporting is performed both by clinicians and pathologists, resulting in 98% coverage for invasive melanomas (12).
The regional ethics board approved the data collection for this study. Population-based data on all invasive melanomas from 1 January 1990 to 31 December 2014 were extracted. In addition to standard patient characteristics, such as age at diagnosis and sex, the data-set included information on tumour characteristics (date of diagnosis, Breslow thickness, ulceration, histopathological subtype and anatomical location). All of the information on tumour characteristics in this study derived from the Swedish Melanoma Registry data-set and no new review of the histopathology of the included cases was performed. Thus, the study cannot comment on possible incomplete sampling of thin melanomas. Melanomas were categorized into the following groups, according to the patients’ age at diagnosis: < 30, 30–49, 50–59, 60–69 and > 69 years. These age intervals were chosen so that the number of melanoma patients would be reasonably large in all age groups. Melanomas were also categorized depending on their invasion depth, measured in Breslow thickness, according to the American Joint Committee on Cancer (AJCC) classification: T1 (≤ 1.0 mm), T2 (1.01–2.0 mm), T3 (2.01–4.0 mm) and T4 (> 4.0 mm) (8). Thin melanomas were further stratified into categories of 0–0.25, 0.26–0.50, 0.51–0.75 and 0.76–1.0 mm. The melanomas were described as being ulcerated or non-ulcerated according to the histopathological reports. The anatomical location for the melanomas on the body surface was specified in the following 5 categories: head or neck, upper extremity, lower extremity, trunk and, finally hand or foot. Also, the melanomas were categorized according to their histopathological subtypes: nodular melanoma (NM), superficial spreading melanoma (SSM), lentigo maligna melanoma (LMM), acrolentiginous melanoma (ALM) and other subtypes. The date and cause of death for all decedents in our cohort until 31 December 2014 were obtained from the national Swedish Cause of Death Registry.
All data were analysed using R version 3.0.3 (The R Foundation for Statistical Computing, Vienna, Austria). Incidence rates per 100,000 person years (age-standardized to the US population in year 2000) for invasive melanoma were calculated for 5-year time-intervals, both in total and divided by Breslow thickness. Crude incidence rates per 100,000 person years for invasive melanoma were calculated by age groups. Univariate Kaplan–Meier estimates for 10-year melanoma-specific survival were calculated in 5-year time-intervals according to the year of diagnosis of the invasive melanoma from 1990 to 2004. Patients who had their first melanoma from 2005 to 2014 were not included in the melanoma-specific survival analysis, to ensure patients had the potential for at least 10 years of follow-up after first diagnosis with melanoma.
Melanomas were further categorized according to sex, age group (as above), Breslow thickness, ulceration, anatomical location, and histopathological subtype. Missing patient data for 1 variable did not affect inclusion with respect to the other variables. Survival time was defined as the time from the date of diagnosis for the invasive melanoma to the date of melanoma-specific death. Censoring was used to remove patients from the analysis at the time of death from other causes, time of emigration, or at the cut-off date of 31 December 2014, whichever came first.
Patients with multiple melanomas were excluded from the primary analysis in order to remove any uncertainty over which melanoma caused a patient’s death. To determine whether the inclusion of multiple melanomas changed the outcome, 2 alternate analyses were performed. The first alternate analysis was performed on the first invasive melanoma and included patients with multiple invasive melanomas. The second alternate analysis also included patients with multiple invasive melanomas, but was performed on the thickest invasive melanoma.
A Cox proportional hazards regression model was used to compare the melanoma-specific survival between NM and SSM using Breslow-thickness, ulceration and age group as covariates. A Cox proportional hazards regression model was also fitted to compare the melanoma-specific survival of the subgroup of non-ulcerated tumours 0.76–1 mm together with the ulcerated tumours 0.26–1 mm, with the subgroup of non-ulcerated tumours ≤ 0.75 mm, using age group as a covariate. All tests were 2-sided, p < 0.05 was considered statistically significant, and 95% confidence intervals (95% CI) were used.
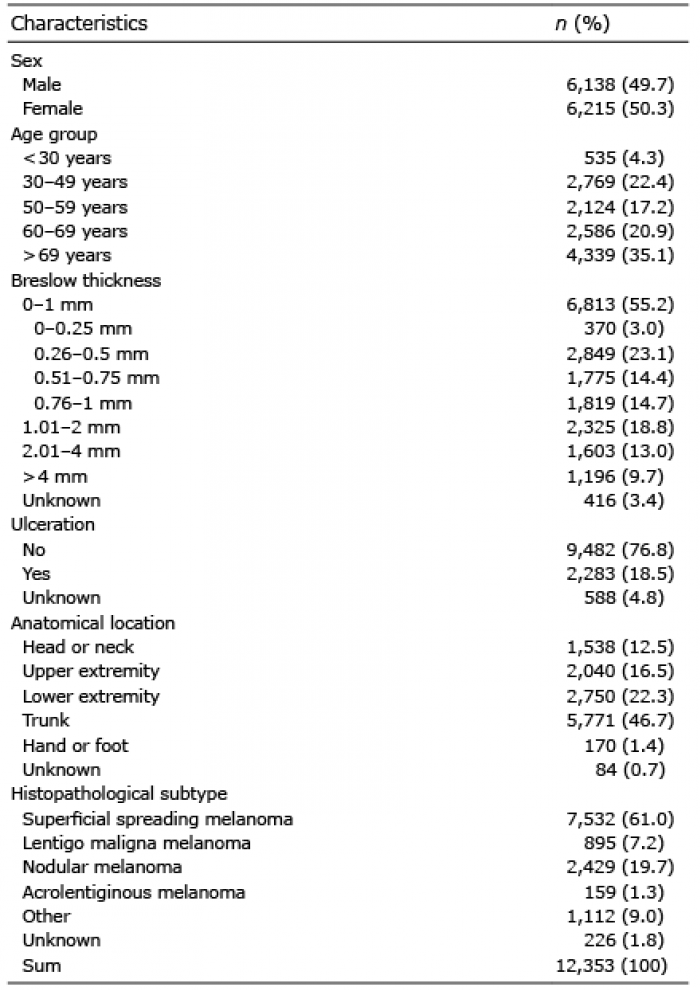
Data extraction yielded 11,700 patients (49.4% men and 50.6% women) and a total of 12,353 invasive melanomas (49.7% tumours on men and 50.3% tumours on women) diagnosed during the years 1990 to 2014. Of all patients, 11,137 (95.2%) developed single invasive melanomas and 563 (4.8%) developed multiple primary invasive melanomas. The median time to death (any cause), emigration or end of the study period in 2014, whichever came first, was 12.0 years. During the years 1990 to 2014, only 29 out of 11,137 patients emigrated to another country. Median age at diagnosis of a first melanoma for all patients in the dataset, was 65 years for men and 60 years for women. Table I shows an overview of the characteristics of all invasive melanomas from 1990 to 2014. The age-standardized incidence (US population 2000) for all invasive melanomas increased steadily from 1990 (ASR 16.6×10–5, 95% CI 15.8–17.4) to 2014 (ASR 36.7×10–5, 95% CI 35.6–37.8). The ASR of thin melanomas increased from 9.1×10–5 (95% CI 8.5–9.8) to 21.3×10–5 (95% CI 20.4–22.1) during the same period. The crude, age-specific melanoma incidence was high-est in the oldest age group (> 69 years), reaching 140.8 (95% CI 133.9–147.7) in the years 2010 to 2014. Table II shows the age-standardized and crude incidence rates in 5-year time-intervals.
Table I. Characteristics of all invasive melanomas in the Western Sweden healthcare region (1990 to 2014)
Table II. Incidence of invasive melanoma in the Western Sweden healthcare region (1990 to 2014), by thickness and age groups including 95% confidence interval in parentheses
Out of the 11,137 patients diagnosed with a single invasive melanoma between 1990 and 2014, 1,221 died from melanoma within the study period (61% men and 39% women). For all decedents, the median and mean times to death were 2.8 and 3.9 years, respectively, with a range of 0.01–22.6 years. The median and mean Breslow thickness for the lethal melanomas was 3.0 mm and 4.4 mm (95% CI 4.1–4.7). Thin melanomas (≤ 1 mm) accounted for 13.5% (165 patients) of all melanoma fatalities, but 55.2% of all invasive melanomas. Meanwhile, thick melanomas (> 4 mm) accounted for 33.1% (404 patients) of all melanoma fatalities, but only 9.7% of all invasive melanomas. Analysis of the data regarding histopathological subtype among all lethal melanomas showed that 49.4% of the decedents in our cohort died from NM, although this subtype comprised only 19.7% of all invasive melanomas. For SSM, the inverse correlation was seen; with 32.3% of the decedents dying from this subtype, which comprised 61.0% of all invasive melanomas.
In terms of melanoma-specific death and survival, only patients with melanomas diagnosed between 1990 and 2004 were included in the analyses, to ensure the potential of at least 10 years of data regarding time to death or emigration. Table SI shows the clinicopathological melanoma characteristics among the patients who died from melanoma within 10 years after diagnosis. Table SII and Table SIII show the clinicopathological melanoma characteristics with respect to the first and the thickest invasive melanomas, respectively, when including patients with multiple melanomas. Only minor differences are seen between Table SI, Table SII, Table SIII.
The overall 10-year melanoma-specific survival for invasive melanomas was 84.1% (95% CI 83.1–85.2), with a survival disadvantage for men at 79.1% (95% CI 77.5–80.9) against women at 88.7% (95% CI 87.4–89.9) (Table SIV). Censoring was performed for patients who died from other causes or emigrated. Survival decreased with age, with the lowest survival in the group of decedents aged over 69 years at diagnosis, at 74.5% (95% CI 72.1–77.0). Thin melanomas (≤ 1 mm) had a very high survival rate of 96.4% (95% CI 95.7–97.1), compared with the low survival rate of thick melanomas (> 4 mm) of 44.3% (95% CI 39.5–49.7). Further stratifying the thin melanomas revealed a low survival for melanomas 0.76–1 mm with a rate of 92.3% (95% CI 90.3–94.3), compared with the survival rate of melanomas 0.51–0.75 mm, which was 96.4% (95% CI 95.0–97.8). Melanomas with ulceration presented a noticeably lower survival of 57.2% (95% CI 53.8–60.7) compared with the survival of non-ulcerated melanomas at 91.1% (95% CI 90.1–92.0).
Combining the prognostic factors of Breslow thickness and ulceration resulted in the Kaplan–Meier survival estimates for lethal melanomas 1990 to 2004 presented in Fig. 1a (all Breslow thickness categories) and Fig. 1b (restricted to tumours ≤ 1 mm Breslow thickness). Fig. 1a shows a very high survival for patients with thin, non-ulcerated tumours, at 96.9% (95% CI 96.2–97.6), but a lower survival for patients with thin, ulcerated tumours, at 86.6% (95% CI 80.3–93.4). Patients with thick, ulcerated (> 4 mm) displayed the poorest survival overall. Fig. 1b shows that non-ulcerated tumours 0.76–1 mm and ulcerated tumours 0.26–1 mm have a lower 10-year survival compared with other thin lethal melanomas, and thus represent a subgroup with a poorer prognosis. The Cox proportional hazards model showed that the survival of the subgroup of the non-ulcerated tumours 0.76–1 mm and the ulcerated tumours 0.26–1 mm together was 92.1% (95% CI 90.1–94.2), which was significantly poorer than for non-ulcerated tumours ≤ 0.75 mm, at 98.1% (95% CI 97.5–98.8) (p < 0.0001). Ulcerated tumours ≤ 0.25 mm were excluded from the analysis, as they were too few in number (no patient in this category died within 10 years).
Fig. 1. Melanoma-specific Kaplan–Meier survival estimates for: (a) all lethal melanomas (0–>4 mm Breslow) and (b) lethal thin melanomas (0–1 mm Breslow) in the Western Sweden healthcare region (1990 to 2004), divided by Breslow thickness and ulceration.
The 10-year survival of patients with melanomas at the hand or foot body sites was low: 53.9% (95% CI 44.2–65.7). Among the 40 patients who died from melanomas located on these body sites, 15 were NMs, 13 ALMs, 6 SSMs and 6 were of Other subtypes. The 10-year survival for head and neck melanomas was also low: 80.0% (95% CI 76.4–83.8). In addition, survival for patients with NMs and for patients with ALMs was poor, at 61.8% (95% CI 58.8–65.0) and 66.7% (95% CI 57.2–77.7) of the patients surviving after 10 years, respectively. In the Cox proportional hazards model, NM showed an independent and statistically significant decreased survival compared with SSM, when controlling for Breslow thickness, ulceration and age group (p = 0.006). For example, for non-ulcerated melanomas with Breslow thickness 1.01–2 mm, NMs showed a 10-year survival of 75.4% (95% CI 69.2–82.2) compared with the survival of SSMs of 88.1% (95% CI 84.7–91.6).
Rapid increases were observed in age-standardized melanoma incidence in Western Sweden from 1990 to 2014. Other studies have projected further future increases in melanoma incidence for Sweden, probably for at least a decade based on current trends (9, 14). For example, a recent analysis predicts an on-going increase until the years 2022 to 2026, before it possibly becomes more stable, similar to how the incidence has reached a plateau in Australia (1, 5). It appears that efforts to reduce mortality from melanoma in spite of increased incidence are now more important than ever.
Recurrent melanoma disease is common in the skin and in the loco-regional lymph nodes, as well as in the form of distant metastases to the lungs, liver, brain or bone. Many studies have investigated clinicopathological factors for distinguishing melanomas with a high risk of metastases and death. The present study confirmed previous findings observing low survival rates among the melanoma decedents with male sex (7, 19, 20), older age (7, 19, 21), increasing tumour thickness (7, 8, 19–23), ulcerated tumours (8, 21, 22), NM (7, 20) and ALM (7, 20) subtypes. Our cohort showed a poor survival for tumours located on the head and neck areas, as well as the hand or foot body sites, whereas other studies only have found poor survival for head and neck tumours (7, 20). Thus, the results concerning survival for melanomas on the hand or foot body sites should be interpreted with caution. In the multiple regression analysis, we found NM to be an independent factor that increased the risk of death from melanoma.
Thin melanomas (≤ 1 mm) were the most commonly diagnosed of all invasive melanomas in the cohort, comprising 55.2% of the total. The 10-year survival fraction for thin melanomas was 96.4%, which is in line with results from other studies (7, 15). Despite their good prognosis, thin melanomas still contributed to 13.5% of all melanoma deaths. Data from Queensland, Australia show that thin melanomas comprised 68% of all melanomas in that state, but caused as many as 23% of deaths in the time-period 2005 to 2009. It appears that the “melanoma epidemic” is more mature in Australia than Sweden, with overall incidence of melanoma now declining in Australia, but with an increasing proportion of thin melanomas. This suggests that primary prevention campaigns to reduce the incidence of melanoma in Australia may be taking effect, coupled with widespread early detection efforts driving a reduction in mean melanoma thickness at diagnosis. Data suggest that early detection may be operating also in Sweden, as evidenced by a growing proportion of thin melanomas, but there is no evidence that primary prevention activities are yet exerting an effect on overall incidence (4).
Thin melanomas have also been shown to account for a large proportion of “Years of life with disability” and “Years of life lost” in the disease burden, although the overall survial rates are very high (24). With increasing incidence, escalating healthcare costs for thin melanomas are to be expected in Western Sweden. If more detailed prognostic factors could be identified, the subset of patients with potentially lethal thin melanomas could be better informed about the prognosis of their disease. Furthermore, they could be kept under closer surveillance with skin examinations, rigorous imaging techniques or lymph node dissection (25). Treatment, such as surgical removal of metastases or new effective adjuvant drug therapies, may also be offered at earlier stages. Such treatments cannot be offered to all patients with thin melanoma, because of high costs and risk of adverse events. Several previous studies have tried to identify adequate prognostic factors for lethal thin melanomas (7, 15, 19–23, 26, 27). In a Swedish study from 2013, Lyth et al. (15) proposed an innovative method of combining prognostic factors to create a classification based on cumulative melanoma-specific mortality. Lyth et al. classified the melanomas in a low-risk group (non-ulcerated, ≤ 0.75 mm and Clark II–III), an intermediate-risk group (non-ulcerated and > 0.75 mm; or non-ulcerated and Clark IV–V; or ulcerated ≤ 0.75 mm and Clark II), and a high-risk group (ulcerated and Clark III–V; or ulcerated, > 0.75 mm and Clark II) (15). Histological information like the Clark level was not available in our particular data-set. Nevertheless, the present study tried to simplify Lyth’s prognostic classification, to make it easier to use in a clinical setting. Therefore, we created a prognostic model, combining only 2 variables for thin melanomas: Breslow thickness and ulceration. The Cox proportional hazards regression analysis resulted in the finding of a significantly poorer survival for ulcerated melanomas 0.26–1 mm and for non-ulcerated melanomas 0.76–1 mm. Thus, our prognostic model identified tumours with these characteristics to be at clinically significant risk of causing death from melanoma. Currently, the Swedish national guidelines for malignant melanoma management do not suggest periodic follow-up for thin, non-ulcerated melanomas ≤ 1 mm (Stage IA). A follow-up frequency of once yearly for 3 years is only recommended for ulcerated melanomas ≤ 1 mm (Stage IB) (25). Hence, there is a high risk of overlooking the potentially lethal thin melanomas in the specific Breslow subgroup of 0.76–1 mm without ulceration. Of the patients diagnosed from 1990 to 2004 in the Western Sweden cohort, 57 patients died from a melanoma of 0.76–1 mm Breslow thickness within 10 years. Non-ulcerated tumours represented 44 of these melanomas, and these patients would thus have been disqualified from regular follow-up. To be able to follow-up closely and intervene in these patients, we therefore propose the possible use of our prognostic model in the future. However, more research focusing on prognostic factors for lethal thin melanomas is needed, and is also planned by our research group.
A strength of this study is the population-based approach, compared with studies from specialized tumour clinics, where patients often present with more advanced tumours leading to higher mortality rates for thin melanomas (15). Also, the Swedish cancer registries are independently acknowledged to report high-quality data (28). There was a low frequency of missing data; for example, the percentage of invasive melanomas without an accurate registration of Breslow thickness was only 3.4%. It was possible to extract data on ulceration from the Swedish melanoma registry, and ulceration is a very important prognostic factor (8). Ulceration data have not been available for analysis for all population-based studies on thin melanomas (7).
This registry-based study has some limitations. The presence of mitosis was not recorded during the entire study period in the Swedish melanoma registry and thus was not included in the analysis. As mentioned above, data regarding the Clark level was not available. Nonetheless, it has been shown that ulceration and Breslow thickness are sufficient and that they are important prognostic factors (8, 29). Patient phenotype and genotype might also influence survival, although such data are not available through registry-based studies. Data on metastatic melanomas with an unknown primary tumour were also missing. Furthermore, immigrants into Sweden who died from melanoma but were diagnosed elsewhere, were not included in the analyses. The study time-frame prevented us from performing a 20-year survival analysis, without a substantial part of patients being censored at the end of the study period (31 December 2014). However, 89.0% of patients (diagnosis year 1990 to 2004) who died in the study period, died within 10 years. Thus, a 10-year survival analysis was appropriate.
Some previous studies have excluded multiple primary melanomas (7, 15) in order to make sure that a subsequent melanoma was not the cause of death, and some other studies have chosen not to (9). We chose to exclude multiple primary melanomas from our primary analysis, but also performed alternate analyses. Since we did not find any essential change in the size of the effect in the alternate analyses, we do not believe this had any impact on our findings.
In conclusion, patients with thin melanomas comprise a non-negligible proportion of the patients who ultimately die from the disease, in spite of the good prognosis for thin tumours in general. Non-ulcerated melanomas with a Breslow thickness of 0.76–1 mm and ulcerated melanomas 0.26–1.0 mm have a poorer survival compared with other thin melanomas. More attention should be brought to such melanoma patients with regards to their management and follow-up.
The authors would like to thank statistician, PhD Erik Holmberg, at the Regional Cancer Centre Western Sweden, and statistician Rasmus Mikiver at the Regional Cancer Centre Southeast for the extraction of data from the regional part of the Swedish Melanoma Registry, and for linking the data to the national Cause of Death Registry.
The federal government supported this study financially under the ALF agreement. Also, the Hudfonden Foundation provided financial support.
DCW is supported by a Research Fellowship (APP1058522) from the National Health and Medical Research Council of Australia.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize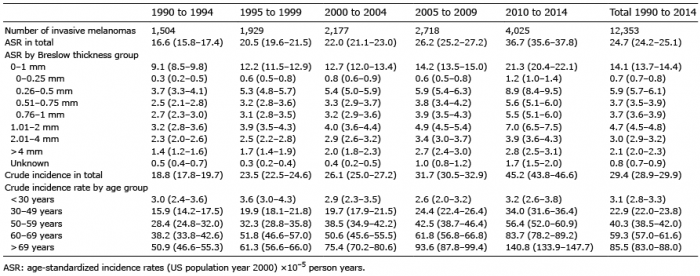 Click to show fullsize
Click to show fullsize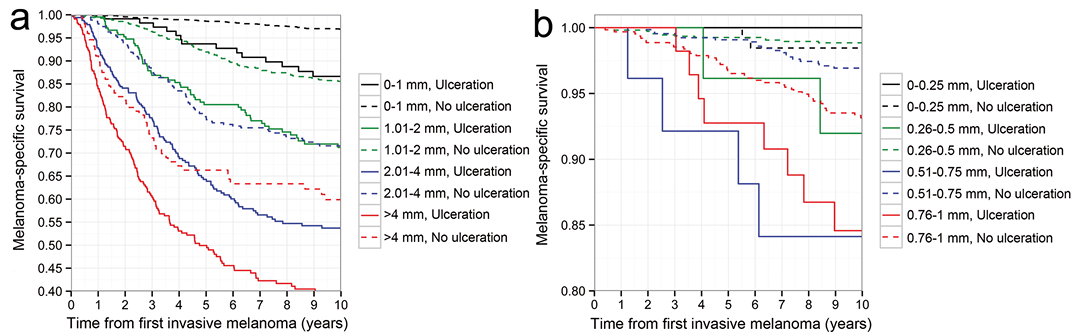 Click to show fullsize
Click to show fullsize