


1Department of Dermatology, Medical University of Vienna, Vienna, Austria, 2Dermatology Unit, Second University of Naples, Naples, Italy, 3Service de Dermatologie, Centre Hospitalier Universitaire de Lyon, Lyon, France, 4Non Melanoma Skin Cancer Unit, Department of Dermatology and Venereology, Medical University of Graz, Graz, Austria, 5Department of Dermatology, University of Florence, Florence, Italy, 6First Department of Dermatology, Aristotle University, Thessaloniki, Greece, 7Melanoma Unit, Departments of Dermatology, Hospital Clínic de Barcelona, IDIBAPS, Barcelona University, Centre of Biomedical Research on Rare Diseases (CIBERER), ISCIII, Barcelona, Spain, 8Dermatology and Skin Cancer Unit, Arcispedale Santa Maria Nuova IRCCS, Reggio Emilia, 9Department of Dermatology, University of Naples Federico II, and 10Department of Anesthesiology, Surgery and Emergency, Second University of Naples, Naples, Italy
Facial melanoma is difficult to diagnose and dermatoscopic features are often subtle. Dermatoscopic non-melanoma patterns may have a comparable diagnostic value. In this pilot study, facial lesions were collected retrospectively, resulting in a case set of 339 melanomas and 308 non-melanomas. Lesions were evaluated for the prevalence (> 50% of lesional surface) of 7 dermatoscopic non-melanoma features: scales, white follicles, erythema/reticular vessels, reticular and/or curved lines/fingerprints, structureless brown colour, sharp demarcation, and classic criteria of seborrhoeic keratosis. Melanomas had a lower number of non-melanoma patterns (p < 0.001). Scoring a lesion suspicious when no prevalent non-melanoma pattern is found resulted in a sensitivity of 88.5% and a specificity of 66.9% for the diagnosis of melanoma. Specificity was higher for solar lentigo (78.8%) and seborrhoeic keratosis (74.3%) and lower for actinic keratosis (61.4%) and lichenoid keratosis (25.6%). Evaluation of prevalent non-melanoma patterns can provide slightly lower sensitivity and higher specificity in detecting facial melanoma compared with already known malignant features.
Key words: dermatoscopy; dermoscopy; face; melanoma; lentigo maligna; diagnosis.
Accepted Jul 31, 2017; Epub ahead of print Aug 1, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Giuseppe Argenziano, Dermatology Unit, Second University of Naples, Via Pansini 5, IT-80131 Naples, Italy. E-mail: g.argenziano@gmail.com
Facial flat pigmented lesions are a diagnostic challenge clinically and dermatoscopically, because many benign lesions show some degree of malignant features, and early melanoma may exhibit only subtle malignant criteria. The dermatoscopic presentation of facial melanoma (FM) was first described by Schiffner et al. (1) and Stolz et al. (2), followed by several studies (3–10) reporting additional morphological clues. However, the differentiation of FM from pigmented actinic keratosis (pAK) remains one of the greatest challenges (4, 10). For example, classic features of FM, such as rhomboidal structures, can be seen in both pAK and FM (9). Additional benign lesions, especially solar lentigines (SL) with regressive features (lichenoid keratosis; lichen planus-like keratosis (LPLK); seborrhoeic keratosis or solar lentigo in regression), may show features that overlap with FM. An important clue to malignancy is the presence of grey structures that, although having a good sensitivity (85.1%), reach a specificity of only 39.7% (9). In addition, recognizing grey colour dermatoscopically is a challenge for inexperienced physicians (personal observation, PT and GA), thus a method based on easily recognizable features is urgently needed to improve the early recognition of FM (11).
The aim of this study was to test an algorithm composed of negative criteria for differentiating early melanoma from flat benign lesions of the head/neck region. For this method, a lesion is scored “benign” when any prevalent non-melanoma feature is found, and “suspicious” when none or only non-prevalent non-melanoma features are found.
Dermatoscopic images, acquired using polarized and non-polarized light, from flat lesions located on the head/neck region were selected from the databases of 7 clinics for pigmented lesions in Italy, Austria, France and Spain. Retrospectively, histopathologically diagnosed early melanomas (in situ or less than 0.7 mm thick), SL, early seborrhoeic keratosis (SK), pAK, and LPLK were retrieved from the image databases of the collaborating centres. To include a representative number of SL that were not excised, a random sample of flat pigmented lesions that were followed longitudinally and examined by confocal microscopy (between 2014 and 2015) were included. If the lesion was diagnosed as benign by confocal microscopy, it was not excised. If the lesion was doubtful under confocal microscopy, a histopathological diagnosis was obtained before inclusion. A benign lesion might also be included if it was monitored for at least one year without change. For this pilot study, no sample size calculation was performed.
Age, sex, diagnosis (either histopathological diagnosis, confocal diagnosis or diagnosis after 1-year follow-up) and eventual Breslow thickness were collected in a Microsoft Excel® file. For each lesion, 1 dermatoscopic image was evaluated separately in a blinded fashion by 2 observers (AG, RA). A third observer (GA) was consulted when there was disagreement between the 2 main observers. The following 7 non-melanoma features were scored as absent, present (but not prevalent), and prevalent (feature found in more than 50% of the lesion surface): 1) scales (pigmented or non-pigmented); 2) white follicles (including white circles, follicular white clods and 4-dot-clods (rosettes)); 3) erythema or reticular vessels; 4) reticular (network) and/or curved/parallel lines (fingerprints); 5) structureless brown colour; 6) sharp demarcation; and 7) classic SK criteria (white dots/clods (milia-like cysts), brown-orange clods (comedo-like openings), thick curved lines (fat fingers)) (Figs 1, 2). Furthermore, all lesions were evaluated for the presence or prevalence of any of the previously described malignant features: 1) grey colour; 2) pattern of circles (brown and grey); 3) scattered globules; 4) annular granular pattern; 5) rhomboidal structures; 6) obliterated hair follicles; and 7) blue and/or white areas. Selection of these features was based on literature review and personal experience of the authors. Descriptive terms were used according to the international consensus of terminology in dermatoscopy (12).
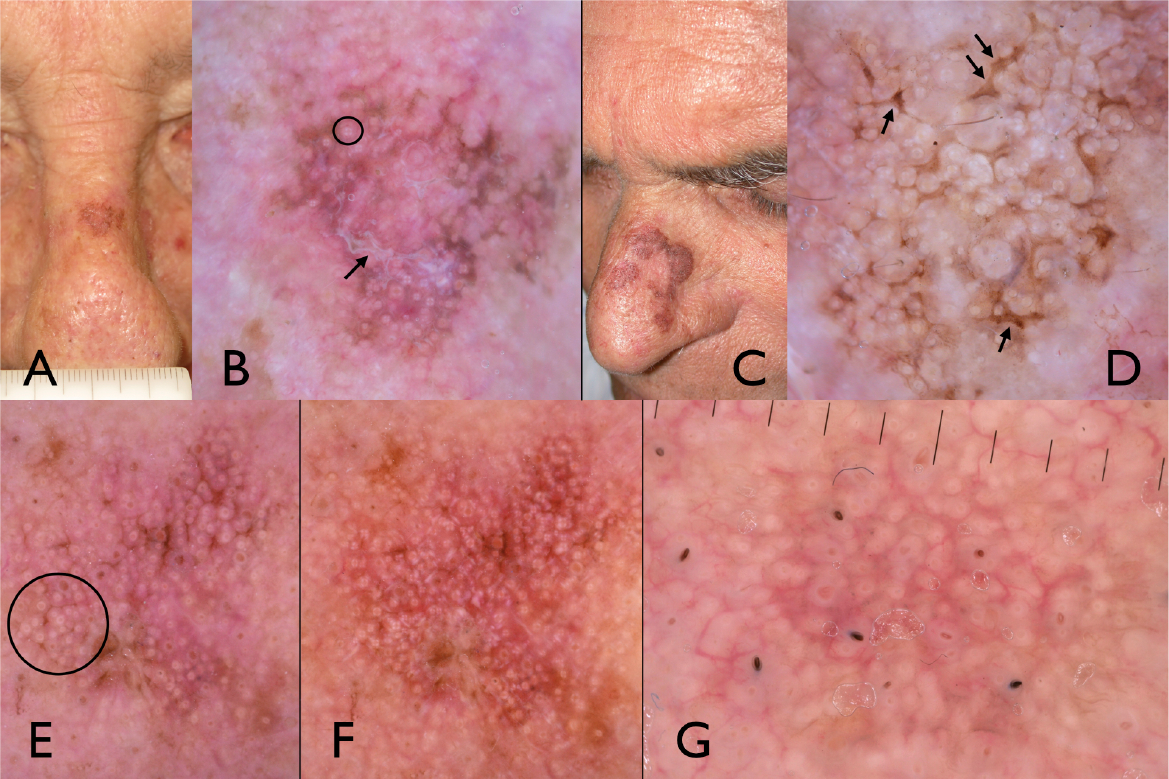
Fig. 1. Examples of actinic keratosis (AK). (A) Clinical and (B) polarized dermatoscopic views of a pigmented AK showing non-pigmented scales (arrow) and multiple rosettes (circle). (C) Clinical and (D) polarized dermatoscopic views of a pigmented AK with multiple pigmented scales (arrows) and rosettes. (E) A pigmented AK showing multiple white follicles (circle) under non-polarized dermatoscopy. (F) The same lesion imaged with polarized dermatoscopy shows multiple rosettes instead of the white follicles. (G) An AK showing dermatoscopically predominant reticular vessels and only subtle grey colour.
Fig. 2. Examples of solar lentigo (SL). (A) Clinical and (B) polarized dermatoscopic views of a SL showing predominant reticular/parallel lines (fingerprint-like structures; arrow). (C) Two SL showing predominant reticular lines and brown structureless areas (D) sharply demarcated at the periphery. (E) Clinical and (F) polarized dermatoscopic views of a SL/early seborrhoeic keratosis typified by parallel lines (fingerprints) and a cluster of white dots (milia-like cysts; circle). (G) Clinical and (H) polarized dermatoscopic views of a melanoma in situ showing a combination of melanoma (grey colour, polygons) and non-melanoma (reticular lines) features. However, reticular lines are only focally visible, whereas most of the lesion is typified by grey structures and an ill-defined border.
Statistical analysis and production of graphs was performed with R (13), using packages epiR (14) and ggplot2 (15). Tests were performed according to data distribution, and a 2-tailed p-value of < 0.05 was considered statistically significant. The multivariate logistic regression model included all non-melanoma features, controlled for age and sex of the patient.
Mean age of patients was 66.7 years (95% confidence interval (95% CI) 65.6–67.7) and 46.7% (n = 302) were female. The collection consisted of 339 melanomas (MM) and 308 non-melanomas (151 SL, 83 actinic keratoses (AKs), 39 LPLK and 35 SK). Patients with a melanoma were older (mean 69.2 vs. 63.9 years; p < 0.001) and, statistically non-significant, less commonly female compared with those with a non-melanoma lesion (43.1% vs. 50.6% female; p = 0.06).
Melanomas had a significantly lower number of non-melanoma features (median 0 vs. 2, Kruskal–Wallis p < 0.001, Fig. 3).
Fig. 3. Proportion of melanoma vs. non-melanomas in lesions with different numbers of benign patterns. The chance of diagnosing a melanoma is low in a lesion with multiple non-melanoma patterns; whereas a single focal non-melanoma pattern is a common finding in facial melanoma (1 point is counted for every non-melanoma feature present, where a prevalent pattern counts for 2).
All of the non-melanoma features were more common in non-melanomas than in melanoma (Fig. 4 A–D), except for focal (not prevalent) reticular lines (Table I). No melanomas showed prevalent scales or classic SK features; thus these criteria virtually excluded the diagnosis of melanoma when found to be prevalent within a given lesion. In a multivariate logistic regression model, all non-melanoma features remained significant independent predictors for a diagnosis of non-melanoma.
Fig. 4. Examples of distinguishing features between melanoma and solar lentigo (SL). (A) Clinical and (B) polarized dermatoscopic views of a SL vs. (C) clinical and (D) polarized dermatoscopic views of a melanoma in situ. The differentiation is made possible by (B) predominant reticular lines and (D) absence of non-melanoma features (e.g. a sharply demarcated border) with only subtle grey circles. (E) Dermatoscopy of a melanoma showing a prevalent non-melanoma pattern (reticular lines) but recognized by the presence of grey colour (circle). (F) Dermatoscopy of a melanoma correctly diagnosed only because of the absence of non-melanoma features (e.g. a sharply demarcated border).
Table I. Frequencies and significance of rated features
A method scoring a lesion suspicious when no prevalent non-melanoma patterns are found resulted in a sensitivity of 88.5% (95% CI 84.6–91.7) and a specificity of 66.9% (95% CI 61.3–72.1). Negative and positive predictive values were 84.1% and 74.6%, respectively.
Specificity (number of correctly diagnosed non-melanomas by the presence of a prevalent non-melanoma pattern) differed highly between specific diagnoses (Table II). The lowest specificity was found for LPLK and the highest for SL and SK. In all, 75.9% (n = 491) of lesions were biopsied (all FM and 49.4% of non-melanomas), and specificity of the scoring differed between the 2 groups of biopsied (59.9%) and not-biopsied (73.7%) lesions.
Table II. Specificity for different benign diagnoses, which is highest for seborrhoeic keratoses (SK) and solar lentigines (SL), followed by actinic keratoses (AK). Lowest specificity was found for lichen planus-like keratoses (LPLK)
In all, 318 of 339 melanomas and 161 of 308 benign lesions showed malignant features (i.e. prevalent or non-prevalent malignant features), resulting in a sensitivity of 93.8% (95% CI 90.7–96.1) and specificity of 52.3% (95% CI 46.5–58.0).
The present study showed that the evaluation of dermatoscopic non-melanoma patterns of facial lesions can result in similar sensitivity (88.5%) but higher specificity (66.9%) for melanoma than using malignant features (9, 10). However, one of the most common and challenging differential diagnosis is between FM and AK (4, 16). In a study comparing only these 2 diag-noses, use of a semiquantitative algorithm allowed a sensitivity of 92.9% and specificity of 55.4% to be reached (10). In the present study, including all main diagnostic categories of facial lesions, our approach allowed better specificity, resulting in a higher diagnostic performance (Youden’s J 0.55 vs. 0.48). This might lead to the conclusion that semiquantitative algorithms are not superior to simple decision trees (17) in the context of facial lesions.
Another simple approach for diagnosing malignant lesions on the face was based on the evaluation of grey colour (18) as the only clue for malignancy (9). Although very easy to apply in practice, and promising in terms of sensitivity for melanoma (85.1%), its specificity was rather low (39.7%). By evaluating the presence of non-melanoma patterns, the present approach might likewise be easy to apply in practice, similarly sensitive, but better in terms of specificity.
The specificity of the approach presented here is the highest among the published clinically applicable dermatoscopic algorithms for facial lesions, but remains below 70% (higher specificities have been reported previously in more detailed multivariate regression models (10)). Looking at subgroups, the lowest specificity was found for AK (a lesion for which biopsy may be considered reasonable) and LPLK. Because of the presence of regressive features (20), LPLK commonly show grey structures in dermatoscopy and rarely exhibit prevalent non-melanoma features. Thus, in most cases preoperative differentiation between LPLK and FM is virtually impossible and a biopsy is usually needed. Since LPLKs are relatively uncommon in clinical routine, in our opinion performing a biopsy of these difficult-to-diagnose lesions does not represent a significant clinical problem. On the other hand, pigmented AK and SL are much more common, and regardless of the dermatoscopic algorithm used, specificity is rather low. Options to reduce the number of unnecessary excisions of benign lesions are digital monitoring (21) or confocal microscopy (22–25), which are highly efficient in the context of facial lesions. Of course careful clinical evaluation, such as tactile information, has always to be coupled with the dermatoscopic examination, as AK (26) and lentigo maligna (27) have distinct clinical presentations that usually contribute to diagnostic reasoning.
The idea of evaluating non-melanoma patterns to rule out melanoma is not completely new in dermatoscopy. Schiffner et al. proposed “fingerprint-like areas” and “horny pseudocysts” as features representing benign growth (1). Also, Marghoob & Braun (28) described benign patterns of the most common skin lesions and used these criteria as a triage system within the 2-step method of dermatoscopy. Pattern recognition is based on the so-called heuristic approach of morphology (an examiner comparing a lesion with known patterns), which is a simple method providing similar diagnostic accuracy compared with more complex reasoning (29, 30).
Regarding the value of specific sub-patterns, 2 of these require further discussion. First, brown structureless areas strongly favour a non-melanoma, although, at least theoretically, this pattern could be better correlated to the most common histopathological feature of lentigo maligna, namely a single-cell proliferation of melanocytes within the epidermis (31). A possible explanation is that, in lentigo maligna, atypical melanocytes are also found within the follicular epithelium; as these melanocytes go down vertically within the follicle they become more evident compared with the single cells along the basal layer, giving rise to a pattern of circles (23), as typically seen in lentigo maligna. Secondly, reticular lines were very frequently found in benign facial lesions, but also rather often in FM (Fig. 4E). This could be explained by the fact that many FM develop in collision with SL, especially in patients with severely sun-damaged skin. However, in most of our FM reticular lines were only focally present within the given lesion, which instead frequently showed prevalent malignant features.
The main limitation of our study is the mixed retrospective design; the results should be validated using a prospective approach. Lesions were verified histopathologically, diagnosed by follow-up imaging or reflectance confocal microscopy. This suggests a selection bias towards lesions that are difficult to diagnose clinically or dermatoscopically, therefore possibly underestimating specificity in clinical practice. In addition, recurrent FM, a group not included in this study, might show other specific diagnostic criteria. Finally, being a pilot study, the results need to be validated in follow-up studies.
Instead of focusing on malignant features alone, as is the case for other dermatoscopic algorithms, facial melanomas could also be differentiated through evaluation of non-melanoma features, and a lesion biopsied if no prevalent non-melanoma patterns are clearly seen within the lesion.
Funding sources: JM and SP: The research at the Melanoma Unit in Barcelona is partially funded by Spanish Fondo de Investigaciones Sanitarias, grants PI12/00840, PI15/00716 and PI15/00956; CIBER de Enfermedades Raras of the Instituto de Salud Carlos III, Spain, co-financed by European Development Regional Fund “A way to achieve Europe” ERDF; AGAUR 2014_SGR_603 of the Catalan Government, Spain; European Commission under the 6th Framework Programme, Contract No. LSHC-CT-2006-018702 (GenoMEL) and by the European Commission under the 7th Framework Programme, Diagnoptics; a grant from “Fundació La Marató de TV3, 201331-30”, Catalonia, Spain; a grant from Telemaraton of Spain “Todos somos raros” and a grant from “Asociación Española Contra el Cáncer (AECC)”. The work was carried out at the Esther Koplowitz Center, Barcelona.


 Click to show fullsize
Click to show fullsize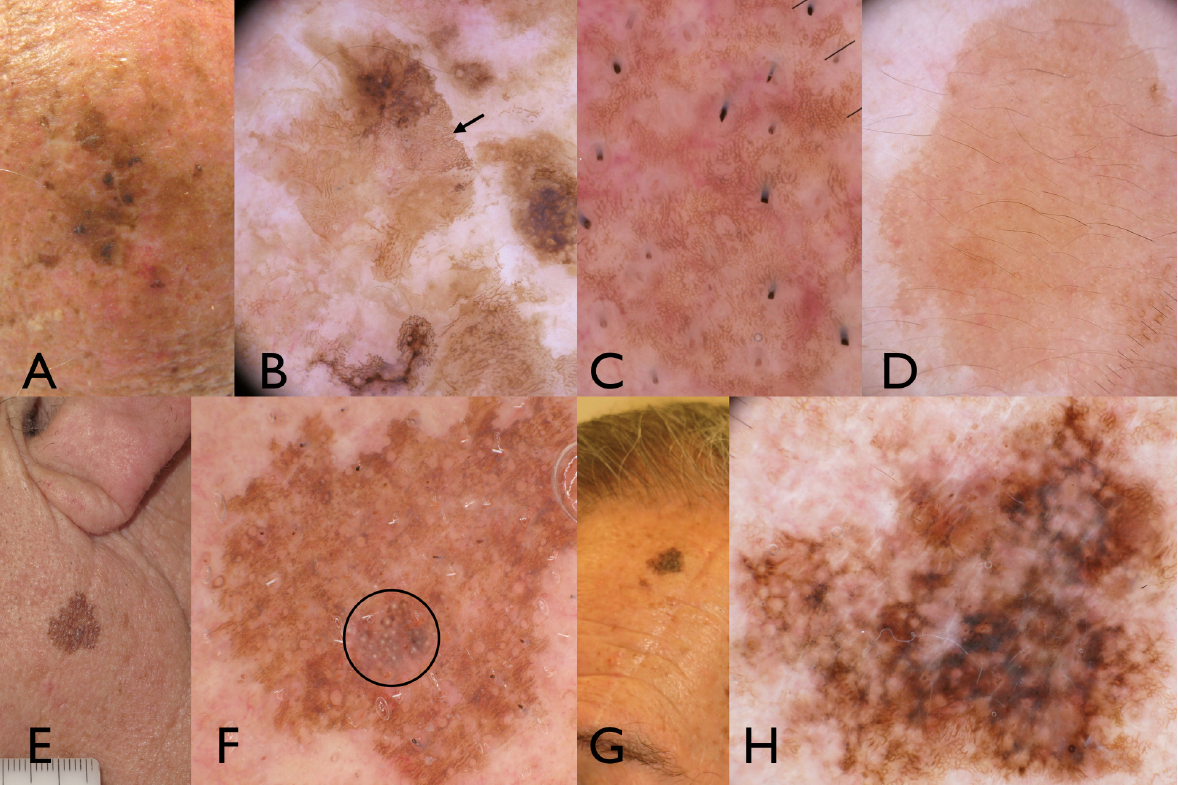 Click to show fullsize
Click to show fullsize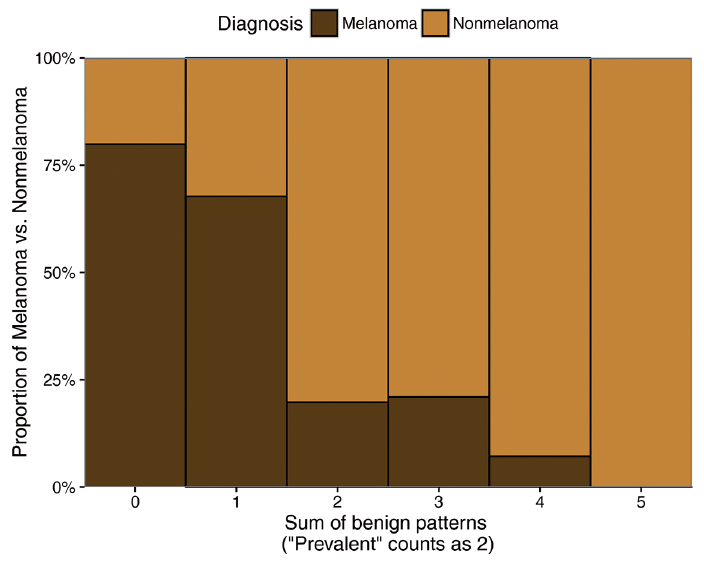 Click to show fullsize
Click to show fullsize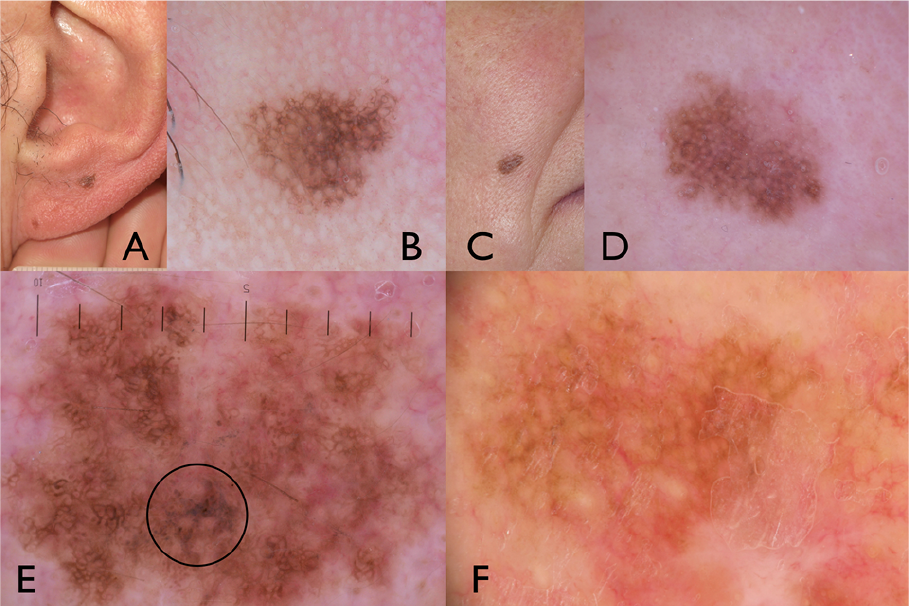 Click to show fullsize
Click to show fullsize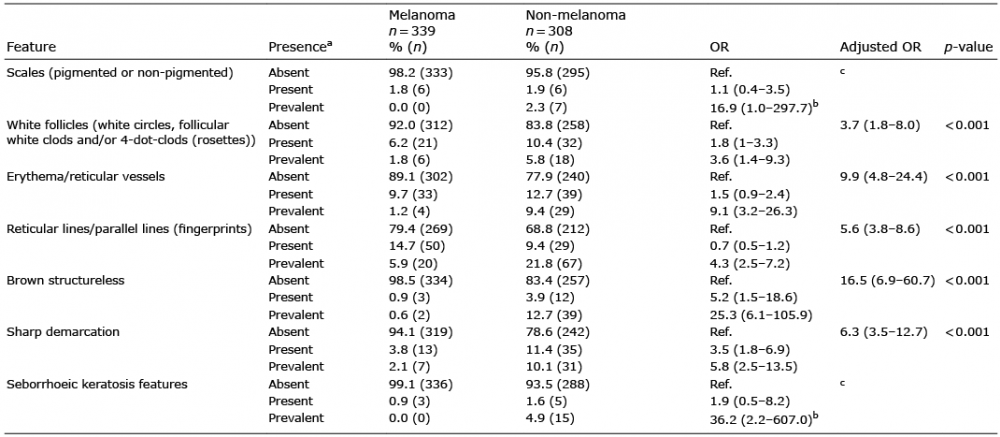 Click to show fullsize
Click to show fullsize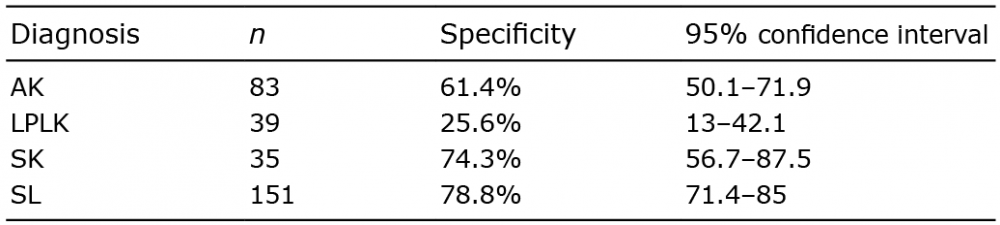 Click to show fullsize
Click to show fullsize