


Departments of 1Infectious and Tropical Diseases, 2Gynaecology and 3Virology, Hôpital Pitié-Salpétrière, 45-83 Bd de l’hôpital, FR-75013 Paris, and 4Department of Dermatology, Hôpital Cochin, Paris, France. E-mail: agathe.nouchi@gmail.com
Accepted Aug 9, 2017; Epub ahead of print Aug 10, 2017
Acute genital ulcer (AGU), also known as reactive non-sexually-related acute genital ulcers, ulcus vulvae acutum or Lipschütz’s ulcer, was first described in 1913. This non-venereal acute genital ulceration, of unknown aetiology, is associated with infections caused by various microorganisms, in particular acute Epstein-Barr virus (EBV) infection (1–4). The ulceration usually heals spontaneously within 2–4 weeks, but treatment may be necessary in severe cases.
We report here a case of AGU due to reactivation of EBV, which was treated successfully with colchicine, whereas other treatments failed.
A previously healthy, Caucasian, non-virgin, 18-year-old female presented with a 2-week history of fever, malaise, nausea and sore throat, and a 10-day history of intense vulvar pain, followed by acute vulvar ulcerations. Treatment with valacyclovir, started by her general practitioner, had no effect on the vulvar lesions.
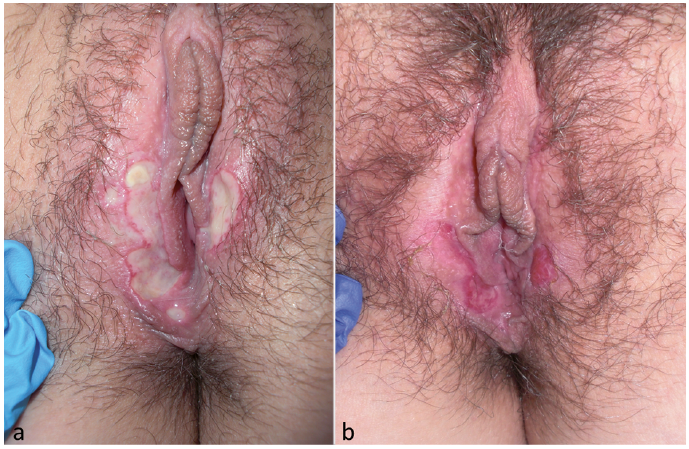
She was then referred to our department and hospitalized for pain management. Any traumatic precipitating factor was denied. She did not report any personal or familial history of oral or genital aphthous or digestive disorders. On physical examination, she had enlarged and erythematous tonsils. Her oral mucosa was normal. Wide, isolated or confluent, well-circumscribed ulcers were present on the fourchette and on the inner posterior aspects of the labia majora, in a bilateral kissing pattern (Fig 1a). The periphery of the ulcers was red, whereas their surface was yellow due to fibrin deposit. There was no further fever and no other systemic signs of infection.
Fig. 1. Clinical findings. (a) Wide, well-circumscribed ulcers of the fourchette and inner posterior aspects of the labia majora. (b) Almost complete ulcer healing on the 7th day of treatment.
Laboratory findings showed a mononucleosis syndrome with 10,850/mm3 white blood cells including 5,420/mm3 lymphocytes (50%) and 1,080/mm3 monocytes (10%) and presence of hyperbasophilic atypical lymphocytes. Serological tests for Treponema pallidum, human immunodeficiency virus, cytomegalovirus (CMV), herpes simplex virus (HSV) and toxoplasmosis were negative. Bacteriological analysis of genital swabs was negative, as well as PCR on genital lesions for HSV 1 and 2, varicella-zoster virus, CMV and EBV. EBV serology was positive for IgM against viral capside antigen (VCA) and IgG against VCA and the nuclear antigen (EBNA), in favour of viral reactivation. PCR for EBV on blood was weakly positive at 2.9log (801 copies/ml). We decided not to perform a vulvar biopsy due to the limited diagnostic value and the invasiveness of this procedure.
Opioids and topical lidocaine could not reduce the patient’s intense pain, causing dysuria and requiring a urinary catheter. Topical and systemic corticosteroids (0.5 mg/kg/day for 3 days) brought no improvement. Topical imiquimod for 3 days was also not effective and, 20 days after onset, new ulcerations occurred on the inner aspect of both labia minora. Treatment with colchine, 1 mg per day, was therefore introduced, leading to a rapid reduction in pain intensity and almost complete ulcer healing on the 7th day of treatment (Fig. 1b). Treatment was stopped after 10 days, with no relapse during the 24-months follow-up. A control of EBV serology performed one month later revealed the disappearance of IgM anti-VCA with persistence of IgG anti-VCA and anti-EBNA, whereas the EBV PCR on blood was negative, all of which confirmed reactivation of EBV.
Although the aetiologies and pathogenic mechanism of AGU are not fully understood, and some authors still do not distinguish AGU from vulvar aphthosis (5, 6), the term AGU should be used to refer only to non-venereal genital ulceration that appears to occur suddenly in response to a systemic infection, with exclusion of idiopathic and complex aphthosis and chronic systemic diseases, such as Behçet’s and Crohn’s diseases (1).
The association of some cases of AGU with EBV infection was suggested in 1977 and, since then, approximately 40 EBV-linked cases have been reported, mostly during primary infection or unspecified EBV infection (4), the involvement of EBV being reported in approximately 30% of AGU (1). Other infectious agents have also been involved in some cases, including CMV (7), Toxoplasma gondii, Mycoplasma pneumonia (6), Streptococcus spp, Salmonella enterica (8), mumps, influenza A and B virus, adenovirus (9), and Borrelia burgdorferi (10).
AGU typically presents with acute, very painful, well-circumscribed fibrinous or necrotic vulvar ulcers in a “kissing pattern” (1–4), usually preceded by flu-like systemic signs, such as fever, headache, fatigue or tonsillitis, occurring in immunocompetent young girls. However, the mean age of 15.1 years reported in the literature (1) may be artificially low, since, by definition, physicians have been excluding older women from this possible diagnosis. In addition, in contrast to the original description, as in the current case, most girls currently affected are not virgins.
Biology often shows a discrete hepatic cytolysis. Histology of the genital lesion can show a localized lymphocytic arteritis with a dense, perivascular, mixed or T-lymphocytic inflammatory cell infiltrates (11). Biopsy might be needed to rule out malignancy for long-lasting ulcers, especially in adult women, but it lacks relevance in younger women and in ulcers with shorter duration. The mean duration of lesions is approximately 20 days, but it may increase to 10 weeks. There is typically no associated oral aphthosis and no further relapse of genital ulcers, differentiating it from idiopathic genital aphthosis (1–4).
In cases of EBV-associated AGU, biology usually shows a mononucleosis syndrome and signs of primary infection with IgM against VCA and seroconversion of EBNA antibodies. EBV PCR is usually positive in the blood and sometimes on vulvar swabs, and in situ hybridization and immunohistochemistry was positive in one case (1). Apart from our patient, we found only one reported case of an AGU associated with a well-documented EBV reactivation (11).
To date, it is not known whether EBV-associated AGU is caused by interplay between a direct cytolytic effect of EBV replication on the vulvar epithelium and the associated cytolytic immune response, or whether it is due to a localized destructive type-III hypersensitivity reaction to deposited immune complex produced during the acute phase of EBV infection (4). For most authors, it is a reactive dermatosis, resulting from an exuberant systemic immune response to an acute infection (1, 4). Our case confirms that viral reactivation can also lead to lesions, without evidence of EBV in situ.
Treatment of AGU may be necessary in some patients, due to intense pain and long-lasting lesions, with the risk of disfiguring scars (12). Treatment with anti-CD20 antibodies did not seem relevant in the current case, as EBV viraemia was weak and the patient was not immunosuppressed. Acyclovir is very poorly effective in EBV infections (13). Topical and systemic corticoids did not lead to any improvement, although they have sometimes been reported to be partially effective (1, 2, 4). Due to its immunomodulatory action and its known efficiency in herpes infections (14), topical imiquimod was applied for 3 days, without success. Colchicine was then introduced because of the emergence of new ulceration 20 days after onset. This treatment is indicated in inflammatory diseases, such as Behçet’s disease, recurrent aphthosis, leukocytoclastic vasculitis and neutrophilic dermatoses. Its efficiency is presumably based on its anti-inflammatory effect, resulting from the inhibition of chemotaxis and phagocytic activity of neutrophils (15). Our patient’s rapid improvement under colchicine suggests that this treatment has at least accelerated healing, possibly acting through the same mechanisms as in aphthosis. We cannot exclude that spontaneous healing occurred at the time the treatment was introduced, although the occurrence of new lesions on the previous day argues against this hypothesis.
Finally, what we have labelled AGU might be the first episode of a recurrent aphthosis, but our patient showed no relapse within the 24 months of follow-up and there was no history of familial aphthosis.
Thus, this case of AGU confirms that this disease can be associated with EBV reactivation and not only with primary infections, and suggests that colchicine could be a treatment of interest in cases where spontaneous recovery does not occur.


 Click to show fullsize
Click to show fullsize