


1Department of Dermatology and Allergy, Technical University of Munich, Munich, Germany, 2Kempf & Pfaltz, Histologische Diagnostik, Zürich, and 3Department of Dermatology, University Hospital Zurich, University of Zürich, Gloriastrasse 31, CH-8091 Zurich, Switzerland. E-mail: emmanuella.guenova@usz.ch
A 60-year-old woman presented with a distinct, sharply demarcated plaque on her left flank. The plaque measured approximately 8 cm in diameter and consisted of confluent, brownish-erythematous dome-shaped papules, with a partially verrucous surface (Fig. 1A). In addition, she reported a subcutaneous nodule on the left upper arm. The lesions first appeared 4 months earlier with mild itching and pain. Physical examination revealed no further involvement of the skin or palpable lymph nodes. Beside arterial hypertension and a dyslipidaemia, her medical history, familial medical history and routine laboratory tests were unremarkable. A punch biopsy specimen from the lesion on the flank and an excision biopsy of the nodule on the upper arm were obtained.
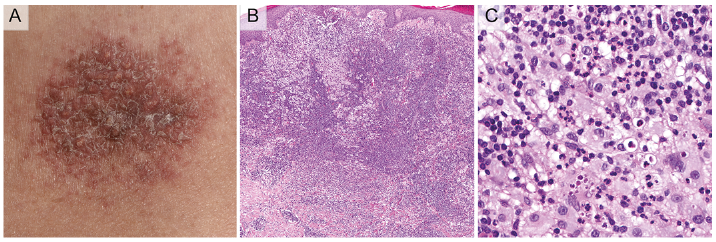
Fig. 1. (A) Sharply demarcated plaque on the left flank, consisting of confluent, brownish-erythematous dome-shaped papules, with a partially verrucous surface. (B) Haematoxylin and eosin (H&E) staining with dense dermal infiltrate of histiocytes admixed with inflammatory cells: plasma cells, lymphocytes and eosinophils (original magnification ×2). (C) Aggregates of large histiocytes with slightly eosinophilic cytoplasm containing inflammatory cells within their cytoplasm: emperipolesis (original magnification ×40).
What is your diagnosis? See next page for answer.
Acta Derm Venereol 2017; 97: xx–xx.
Diagnosis: Cutaneous Rosai-Dorfman Disease (sinus histiocytosis with massive lymphadenopathy)
Biopsy specimens revealed a dense dermal infiltrate consisting of histiocytes admixed with inflammatory cells: plasma cells, lymphocytes and eosinophils (Fig. 1B). Emperipolesis, which is a process of engulfment of viable inflammatory cells by histiocytes, could be detected (Fig. 1C). Immunohistochemistry showed co-expression of S100 and CD68 in the histiocytic cells, whereas CD1a remained negative. The 18F-fluoro-2-deoxy-D-glucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) did not detect lymph node involvement or extranodal manifestation of Rosai-Dorman disease (RDD).
RDD, also known as sinus histiocytosis with massive lymphadenopathy, is a rare, self-limiting histiocytic disorder of unknown aetiology (1). The polyclonality of the cellular infiltrate in RDD suggests that the disease has a reactive rather than a neoplastic nature. Abnormal response to antigenic stimuli may be related to RDD; circulating antibodies to Borrelia, human herpes virus 6, and Epstein-Barr virus have been detected in some patients (2). RDD is typically characterized by lymphadenopathy (especially bilateral cervical lymphadenopathy), fever and weight loss, leukocytosis, polyclonal gammopathy, anaemia, and elevated erythrocyte sedimentation rate. Extranodal lesions occur in approximately one-third, and the skin has been involved in > 10% of reported cases. RDD limited to the skin only is rare, with < 100 cases reported until now (3).
The histological features of RDD in the lymph nodes are characteristic, and include expansion of the sinuses by large foamy histiocytes admixed with plasma cells. Cutaneous lesions show a dense dermal infiltrate of polygonal histiocytes with abundant pale cytoplasm, large nuclei with dispersed chromatin and prominent nucleoli. The skin infiltrate is admixed with inflammatory cells: plasma cells, lymphocytes and eosinophils (1). The enlarged histiocytes stain positive for CD68 and S100 and are negative for CD1a (2). Emperipolesis, which is a process of engulfment of inflammatory cells, protected from degradation by intracytoplasmatic vacuoles within the cytoplasm of the histiocytes, is a hallmark feature of RDD. Emperipolesis can be also observed in other haematological and non-haematological conditions, such as leukaemia, and multiple myeloma (4).
Treatment approaches for RDD depend on the nodal or extranodal manifestation of the disease and the clinical symptoms. As spontaneous resolution has been reported, “wait and see” is an option for patients with uncomplicated lymph node involvement or asymptomatic cutaneous RDD. Surgical excision, radiotherapy and systemic corticosteroids have been used with some success. In the case presented here, radiotherapy to a total cumulative dose of 32 Gray did not result in a clinical response. As a second-line line approach it was decided to use class IV topical steroids, and this treatment is currently ongoing. If topical steroids are also ineffective, either surgical excision or “watchful waiting” will be proposed to the patient. There are scattered reports on the use of thalidomide, imatinib, rituximab, oral 6-mercaptopurine and methotrexate for patients with refractory RDD (5–7). Clofarabine and cladribine have been applied in patients with relapsed, multisystem, non-resectable central nervous system (CNS) or autoimmune-related RDD (8).


 Click to show fullsize
Click to show fullsize