


1Department of Dermatology, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya 466-8550, and 2Department of Nursing, Sugiyama Jogakuen University School of Nursing, Nagoya, Japan. *E-mail: miro@med.nagoya-u.ac.jp
Accepted Aug 16, 2017; Epub ahead of print Aug 17, 2017
Staphylococcal scalded skin syndrome (SSSS) is a systemic toxic disease whose symptoms include diffuse erythema and blister formation over the whole body (1). SSSS develops when exfoliative toxin (ET) produced by Staphylococcus aureus reaches the skin via blood flow. SSSS is ordinarily seen in children; in adults it is rare but serious (1). We report here a severe case of adult SSSS caused by an ET A-producing strain of Staphylococcus. The patient had had immunosuppressive therapy for rheumatoid arthritis (RA) and was complicated with kidney failure associated with septic shock. She was treated successfully with intravenous immunoglobulin (IVIG) therapy.
The patient was a 71-year-old woman with a history of RA. She had been taking methotrexate, 8 mg per week, as well as non-steroidal anti-inflammatory drugs. She had regularly received intra-articular injections of hyaluronic acid to treat osteoarthritis of the right knee joint. Four days before her first visit to our hospital, she developed general malaise and rashes on the limbs and trunk. As those symptoms did not resolve, she visited a neighbourhood clinic. The general physician suspected drug eruption and prescribed oral prednisolone, 15 mg/day. However, the rash spread and the malaise intensified. The patient was referred to our hospital and arrived by ambulance. On arrival, she was in septic shock and had generalized rash with erosions and bullae. The emergency physician suspected toxic epidermal necrolysis (TEN) and consulted us.
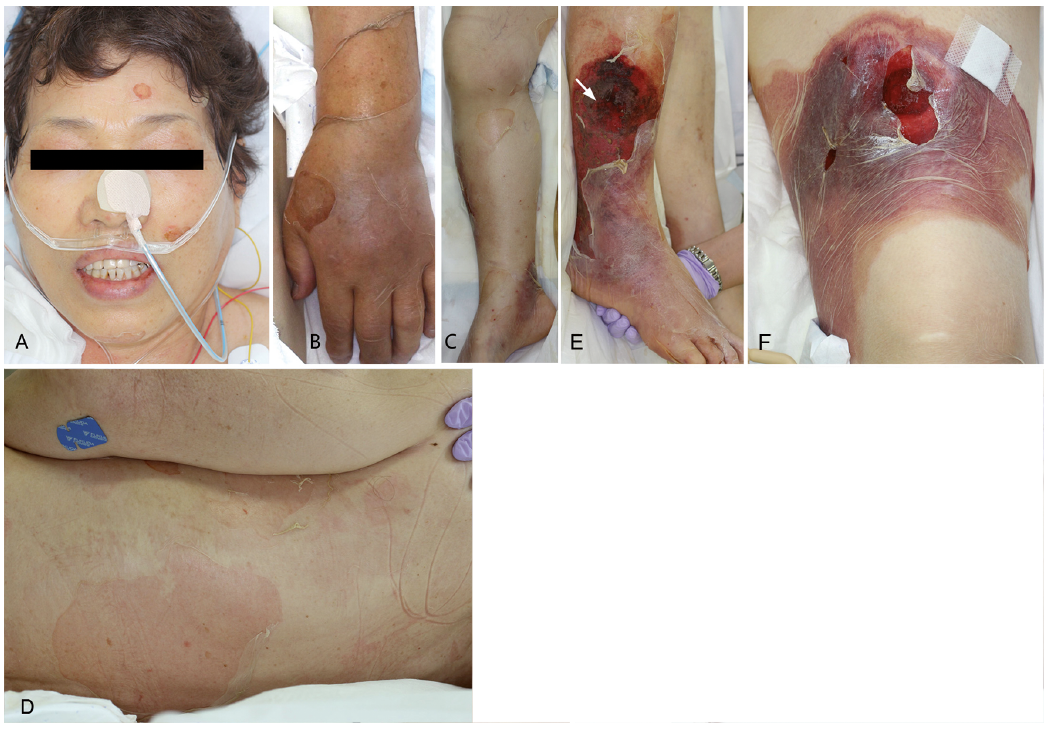
At initial examination, membranous blister roofs, shallow erosions and flaccid bullae were observed over most of the patient’s body, but predominantly on intertriginous areas of the limbs and the trunk (Fig. 1A–D). Purpura was observed on the right calf and the left thigh (Fig. 1E, F). Enanthema was not observed in the oral cavity, the eyes, or the vulva. Mild, but painful, swelling was noted in the right knee joint.
Fig. 1. Clinical features of the adult patient with staphylococcal scalded skin syndrome (SSSS). (A) Erosive plaques and shallow flaccid bullae are observed on the face. The erosive plaques with crusts around the eyes and mouth that are often seen in paediatric SSSS are not observed in the present patient. (B–D) Membranous blister roofs, erosive plaques and shallow flaccid bullae are seen on the whole body. Even skin that appears normal in colour shows diffuse superficial blister formation (B: an upper limb; C: a lower limb; D: the back). (E, F) Flaccid bullae and purpuric plaques are observed on the right lower leg (arrow indicates the biopsy site) (E) and the left thigh (F), indicating necrotic lesions of the skin.
On histopathological examination, blister formation was observed under the stratum corneum in the lesions with flaccid bullae, consistent with SSSS (Fig. S1A). The purpuric lesions on the right calf (Fig. 1E) and left thigh (Fig. 1F) revealed bacterial colonies in the upper epidermis, necrosis of the epidermis and the dermis, and neutrophilic infiltration from the epidermis to the adipose tissue, consistent with an abscess with necrotic tissue (Fig. S1B).
Blood examinations showed total leukocytes of 2,400/µl, serum blood urea nitrogen of 3 mg/dl, serum creatinine of 2.13 mg/dl, serum aspartate aminotransferase of 96 IU/l, serum alanine aminotransferase of 41 IU/l, serum creatinine kinase of 5,155 IU/l, C-reactive protein of 28.41 mg/dl, procalcitonin at 96.6 mg/dl, international normalized ratio of prothrombin time of 2.08, fibrinogen of 786 mg/dl, D-dimer of 60.4 µg/ml, and fibrin degradation products of 143 µg/ml. Peripheral blood, synovial fluid samples from the right knee and necrotic tissues from the thigh were subjected to bacterial culture. From all of these samples, methicillin-sensitive S. aureus (MSSA) was cultured and was characterized as positive for ET A and negative for toxic shock syndrome toxin-1, staphylococcal enterotoxins A through D, and endotoxin. Panton–Valentine leukocidin was not detected in the strain of MSSA isolated from the patient’s blood by previously reported PCR methods (2). In addition, magnetic resonance imaging (MRI) scan revealed discitis and an epidural abscess at L3/L4 (Fig. S1C, D). Based on these results, the patient was diagnosed with SSSS resulting from MSSA septic arthritis of the right knee.
The patient was transferred to the emergency room (ER) of our hospital early in the morning. Shortly after her arrival, meropenem (1 g every 8 h) was started, and then daptomycin (500 mg every 24 h) was additionally administered. Continuous haemofiltration was started from the early afternoon. However, the patient’s general condition was serious, and it worsened despite the treatments. Thus, we started 5,000-mg IVIG therapy in the evening of that day. MSSA was detected by blood culture late at night, and the regimen was switched to cefazolin (2 g every 8 h) and clindamycin (600 mg every 4 h) from the morning of the next day. Regarding the clindamycin, we expected it to have an anti-toxinic effect in addition to its antibiotic effect. IVIG therapy was continued for 3 days to treat the SSSS by neutralizing the toxins. The kidney injury was known to be a side-effect of the IVIG. As the patient showed acute renal failure at admission, we provided adequate fluid replacement and monitored renal function carefully while administering the IVIG. Concurrently, the right knee joint was drained, and continuous haemofiltration was performed for 8 days. After these multimodal treatments were started, the patient’s general condition, skin symptoms and blood test results improved dramatically. The epidural abscess was managed successfully with non-surgical treatment. The patient was discharged from the intensive care unit (ICU) on day 20 with normal renal function.
Adult SSSS and TEN both show high mortality rates, but they are treated with completely different methods (3). Therefore, it is important to make a differential diagnosis as quickly as possible at the patient’s first examination. Our patient presented a rash primarily composed of shallow erosions and flaccid bullae without fresh erythema, and she did not have enanthema. The absence of mucous membrane involvement was an important finding that ruled out TEN. Histopathological examination also revealed subcorneal splitting without the epidermal necrolysis that is characteristic of TEN. Based on the clinical and histopathological findings, we made a diagnosis of SSSS. The results of bacterial cultures and blood tests were consistent with the diagnosis.
The pathogenic bacteria in this patient seemed far more aggressive than those described in previous reports of adult SSSS (4–9). The foci of infection spread haematogenously to produce skin infections at the right lower thigh and the left thigh, as well as discitis and an epidural abscess at L3/L4. The bacteria detected in the wound culture were identical to those detected in the cultures from the blood and skin, indicating that the infection had spread haematogenously to the skin. Risk factors for SSSS in adults are immunosuppression and renal failure (3). The patient had been taking methotrexate weekly for a long time. Acute renal failure due to septic shock might have exacerbated her SSSS manifestations.
In the present case, in addition to antibiotics, IVIG had a favourable course and enabled us to save the patient’s life. IVIG administration has been tried as a way of neutralizing ETs in SSSS, but it has been reported as successful in only one paediatric case (10). The present case is the first reported adult patient with SSSS treated successfully with IVIG.
IVIG preparations reportedly contain higher titres of anti-ET A antibodies than of anti-ETB antibodies (11). Rates of anti-ET A antibody carriers vary by age. The anti-ET A antibody carrier rate in children from 3 months to 2 years of age is only 30%, but the carrier rate in individuals from 50 to 80 years of age is 91% (12).
In previous reports, 89%, 4% and 8% of S. aureus strains isolated from children with SSSS produced ET A alone, ET B alone and both ET A and ET B, respectively (13). Only 9 adult cases of SSSS with the data of ET serotypes have been reported in Japan, including in the Japanese literature (14, 15). Of these, only one patient had an ET A-producing strain, whereas the other 8 had ET B-producing strains. The fact that most adult SSSS cases are caused by ET B-producing strains might be associated with high carrier rates of anti-ET A antibodies in adults. The present patient’s SSSS was caused by an ET A-producing strain, which is very pathogenic in adult cases of SSSS, and the favourable results of the IVIG therapy may be associated with a high titre of anti-ET A antibodies in the IVIG preparations.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize