


Department of Dermatology, Odense University Hospital, Søndre Blvd 29, DK-5000 Odense C, Denmark. E-mail: trinehoegsberg@yahoo.dk
A 51-year-old woman was hospitalized due to an itchy, generalized rash, which had been present for 5 days. She had concomitant sore throat, oral lesions and some genital irritation. Before admission, she had visited her family practitioner and emergency service, where she was prescribed nobligan. A practicing dermatologist suspected vasculitis and took a skin biopsy.
No known exposures could be identified. She was working as a teacher for adults, and did not know of any people with infections in her social circle. For 2 years she had been treated with a stable dose of escitalopram.
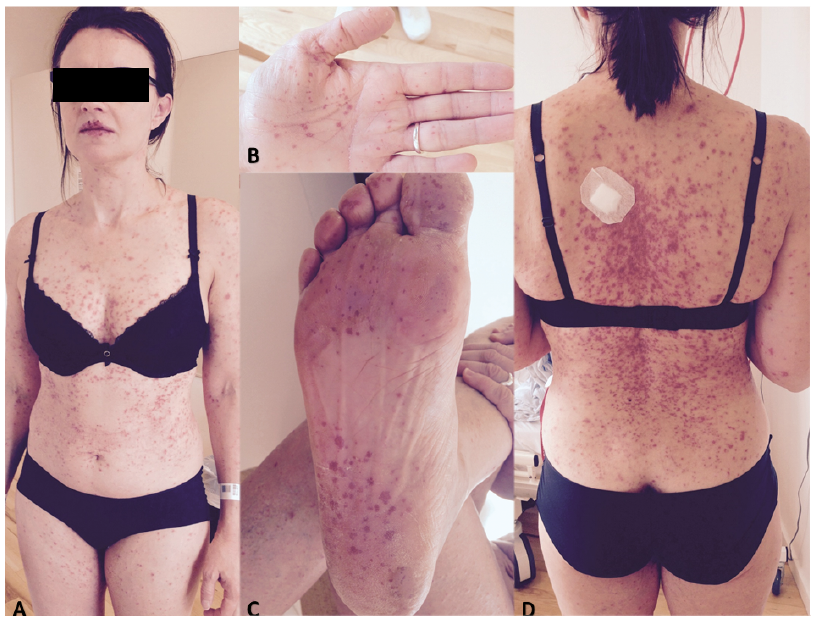
Clinical examination revealed multiple red papulovesicular and pustular lesions distributed mainly on the trunk, but also to a lesser extent on the limbs including the palms and soles (Fig. 1). She had vesicles and small erosions around her lips and inside her mouth, general malaise, retrosternal pain on swallowing, and had been vomiting. She had no fever and had reported no other complaints. Blood testing showed mild lymphopenia and marginally raised C-reactive protein 27 (< 6).
Skin biopsy revealed extensive necrosis of the epidermis with a few scattered lymphocytes. Dermal oedema was seen with a lymphocytic infiltrate, but no signs of vasculitis. Histopathology suggested erythema multiforme or toxic epidermal necrolysis.
What is your diagnosis? See next page for answer.
Fig. 1. Multiple papulovesicular lesions confluent on the trunk and centred around the mouth and macular punctate lesions on the palms and soles. Written permission was provided by the patient to publish these photographs.
Acta Derm Venereol 2018; 98: xx–xx.
Diagnosis: Atypical hand, foot, and mouth disease caused by echovirus 3
The clinical picture was suspicious of atypical hand, foot, and mouth disease (HFMD), which can also occur in adults. This condition is most often caused by coxsackievirus A6 and may manifest as eczema coxsackium in people with a background presence of eczema. Typical HFMD is caused by coxsackievirus A16 or enterovirus A71. In this case PCR analysis of a stool sample revealed echovirus 3, another enterovirus. Echoviruses are infrequently reported in human disease, and we could only find 12 reports in the literature of vesicular rashes caused by echovirus (1–12). Ten of these publications referred to children from Thailand, China, Malaysia, Brazil, Spain or Germany with HFMD caused by echovirus 3, 4, 7, 9, 11, 19, 24, 25 or 71. To our knowledge, there have been no reported cases of echovirus 3 infection associated with atypical HFMD in an adult. The patient’s condition improved spontaneously within 2 weeks.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize