


1Center for Chronic Pruritus, Department of Dermatology, University Hospital Münster, Münster, 2Department of Dermatology, Fachklinik Bad Bentheim, 3Dermatological Practice, Bad Bentheim, 4Department of Dermatology, Klinikum Dortmund GmbH, Dortmund, Germany, and 5Itch Center Department of Dermatology and Cutaneous Surgery, University of Miami Hospital, Miami, FL, USA
Prurigo nodularis (PN) is a subtype of chronic prurigo presenting single to multiple symmetrically distributed, hyperkeratotic and intensively itching papules and nodules. PN evolves along with chronic pruritus in the context of diverse dermatological, systemic, neurological or psychiatric conditions. Permanent scratching is possibly a major trigger of PN, although its exact pathophysiology remains unclear. Current state-of-the-art therapy for PN consists of topical steroids, capsaicin, calcineurin inhibitors, ultraviolet (UV) therapy, systemic administration of gabapentinoids, μ-opioid receptor antagonists, antidepressants or immunosuppressants. Novel treatment concepts, such as inhibitors of neurokinin-1, opioid and interleukin-31 receptors, have been developed and are currently being clinically tested.
Key words: itch; pruritus; chronic scratch lesions; prurigo nodularis; Hyde’s prurigo; interleukin-31; neurokinin-1.
Accepted Aug 23, 2017; Epub ahead of print Aug 23, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Claudia Zeidler, Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: claudia.zeidler@ukmuenster.de
Prurigo nodularis (PN) is a highly pruritic, chronic disease clinically defined by the existence of many, usually symmetrically distributed, hyperkeratotic and erosive papules and nodules (1). PN evolves along with consistent scratching in patients with chronic pruritus, and is a subtype of chronic prurigo (CPG), which was defined recently by members of the European Academy of Dermatology and Venereology (EADV) Task Force Pruritus group, as a skin disease due to neuronal sensitization to itch and development of an itch–scratch cycle (2). The debate on the nature of CPG was initiated over 100 years ago after the first description of PN by Hyde (3), and is ongoing, as relevant aspects of the pathogenesis of CPG remain unclear (4). Part of the confusion is the use of the term “prurigo” for other not-primarily itch-related skin diseases (e.g. actinic prurigo), but also for scratching-related dermatoses. An attempt has been made recently to classify subtypes of CPG based on clinical criteria, differentiating between several types, such as papular, nodular, plaque or umbilicated prurigo, signifying the generally increased acceptance of this terminology (1). An important aspect of this terminology is the acceptance that the presence of CPG should initiate proper treatment and diagnosis of potential underlying diseases that might trigger scratching (5). The itch–scratch cycle in CPG appears to be linked to pruritus induced by various disorders, with 50% of PN patients showing an atopic predisposition (6). Other dermatoses, as well as various systemic diseases, infections, neurological and psychiatric disorders, are also known to cause PN (5). Most patients then develop the vicious itch–scratch cycle that is difficult to treat with existing therapies. Itch intensity in PN is thought to be the highest among the different types of chronic itch (5, 7), resulting in reduced quality of life, including sleep disturbances and psychiatric comorbidities (8).
This review summarizes current knowledge and recent findings on the clinical presentation and therapeutic management of PN, discusses ongoing research and indicates areas of future research needs.
Epidemiological data regarding the incidence and prevalence of PN are lacking. Based on observations from case series, all age groups, including children (9) can be affected by PN, but elderly people are the most frequently affected (5). Furthermore, African Americans with atopic eczema appear to have more PN lesions than other racial groups (10). No conclusion can be drawn on differences between the sexes, as these results have not been reported consistently (5).
Cutaneous inflammation and neuronal plasticity appear to play an important role in PN, but the exact pathogenesis of the condition remains unclear (11).
In 1934, Pautrier (12) observed the presence of neural dermal hyperplasia (Pautrier’s neuroma) in PN. Thirty-five years earlier Johnston described hypertophy of dermal nerve fibres in a papular dermatitis (13).
Histopathological studies revealed increased dermal nerve fibre density and changes in many types of skin cells, including mast cells, collagen fibres, Merkel cells, epidermal keratinocytes, dendritic cells and endothelial cells (14–16). The aforementioned cells cause inflammation and pruritus through the release of tryptase, interleukin-31 (IL-31), prostaglandins, eosinophil cationic protein, histamine, and neuropeptides, such as substance P, calcitonin gene-related peptide (CGRP) and nerve growth factor (NGF) (16–19). In fact, PN skin biopsies exhibit a 50-fold upregulation of IL-31 mRNA compared with healthy skin biopsies (20). Studies in mouse models showed that the T-cell-derived cytokine IL-31 induces severe pruritus and inflammation (21) by binding to a heterodimeric IL-31 receptor (IL-31 receptor A and oncostatin M receptor subunits) at transient receptor potential cation channels subfamily V or A member 1 (TRPV1+/TRPA1+) C fibres, keratinocytes, macrophages and eosinophils (22). By contrast, the lack of response to antihistamines, indicates that histamine is probably not a major mediator of PN, as it had been considered previously (23). The increased expression of NGF (24) indicates that a substance P-induced signal may contribute to neuronal and dermal hyperplasia (25). Similarly, overexpression of CGRP leads to neurogenic inflammation via the regulation of inflammatory cells, such as eosinophils and mast cells (26).
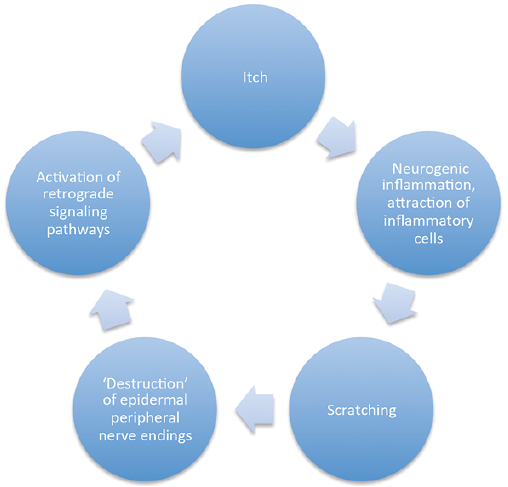
In contrast to observations in the dermis, hypoplasia of sensory nerves has been reported in the epidermis of PN skin, including interlesional skin, in comparison with healthy skin (16, 27). Moreover, restoration of epidermal nerve fibre density was detected in biopsies of healed nodules (27). A functional study did not detect signs of neuropathy of small fibres in patients with PN (28). Thus, it is likely that the reduced epidermal nerve fibre density is the result of repeated scratching rather than of small fibre neuropathy (27) (Fig. 1).
Fig. 1. Itch-scratch cycle and possible pathophysiology of prurigo nodularis.
PN is characterized by hyperkeratotic, crusted or excoriated, light-red to bright-red papules, nodules or plaques with hyperpigmented borders. Skin lesions may range from a few to hundreds, and their size can range from a few millimetres to 2–3 cm. PN can manifest in circumscribed areas, but in most cases is generalized with symmetrical distribution of the lesions on the extensor surfaces of the extremities and the trunk. On the back, the areas that are free of lesions due to the inability of patients to reach them and to scratch, form the so-called ‘’butterfly sign’’ (Figs 2–4) (1, 11, 29). PN is highly pruritic, with a mean numerical rating scale (0–10) score of 8. Most patients mention more than one quality of pruritic sensation, i.e. a combination of stinging, burning, tingling, heat and cold, independent of the aetiology of PN (5).
In addition to the visible and sensorial symptoms, PN has considerable impact on the quality of life of patients, often leading to sleep disturbance, psychological distress, behavioural/adjustment disorder and social isolation (30, 31).
Fig. 2. Prurigo nodularis due to atopic predisposition in a 47-year-old woman with typical distribution of lesions including the “butterfly sign” (no lesions on the centre of the back).
Fig. 3. Prurigo nodularis in a 73-year-old patient due to diabetes mellitus.
Fig. 4. Prurigo nodularis: treatment algorithm (59). RCT: randomized controlled trial; UV: ultraviolet; PUVA: psoralen plus ultraviolet; NK1R: neurokinin-1 receptor.
Different inflammatory dermatoses have been observed in association with PN, with atopic eczema being the most frequent (32). These dermatoses evolve with itch and subsequently the itch–scratch cycle promotes PN. Accordingly, PN may coexist with inflammatory dermatoses or continue after their cessation. This association is sometimes described in terms such as “pruriginous atopic eczema”, reflecting the synchronism and biological connection between the conditions. Many patients have PN with an atopic background with no signs of an active dermatosis (Fig. 2).
Although rare, pruritic cutaneous T-cell lymphoma, dermatitis herpetiformis and lichen planus also have the potential to trigger PN (5). In some patients, especially in elderly people, PN lesions may present the initial clinical sign of incipient bullous pemphigoid (33, 34). Therefore, in case of doubt, performing direct immunofluorescence is recommended for diagnosis (35).
Many systemic and neurological diseases can result in PN, the most common of which are presented below.
Approximately 18–60% of patients with chronic kidney disease can be affected by chronic itch depending on the region and the definition of itch (36–38). In a study of patients with chronic pruritus due to chronic renal failure, over half of the patients exhibited PN and were those who suffered for longer time from renal failure (39). According to a representative prospective cross-sectional study in patients attending dialysis units (GEHIS), 10% of hemodialysis patients demonstrated excoriations and scratched nodules with the typical clinical picture of PN (40).
Diabetes mellitus is also associated with PN (Fig. 3) (41). In the case of both, chronic renal failure and diabetes mellitus, PN lesions frequently appear with central ulcerations, resembling Kyrle disease (42, 43). The latter was recently attributed to be a variant of PN (44). Interestingly, chronic pruritus associated with liver disease rarely leads to the formation of PN (45).
Infections, especially HIV, are often associated with PN (46). It is notable that the severity of PN correlates with a lower level of CD4 cells. Areas of high HIV prevalence may also indicate a high prevalence of PN. Following antiretroviral treatments, the symptoms of PN usually improve (47).
Neuropathic diseases can result in localized PN caused by damage to cutaneous or extracutaneous nerves (48). PN can occasionally appear in the context of a post-herpetic neuralgia (49), but also due to other neuropathic forms of chronic pruritus; for example, brachioradial pruritus mostly localized in the dermatome C5/C6 (50).
Depression and anxiety, as well as tactile hallucinations, can induce psychogenic pruritus and thereby lead to PN (51). This must be distinguished from skin-picking disorder, in which patients manipulate (including scratching) the skin without primarily perceiving pruritus (52). Skin-picking disorder is often correlated with pathological behaviours and/or mental disorders, thus emphasizing the importance of identifying the underlying illness (52).
Treating PN remains challenging as long as data from randomized controlled trials (RCT) are sparse (Table I). An individual treatment plan needs to be established, taking into consideration age, underlying disease, comorbidities, severity of PN, quality of life impairment, and expected side-effects (30). This usually requires a multimodal treatment algorithm, consisting of topical and systemic therapies to address all above-mentioned aspects (Fig. 4) (30). Symptomatic therapy should follow 2 objectives: reduction of itch and complete healing of PN lesions. General measures, for instance the use of an emollient as the basis of therapy, are recommended.
Table I. Treatment of prurigo nodularis based on literature reviews
Topical steroids, pimecrolimus, and calcipotriol are the only topical therapies investigated so far in RCT with PN patients (Table I).
Betamethasone 0.1% cream significantly reduced itch (visual analogue scale (VAS 0–10) before treatment 8.8, VAS after treatment 3.9) in comparison with an antipruritic moisturizing cream (VAS 5.6 after treatment) (Table I), and also resulted in nodule flattening (53). In addition, direct injection of triamcinolone acetonide into the nodules resulted in clinical improvement (54). In inflamed pruriginous lesions, topical steroids can also be combined with an occlusive dressing (55).
Topical calcineurin inhibitors represent a relatively long-term treatment option. Treatment with pimecrolimus led to similar improvement in itch as treatment with hydrocortisone (VAS before 7.1; VAS after pimecrolimus 4.4; p < 0.001; VAS after hydrocortisone 4.5; p < 0.001) and to distinct amelioration of PN (Table I) (56).
With regard to vitamin D derivatives, calcipotriol ointment significantly decreased the number of PN lesions in comparison with betamethasone valerate (Table I) (57).
Topical capsaicin inhibited pruritus in localized, neuropathic forms of PN and improved the skin condition (58, 59). Another treatment used in the USA, which targets the transient receptor potential channels in the same way as capsacin, is a combination of topical ketamine and amitriptyline (60).
UV phototherapy is a viable therapeutic option, in particular for elderly patients with multi-morbidities and multi-medications. Here, several UV therapies have been reported, such as psoralen plus UVA (PUVA), UVA, and UVB (61–63); in addition, a common and effective option is narrow-band UVB (62).
An accelerated healing process has been observed after combination treatment with a 308-nm excimer laser and PUVA (61). A modified Goeckerman regimen, consisting of daily multi-step broadband UVB therapy followed by the application of crude coal tar and topical steroids under occlusion, was also found to be effective (62). Nevertheless, as the carcinogenic potential of tar is still being discussed, this treatment regimen should be used with caution and only in selected patients (63).
Antihistamines. Antihistamines are often used in PN treatment regimens due to the increased numbers of mast cells found in PN lesions. A high-dose non-sedating antihistamine, in combination, if needed, with a sedating antihistamine at night, showed some effect in case series (64). In combination with leukotriene inhibitors, antihistamines decreased the number of PN lesions from between 10 and 290 (mean 107.6) before treatment to between 0 and 154 (mean 42.7) at treatment end (65). However, these were only single reports; the majority of experts agree that antihistamines are not sufficiently effective in PN (30, 66). There is a lack of systematic analyses and RCT of antihistamines in PN.
Gabapentinoids. The addition of gabapentinoids, such as gabapentin and pregabalin, in the treatment scheme of PN should be considered only if other therapies have failed. As proven in RCTs these substances are successfully used in chronic pruritus (67). In PN, improvement has so far been reported only in case series (68, 69). The exact mechanism of action is not yet understood. Stabilization of the spinal nerve membrane by calcium channel blockage, inhibition of glutamate synthesis, or reinforcing of the GABA inhibitory mechanisms so that incoming signals are stopped at the presynaptic membrane, are possible mechanisms (70). When prescribing, the side-effects profile, as well as dosage adjustments for elderly patients and those with renal failure should be taken into account.
Opioid receptor antagonists. Antagonists of the μ-opioid receptor, such as naloxone (intravenous) or naltrexone (oral), demonstrated efficacy in PN (71). An RCT reported significant decrease in itch intensity in cholestatic PN (72). In case series, 67.7% of patients with PN of dermatological origin reported improved symptoms and 38% reported complete healing (71). Despite efficacy, side-effects, such as dizziness and vomiting during the first days of application, must be considered. Combination treatments of κ-opioid receptor agonists with μ-opioid receptor antagonists, such as butorphanol, may also have a beneficial effect on PN (Table I) (73).
Antidepressants. Antidepressants, such as paroxetine, amitriptyline or mirtazapine, showed positive effects in patients with severe PN. In a 2-arm proof of concept study with either paroxetine or fluvoxamine, scratch lesions healed partially or completely in most patients, while the intensity of pruritus decreased significantly (Table I) (74).
Immunosuppressants. After careful consideration of the risk–benefit profile, immunosuppressants can also be considered as a therapeutic option for patients with severe PN. A number of case series described the application of immunosuppressive agents, such as cyclosporine in PN, showing remarkable symptom improvement (75, 76). During immunosuppressant therapy, it is important to monitor blood pressure and laboratory values, especially those of the kidneys. Several cases series describe the use of thalidomide, a neurotoxic and teratogenic drug, for PN (77, 78). A recently published review (79) analysed data from 280 patients with pruritus, mostly due to PN, treated with thalidomide. PN and itch intensity improved in most patients, but the incidence rate of peripheral neuropathy was approximately 20% in the first year of treatment (79). Because of this side-effect thalidomide is commonly a last choice for most severe cases. Lenalidomide, a second-generation thalidomide analogue, decreased pruritus and PN lesions in case reports with conflicting results regarding its neurotoxicity (Table I) (80, 81).
Treatment of PN related to atopic dermatitis, with immunoglobulins in combination with methotrexate, had an antipruritic effect (82).
Based on current understanding of the pathomechanism of PN, targeting the increased levels of IL-31, receptors for substance P and for opioids appear to be promising treatment approaches.
Recent RCTs have investigated the efficacy of the neurokinin-1 receptor antagonists aprepitant (German register: DRKS00005594) and serlopitant (VPD-737; ClinicalTrialGov: NCT02196324) in PN. The latter demonstrated significant itch reduction in the majority of patients with PN (Ständer; unpublished data), as did aprepitant in a previous case series (83).
An RCT, currently running in the US and Europe, is assessing the efficacy of nalbuphine, a dual opioid receptor μ-antagonist/κ-agonist, in PN (NCT02174419) and appears to be promising. In uraemic pruritus, the use of nalbuphine resulted in a reduction in itch intensity, as demonstrated in an RCT (84).
Future studies in PN will investigate the antipruritic effect of blocking IL-31 at the corresponding receptor. In atopic dermatitis, a similarly itchy disease, the monoclonal antibody nemolizumab has resulted in clinically meaningful improvement in symptom (85, 86).
Chronic prurigo, including its subtypes, such as PN, is an itch–scratch cycle related disease based on neuronal sensitization processes. As long as the pathophysiology of PN is not completely clear, its management will represent a therapeutic challenge. It is hoped that the multiple ongoing RCTs on novel targets, such as IL-31, neurokinin-1 and opioid receptors, will lead to effective treatments for this intractable disease with persistent, chronic itch.
The authors would like to thank the German Federal Ministry of Education and Research (BMBF; No. 01KG1305 to AT and SST) and the European Academy for Dermatology and Venereology (EADV, No. 2016-012 to MP) for their support for this work, Galderma International financial support for this publication, and Helena Karajiannis for assistance in preparation of the manuscript.
Conflicts of interest. SS received advisory honoraria from Almirall, Beiersdorf, Chugai Pharma, Creabilis, Daiichi Sankyo, Galderma, Helsinn, Kneipp, Maruho, Merz, Nerre, Trevi, Vanda, Menlo, Ziarco. GY received honoraria as consultant for advisory board work and as investigator from Trevi, Opko, Menlo, Creabilis, Chugai Pharma, Pfizer, Eli Lilly, Celgene, Anacor, Tioga, Roche, GSK, J&J, and LEO Foundation.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize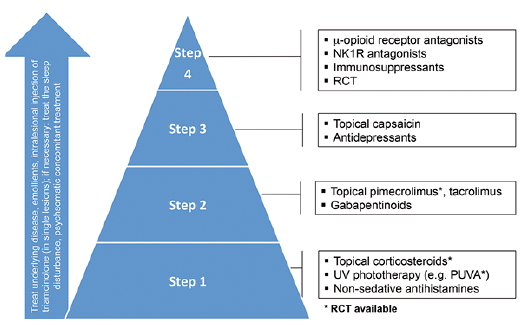 Click to show fullsize
Click to show fullsize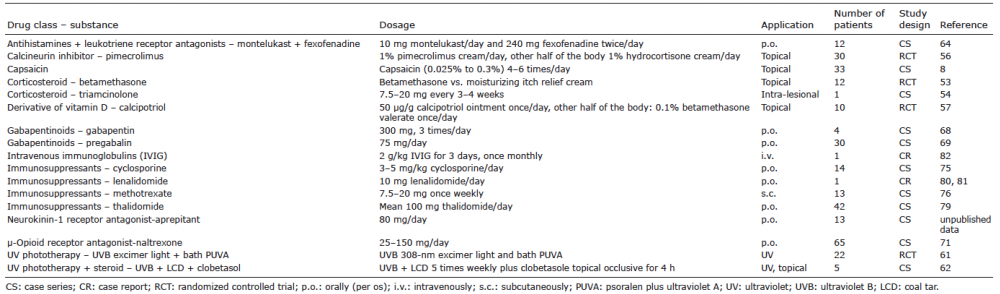 Click to show fullsize
Click to show fullsize