


1Department of Dermatology, Division of Immunology, Allergy and Infectious Diseases, Medical University of Vienna, AT-1090 Vienna, Austria, and 2Department of Infectious Diseases, National Reference Centre for Staphylococci and Enterococci, Division Nosocomial Pathogens and Antibiotic Resistances, Robert Koch Institute, Wernigerode, Germany. E-mail: simona.saluzzo@meduniwien.ac.at
#These authors contributed equally.
Accepted Aug 29, 2017; Epub ahead of print Aug 30, 2017
Staphylococci may cause severe infections in children and immunocompromised adults (1). Staphylococcal scalded skin syndrome (SSSS), for example, is a potentially life-threatening disease caused by the haematogenous spread of exfoliative toxins (ET) of Staphylococcus aureus termed ET-A, ET-B or ET-D (2) and encoded by the respective chromosomal (eta, etd) and plasmid located genes (etb) (3); bullous impetigo (BI), on the other hand, results from the local impact of the very same exfoliatins. We report here a case of a SSSS caused by a rare ET-A-producing S. aureus strain in an adult woman affected by chronic lymphocytic B-cell leukaemia (CLBCL).
A 63-year-old woman presented with fever and a bullous skin eruption. She reported the intake of antibiotics one week earlier (amoxicillin and sulbactam) because of an upper airway infection. Her past medical history was remarkable for CLBCL, currently being treated with Ibrutinib. The patient had vesiculobullous lesions on an inflamed basis on her face, neck, trunk and left arm (Fig. 1A, B). Only a few blisters were intact; most were ruptured. Differential diagnoses included SSSS, a generalized variant of BI, toxic epidermal necrolysis (TEN), pemphigus vulgaris (PV) and toxic erythema of chemotherapy (TEC).
Fig. 1. Clinical course. (A) Flaccid bullae formation of face, neck, trunk and left arm. (B) Twenty days after initiation of antimicrobial therapy, lesions were healed without scarring. A written permission from the patient is given.
Physical examination revealed fever (38°C) and crepitation on thorax auscultation. A chest X-ray was diagnostic for pneumonia of the left lower lobe. The Tzanck test from a bullous lesion showed acantholytic cells with no sign of necrosis, making TEN unlikely. The Nikolsky sign was positive on clinically normal-appearing skin. Primary laboratory findings revealed elevated C-reactive protein of 20.88 mg/dl (normal < 0.5) and 9% relative band neutrophils (normal 3.0–5.0%). We observed hypoimmunoglobulinaemia, with IgG 340.0 mg/dl (normal 700–160), IgA 28.5 mg/dl (normal 70–400) and IgM 6.6 mg/dl (NR, 40–230).
Perilesional histology of a fresh bulla showed a neutrophilic infiltrate in the upper dermis, spongiosis and acantholytic split formation in the stratum granulosum (Fig. 2A). A search for pemphigus antibodies yielded negative results. A gram stain of lesional skin revealed gram+ cocci in the split (Fig 2B). Bacterial cultures from blood and sputum, as well as swabs of the nose and lesional skin, were positive for methicillin-sensitive S. aureus (MSSA). DNA sequencing of the S. aureus-specific staphylococcal protein A (spa) and multi-locus sequence-typing (MLST) revealed spa-type t729, sequence type (ST) 88 for all isolates. Strains were positive for the gene encoding the exfoliative toxin A (eta). A diagnosis of SSSS was made and the patient received intravenous piperacillin-sulbactam (4.5 g i.v. 3 times daily for 10 days) until complete remission (Fig. 1B).
Fig. 2. Perilesional histology of a fresh blister. (A) Haematoxylin and eosin (H&E) stain of a paraffin-embedded skin biopsy (upper left). Higher magnification reveals an exposed granular layer (upper right), spongiosis and subcorneal split formation (lower left), as well as a dense neutrophilic infiltration of the papillary dermis (lower right). (B) Gram stain of the skin biopsy showing Gram-positive cocci.
ET-A producing MSSA with spa-type t729/ST88 are ex- tremely rare in Europe. The National Reference Center for Staphylococci and Enterococci in Germany reported 68 cases of SSSS in the period 2014–2015, among which none of the ET-A-positive S. aureus strains were affiliated with spa-type t729. A French study of 349 cases of SSSS (in the period 1997–2007) reported no t729 strain (4). Among S. aureus nasal carriage studies performed in Germany and the Netherlands, only one strain with similar characteristics was reported in the community (5).
S. aureus strains ST88 are found more frequently in African countries and, in addition to MSSA, methicillin- resistant isolates are also reported (6).
The occurrence of SSSS in our patient was probably not fortuitous. Recent evidence suggests an impaired bactericidal function of polymorphonuclear cells in patients affected by CLL (7), potentially explaining the susceptibility to gram+ septicaemia. Moreover, an impaired humoral response favours the septic spread of S. aureus both in children and immunocompromised adults (8). Therapeutic strategies to cure SSSS using intravenous immunoglobulins or direct elimination of the Toxin via Plasma exchange have proved successful (9, 10). A recent report suggests a role of Langerhans cells in providing a pre-emptive humoral protection against surface exfoliatin toxins, even before they can breach the tight junction causing systemic disease (11). Topical vaxination strategier that take advantage of antigen presentation through tight junktion by Langerhans cells might be useful in reducing the incidence of SSSS in immunocompromised patients and children.


 Click to show fullsize
Click to show fullsize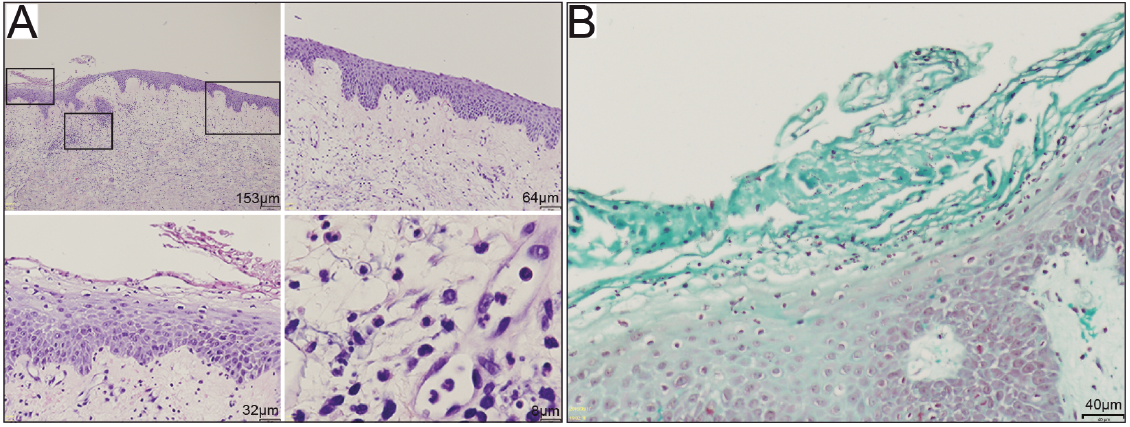 Click to show fullsize
Click to show fullsize