


1Department of Dermatology and Venereology, and 2Department for Biometrics and Medical Informatics, Otto-von-Guericke University Magdeburg, Magdeburg, Germany
Differential diagnosis of palmoplantar non-pustular psoriasis and chronic allergic contact dermatitis (ACD) and the combination of these conditions, termed “eczema in psoriatico” (EIP), is difficult, especially in cases of isolated involvement. A blind re-evaluation of 63 archived formalin-fixed palmoplantar samples, previously diagnosed clinically as either psoriasis or
chronic ACD, was performed. Samples were allocated to histopathological diagnoses of psoriasis, contact dermatitis or EIP. Immunohistological stainings were performed for better characterization. Immunochemistry of EIP revealed features that overlapped contemporarily with psoriasis (cytokeratin 17 (CK17), Ki67, interleukin (IL)-8, IL-17, IL-23) and with ACD (CD1a, major histocompatibility complex (MHC) class I, MHC class II, epidermal T-cell subsets). Surprisingly, a significantly much higher number of dermal CD8+ T cells was found in EIP than in ACD and psoriasis. In conclusion, this study provides insight into the immunohistological differentiation of palmoplantar psoriasis, chronic ACD and EIP.
Key words: eczema in psoriatico; palmoplantar; allergic contact dermatitis; psoriasis; immunohistology.
Accepted Aug 29, 2017; Epub ahead of print Aug 30, 2017
Acta Derm Venereol 2018; 98: xx–xx.
Corr: Malgorzata Kolesnik, Department of Dermatology and Venereology, Otto-von-Guericke University Magdeburg, Leipziger Str. 44, DE-39120 Magdeburg, Germany. E-mail: malgorzata.kolesnik@med.ovgu.de
Differential diagnosis of palmoplantar non-pustular psoriasis and chronic contact dermatitis is often difficult if other characteristic signs and history are missing. Typical histological patterns are often lacking in the palmoplantar localization (1). Furthermore, these 2 conditions have similar histological features, such as acanthosis, parakeratosis and spongiosis.
The concept of eczematous psoriasis has been discussed previously (2, 3). However, there are conflicting results regarding the correlation of psoriasis and contact sensitivity. Some authors have observed an inverse relationship (4), while others have reported a higher incidence of type IV sensitization only in palmoplantar psoriasis (5, 6). Another study noted a positive correlation with the duration of the disease, but not with the site of lesions (7).
Psoriasis and allergic contact dermatitis (ACD) can influence each other’s course and clinical picture. It has been shown (8) that occurrence of the ACD reaction in patients with psoriasis sensitized to nickel is delayed and that it resolves more slowly than in patients without psoriasis. Furthermore, mixed histological and immunohistological patterns have been observed in cases of ACD on top of pre-existing psoriasis, combining both psoriasis and eczema. After self-limitation of an artificially induced ACD reaction, the course of psoriasis was unaltered.
A group of patients with palmoplantar lesions and type IV sensitization, contemporarily showing clinical and histological features of both psoriasis and contact dermatitis, has been indentified in our Department of Dermatology. This constellation (Fig. S1a–c) is termed “eczema in psoriatico” (EIP) (9).
The aim of the current study was to compare the clinical, histological and immunohistological characteristics of patients with EIP with those diagnosed with palmoplantar psoriasis or ACD alone.
Patient selection is described in the study flow chart (Fig. S2). Intralesional punch biopsies were obtained from patients during routine diagnosis, after obtaining written, informed consent and in accordance with the principles of the Declaration of Helsinki. Two experienced dermatopathologists performed a blind re-evaluation of 132 histopathology sections from the palmoplantar localization stained with haematoxylin and eosin (H&E), which had been clinically diagnosed previously as either psoriasis or chronic contact dermatitis. They allocated the samples a diagnosis of psoriasis, contact dermatitis or EIP.
Clinical data and allergy tests were examined retrospectively. Patients presented with well-demarcated scaling palmoplantar erythema. Additional findings, such as erythematous plaques on the elbows, knees or scalp, and oil spots, favoured a diagnosis of psoriasis. Nummular, papulo-vesicular lesions in localizations other than palmoplantar favoured a diagnosis of eczema.
All patients (except for the control group and 4 patients with psoriasis) had been investigated previously with the German baseline series of contact allergens (Almirall Hermal, Reinbeck, Germany). Patch tests were interpreted according to the guidelines of the International Contact Dermatitis Research Group (10). Evaluation of total IgE in serum was based on fluorescence-enzyme immunoassay and investigated by UniCAP 250 EliA (Phadia, Freiburg, Germany). Proven contact sensitization was an inclusion criterion in the group with ACD and EIP.
Cases with irritant, non-allergic palmoplantar manifestations, and those with isolated atopic hand dermatitis and pustulosis palmoplantaris of any type were excluded from the study.
From this collection of samples, a final selection resulted in 63 specimens from 59 patients, for which both experts agreed on the diagnosis: 33 with EIP, 13 with ACD and 12 with psoriasis. Five samples of healthy skin with a palmoplantar localization served as negative controls.
Immunochemistry was performed on formalin-fixed, paraffin-embedded tissue blocks. The following primary antibodies were used: CK16 (1:500; Clone LL025; Abcam, Cambridge, UK), cytokeratin 17 (CK17) (1:100; CK-E3; BioSystems, Pleasanton, CA, USA), filaggrin (1:100; Clone FLG01; GeneTex, Irvine, USA), major histocompatibility complex (MHC) class I (1:1250; Clone EP1395Y; Abcam), MHC class II (1:200; monoclonal; Abcam), CD1a (1:15; JPM30; Leica Biosystems, Newcastle, UK), Ki67 (1:100; Clone MIB-1; Dako, Hamburg, Germany), CD4 (pure; Clone 4B12; BioGenex, Fremont, CA), CD8 (pure; Clone 144B; BioSystems), interleukin (IL)-8 (1:200; Clone 6217; R&D Systems, Minneapolis, MN, USA), IL-17 (1:300; polyclonal; Abcam), IL-23 (1:500; polyclonal; Abcam).
Paraffin skin sections (3 µm) were deparaffinized and heated for antigen retrieval in citrate buffer pH 6 in case of CK16, filaggrin, IL-17, IL-23 and ethylenediaminetetraacetic acid (EDTA) buffer pH 9 in case of CK17, MHC I, MHC II, CD1a, Ki67, CD4, CD8, and IL-8.
The background stainings of MHC I and II were blocked using Protein Blocking ProTaqs (BIOCYC, 400104695). In case of IL-17, sections were quenched with 0.25% Tween 20 (Sigma, Schnelldorf, Germany) in 1× phosphate buffer solution (PBS) for 10 min and then blocked with 10% foetal calf serum (Invitrogen, Heidelberg, Germany), 1% bovine serum albumin and 0.25% fish skin gelatine (both Sigma) in PBS for 1 h.
For detection of primary antibodies, the streptavidin-biotin method was performed using the biotynylated secondary antibody together with streptavidin-alkaline phosphatase-conjugate (Zytomed Systems AP125, Zytomed, Berlin, Germany).
Filaggrin pattern was assessed as reported previously (11). Epidermal staining of CK16, CK17, IL-8, and MHC I was determined as established previously (12). CD1a-, CD4-, CD8-, IL-8-, IL-17-, IL-23-, MHC I- and MHC II- positive cells were semi-quantitatively evaluated by counting their number in 3 consecutive high-power fields, separately in the epidermis and/or dermis. Ki67+ basal layer cells per 10 mm length were counted under 100-fold magnification.
Deparaffinization, antigen retrieval, quenching and blocking were carried out as for IL-17. For antibody staining mouse anti-human Ki67 (1:1000 in blocking solution, Clone MIB-1, Dako) was used as primary antibody and goat-anti mouse Alexa 488 (1:1000 in blocking solution, BD Bioscience, Heidelberg, Germany) as secondary antibody. Next, a directly labelled anti-human CD8a-PE antibody (1:200, Biolegend, San Diego, CA, USA) was utilized. CD8 Ki67 double-positive cells were detected by confocal microscopy (Leica SP2, Wetzlar, Germany).
Statistical analyses were performed with IBM SPSS Statistics, Version 21 software. Descriptive analyses of the outcome variables include determination of their frequencies, location and dispersion parameters in the different groups. Group comparisons of outcome variables were performed with χ2 tests or Mann–Whitney U tests, depending on the characteristic scale. p-values were considered as follows: > 0.1 no significance, ≤ 0.1 tendency, ≤ 0.05 significance, ≤ 0.01 high significance, and ≤ 0.001 highest significance.
Isolated palmoplantar involvement with sharply demarcated erythrosquamous plaques was found in 76.7% of patients with EIP, 76.9% of patients with eczema, and 33.3% of patients with psoriasis.
All patients in the ACD and EIP cohort had one or more clinically relevant positive patch test reaction. In the psoriasis group, 55.6% of patients had weak-positive (+) patch tests with no clinical or histological correlation with contact hypersensitivity.
Serum from these patients had elevated levels of IgE (>100 kU/l) in 40% (2/5) of patients with psoriasis, 76.2% (16/21) of patients with EIP and 18.2% (2/11) of patients with ACD.
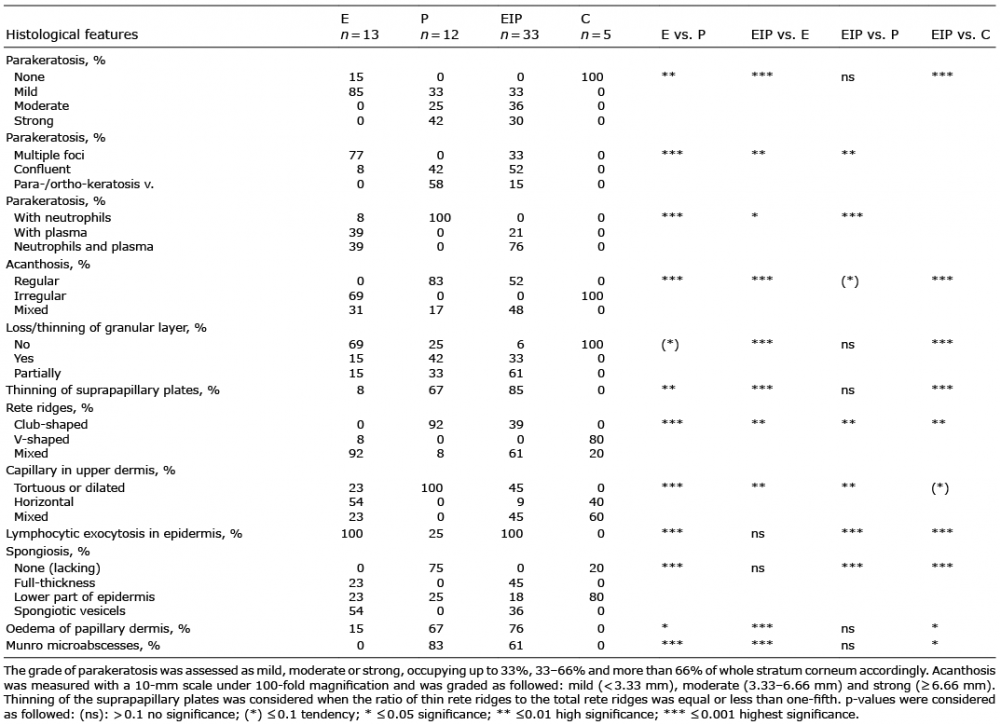
The frequency of different histological features in ACD, psoriasis, EIP and healthy skin is shown in Table I. EIP had overlapping characteristics with both psoriasis and ACD (Fig. S1d, e). The following features of EIP were shared with psoriasis: moderate-to-strong parakeratosis, regular acanthosis, loss of granular layer, thinning of suprapapillary plates, oedema of papillary dermis, and presence of Munro’s microabscesses. Similar to ACD, EIP was also characterized by lymphocytic exocytosis, full-thickness spongiosis, or formations of spongiotic vesicles. In addition, EIP showed a high coincidence of neutrophils and plasma exudation in parakeratosis, which was also observed in ACD, although to a lesser extent.
Table I. Histological features of contact dermatitis (E), psoriasis (P), eczema in psoriatico (EIP) and healthy skin (C)
CK17 staining was negative in the basal layer and positive in the upper epidermal layers of inflammatory diseases (Fig. 1a). Strong positive reactions were observed in EIP and psoriasis, in contrast to weak-positive staining in ACD (p ≤ 0.001 and p ≤ 0.05, respectively) and to a negative reaction in healthy controls (p ≤ 0.001) (Fig. 1b).
Fig. 1. Paraffin sections of skin samples from healthy controls (C), patients with contact dermatitis (E), psoriasis (P) and eczema in psoriatico (EIP) were stained with CK17, CK16, filaggrin and Ki67 antibodies. (a) CK17 staining reveals strong, positive reaction in upper epidermis in psoriasis and “eczema in psoriatico” (EIP) in contrast to a weak-positive expression in eczema and to a negative reaction in healthy controls. (b) Semi-quantitative evaluation of CK17 staining in superficial layers. (c) CK16 staining with diffuse positive reaction in suprabasal and superficial epidermis layers in eczema, psoriasis and EIP. (d) Statistical analysis of CK16 staining in superficial layers. (e) Filaggrin staining with normal pattern in healthy controls, linear pattern in eczema, chequered pattern in psoriasis and dotted pattern in EIP. (f) Semi-quantitative evaluation of filaggrin staining. (g) Ki67+ cells distributed predominantly in basal layer, are most abundant in psoriasis. (h) Statistical analysis of Ki67 staining in stratum basale. Staining × 200.
Diffuse positive expression of CK16 staining was observed in ACD, EIP and psoriasis (Fig. 1c), with no statistical differences between these cohorts (Fig. 1d). CK16 staining in healthy skin samples was negative, except in the acrosyringium.
Filaggrin expression was most reduced in EIP, followed by psoriasis and ACD (Fig. 1e). The distribution and statistical evaluation are shown in Fig. 1f.
Ki67+ cells were found predominantly in the basal layer and were most abundant in psoriasis (Fig. 1g). Ki67 staining revealed a moderately increased number of proliferating cells in EIP, which was lower than in psoriasis (p ≤ 0.05) and higher than in ACD (p ≤ 0.05) (Fig. 1h).
CD1a+ cells distributed throughout the epidermis (Fig. 2a), showed an increased number in ACD and EIP compared with psoriasis (p ≤ 0.01) and healthy skin (p ≤ 0.001) (Fig. 2b).
Fig. 2. Paraffin sections of skin samples from healthy controls (C), patients with contact dermatitis (E), psoriasis (P) and eczema in psoriatico (EIP) were immunohistochemically stained with CD1a, MHC I, MHC II. (a) CD1a staining with increased number of positive cells in contact dermatitis and EIP compared with psoriasis and healthy controls. (b) Semi-quantitative analysis of CD1a staining in epidermis. (c) MHC I staining with membrane-like pattern and pericellular delineation in the basal- and suprabasal epidermal layers, most pronounced in eczema and EIP compared with psoriasis and with healthy skin. (d) Statistical evaluation of MHC I expression in suprabasal layers. (e) MHC II staining with elevated count of positive epidermal cells in eczema and EIP compared with psoriasis and with healthy controls. (f) Semi-quantitative evaluation of MHC II staining in epidermis. Staining × 200
Evaluation of major histocompatibility complex (MHC I) within the suprabasal area revealed overexpression in both ACD and EIP compared with psoriasis and healthy skin (p ≤ 0.001) (Fig. 2c, d).
MHC II staining showed an increased number of positive epidermal cells in ACD and in EIP compared with psoriasis (p ≤ 0.01 and p ≤ 0.001, respectively) and healthy controls (p ≤ 0.001) (Fig. 2e, f).
IL-8 revealed an intracorneal staining that was strongest in psoriasis, moderate in EIP and lowest in ACD (Fig. 3a, b). IL-8 showed contemporarily a distinct, intercellular, spotted pattern in basal and suprabasal keratinocytes, which was most pronounced in ACD compared with psoriasis and EIP (p ≤ 0.01 and p ≤ 0.05, respectively) (Fig. 3c, d).
Fig. 3. Interleukins IL-8, IL-17, and Il-23 in paraffin sections obtained from healthy controls (C), patients with contact dermatitis (E), psoriasis (P) and eczema in psoriatico (EIP). (a) Accumulation of interleukin (IL)-8+ neutrophils in stratum corneum in psoriasis. (b) Semi-quantitative evaluation of IL-8 staining intracorneal. (c) Spotted pattern of IL-8 in basal- and suprabasal keratinocytes in eczema. (d) Statistical analysis of IL-8-spotted pattern suprabasal. (e) IL-17+ cells with a mast cell-like morphology in EIP. (f) Statistical evaluation of IL-17 staining. (g) IL-23+ cells with neutrophil morphology in EIP. (h) Semi-quantitative analysis of IL-23 staining dermal. Staining × 400.
IL-17+ cells were found in the dermis, showing mainly a mast cell-like morphology (Fig. 3e). Their counts were increased in both psoriasis and EIP compared with ACD (p ≤ 0.05 and p ≤ 0.1, respectively) and healthy skin (p ≤ 0.01) (Fig. 3f).
IL-23+ cells, predominantly with neutrophil morphology, were found in the papillary dermis of inflammatory diseases (Fig. 3g) and were not observed in healthy skin. Both psoriasis and EIP had an increased number of IL-23+ cells compared with ACD (p ≤ 0.01 and p ≤ 0.05, respectively) and healthy skin (p ≤ 0.001) (Fig. 3h).
Elevated IgE was found to correlate positively with the number of CD1a+ cells and negatively with mitotic activity. As a result, patients with EIP and elevated IgE levels had an eczematous reaction pattern in both stainings: an enhanced number of CD1a+ cells and reduced number of Ki67+ cells.
ACD and EIP had an increased number of both epidermal CD4+ and CD8+ T cells compared with psoriasis (p ≤ 0.001) and healthy skin (p ≤ 0.001) (Fig. 4a, b). Regarding the number of dermal CD4+ T cells, there were no statistical differences between the 3 diseases (Fig. 4c). Surprisingly, a greatly increased number of dermal CD8+ T cells was found in EIP, compared not only with healthy skin (p ≤ 0.001), but also with ACD (p ≤ 0.01) and psoriasis (p ≤ 0.001) (Fig. 4d, e). Double immunofluore-scence staining with CD8 and Ki67 in EIP samples proved mitotic activity of dermal CD8+ T cells (Fig. 4f).
Fig. 4. T cell subsets (CD4, CD8) in paraffin sections obtained from healthy controls (C) and patients with contact dermatitis (E), psoriasis (P) and eczema in psoriatico (EIP). (a) Statistical evaluation of epidermal CD4+ T cells. (b) Statistical analysis of epidermal CD8+ T cells. (c) Statistical evaluation of dermal CD4+ T cells. (d) Semi-quantitative analysis of CD8+ T cells in dermis. (e) Overexpression of CD8+ T cells in dermis of EIP. (f) Double immunofluorescence staining with CD8 and Ki67 in EIP (white arrows). (g) Summarized results of immunochemistry. Staining × 200.
Erythematous-squamous plaques on palms and soles often cause diagnostic difficulties. Positive history of psoriasis does not exclude the coexistence of contact dermatitis, atopy or irritation. ACD reactions in palmoplantar localisation are often chronic and due to the ubiquitous character of allergens not self-limited. Persistent ACD acts as a negative determinant of psoriasis (5). Allergy diagnostic including patch testing is essential for the correct diagnosis, successful treatment and, in our opinion, mandatory in cases of palmoplantar psoriasis. It can be speculated, that predisposed patients with psoriasis can develop ACD and subsequently manifestation of EIP. If its development is work-related and lead to aggravation of constitutional disease (here psoriasis), an occupational disease may be assessed (13). It should be further examined, if IgE elevation, which was frequently observed in EIP patients, contributes to the development of contact sensitization (14).
A literature review revealed a few studies comparing the histological features of non-pustular palmoplantar psoriasis with those of palmoplantar contact dermatitis (15, 16). EIP had features that overlapped with both of these conditions, similar to the histological pattern already described of an ACD reaction on top of pre-existing psoriasis (8). Although it was possible to distinguish some characteristic features, H&E staining alone was not always sufficient for the differential diagnosis of these diseases.
CK17 reactivity can be observed in the hyperproliferating epidermis of psoriasis, but not in healthy skin (17, 18), which correlates with our findings. A few studies have examined expression of CK17 in contact dermatitis (19), but to our knowledge there has been no comparison with psoriasis. In the current study, CK17 showed decreased expression in ACD compared with both psoriasis and EIP. Therefore CK17 and not CK16 (which is highly positive in all 3 examined conditions), appears to be useful in differentiation of epidermal alterations between palmoplantar psoriasis and ACD. EIP revealed a psoriasis-like reaction pattern of CK17, probably due to the same epidermal alterations.
Filaggrin is the main component of keratohyalin granules located in stratum granulosum. Its deficiency is associated with impaired skin barrier function (20). Reduced filaggrin expression may be a result of alterations in epidermal differentiation or of filaggrin-loss-of-function mutations, as described in psoriasis (11) and atopic dermatitis (21). In our study, EIP showed stronger reduced filaggrin expression compared not only with ACD, but also with psoriasis. It may be that, in EIP, loss of granular layer characteristic for psoriasis and coexistent contact sensitization, may negatively influence filaggrin production.
Hyperproliferation of epidermal keratinocytes detected by Ki67 staining (22) is a characteristic feature of psoriasis. Only a few studies have examined the proliferation rate in contact dermatitis (23) and only single comparisons have been made between psoriasis and eczema (8, 24). As expected, psoriasis had a higher proliferation rate than ACD. In our study, EIP showed more similarity in hyperproliferation to psoriasis, especially when evaluating cases with normal IgE.
CD1a is a specific marker for Langerhans cells (LCs), a subtype of epidermal dendritic cells (DCs) (25). LCs are antigen-presenting cells, which are important for the development of ACD (26). The role of LCs in psoriasis is not completely understood, and their number varies in the different stages and localizations (27). DCs also play an important role in atopic dermatitis, and their number correlates with disease activity (28). Our results confirm that LCs are highly increased in ACD compared with in healthy skin. The number of CD1a+ cells in psoriasis was significantly lower than in ACD and EIP, which depends on their localization (lesional skin) and impaired migratory functions of LCs in psoriasis (29, 30). EIP shared more similarities in the CD1a pattern with ACD than with psoriasis. Evaluation of patients with EIP having normal IgE levels in serum, however, had opposite results, confirming its psoriatic reaction pattern.
MHC class I molecules are expressed on the surface of all nucleated cells and take part in the presentation of endogenous peptide antigens to CD8+ T cells (31). In contrast to previous reports (32), we observed significant overexpression in ACD and EIP compared with psoriasis and healthy skin in the suprabasal epidermis only. Enhanced expression of MHC I molecules in ACD and EIP correlated with an elevated number of LCs and epidermal CD8+ T cells in both diseases.
MHC class II molecules are expressed on antigen-presenting cells and present exogenous antigenic peptides to CD4+ T cells (33). Increased expression of MHC II in the epidermis of ACD and EIP correlated with elevated numbers of epidermal CD4+ cells, as well as LCs in both of these diseases.
IL-8 is a marker of different inflammatory processes (33), which plays a role in the chemotaxis of neutrophils and T lymphocytes into the lesional epidermis. Our results regarding IL-8 staining in psoriasis were consistent with previous reports (34). Due to a higher number of accumulated neutrophils in parakeratosis, psoriasis had a stronger intracorneal expression of IL-8 than did ACD. Spotted, keratinocyte-derived IL-8 pattern in the lower epidermis was strongest in ACD. EIP revealed distinct characteristics of IL-8 staining with a weakly spotted pattern (like that of psoriasis) and a moderate number of intracorneal neutrophils.
Il-17 as a proinflammatory cytokine induces production of IL-6 and IL-8, which are involved in recruiting DCs, Th17 cells and neutrophils. In agreement with our observations, it has been shown that mast cells are the majority of IL-17-containing cells in psoriatic skin (35). mRNA expression of IL-17A and IL-17F was found to be enhanced in lesional psoriatic skin, compared with non-lesional psoriatic skin (33–39). IL-17+ T cells were also found within spongiotic areas in ACD and were shown to amplify allergic reactions (40). We found an increased number of IL-17+ cells in psoriasis compared with ACD, as reported previously (8). EIP revealed a psoriasiform reaction pattern.
IL-23 promotes the development and activation of Th17 cells and plays a crucial role in the pathomechanism of psoriasis (41, 42). Some studies have described an increased number of IL-23 cells in lesional psoriatic skin (43), but this has not been compared with ACD. As expected, the highest number of IL-23+ cells were observed in psoriasis and the lowest in ACD. EIP showed similarities with psoriasis.
T lymphocytes play a crucial role in the pathogenesis of psoriasis and contact dermatitis. In both disorders, they are polarized as Th1 and Th17. Successful therapies have been found to reduce their overall number (30). Both ACD and EIP showed an increased number of epidermal CD4+ and CD8+ T cells compared with psoriasis, due to lymphocytic exocytosis. As reported previously (44), and as was confirmed in the current study, there were more dermal CD8+ T cells in ACD than in psoriasis. Surprisingly, the number of dermal CD8+ T cells in EIP outnumbered not only those found in psoriasis, but also in ACD. Double immunohistochemical staining (CD8+Ki67+) performed in EIP revealed proliferate activity of dermal CD8+ T cells within the dermal lymphoid infiltrate, similar to earlier studies of spongiotic dermatitis (44). The authors speculated that DCs could stimulate adjacent CD8+ T cells directly or via CD4+ T cells. Additional studies on this T-lymphocyte subset are required to further explore its role in the pathomechanism of EIP.
Studies of molecular and cellular profiling of psoriasis and eczema have provided new insights into these complex and multifactorial diseases. Various approaches, such as analysis of gene expression profiles from skin biopsy tissues, disease-associated serum cytokines by reverse transcription PCR, or immune cell infiltration, have been suggested (45–47). It can be assumed that molecular diagnostics can distinguish between common psoriasis and ACD transcriptomes. However, it has been suggested recently (45) that various clinical forms of psoriasis have different molecular profiles. Comparison of thin and thick plaque psoriasis has revealed differences in the immunohistological pattern as well as in the expression levels of the psoriasis transcriptome (45). Distinctions between mild and severe psoriasis were drawn by differences in expression of some regulatory genes (46). Examination of the cellular and molecular phenotype of scalp psoriasis revealed diversities compared with skin psoriasis (48). Molecular profiling of contact dermatitis skin biopsies also revealed heterogeneities and provided evidence for allergen-dependent differences in immune response (47). Although various allergens lead to similar clinical manifestations, they were characterized by distinct immune polarization (47). Further research is needed into molecular phenotyping of palmoplantar psoriasis and palmoplantar contact dermatitis, taking into account allergen-dependent differences.
This study provides new insight into the clinical, histological and immunohistological differentiation of palmoplantar psoriasis and chronic palmoplantar ACD, and, in particular, EIP, a condition composed of features of both. We can therefore distinguish a distinct clinical entity: EIP with type IV sensitization and overlapping clinical and histological features of both psoriasis and ACD. Immunohistological analysis showed that, in the case of EIP, a small set of markers specific for both diseases is found contemporaneously (Fig. 4g). These results enable better understanding of the pathomechanism and differentiation between EIP, psoriasis and ACD in the palmoplantar localization. This data is also of importance when a relevant occupational background is present in patients with psoriasis.
The authors would like to thank Ines Doering for excellent technical assistance.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize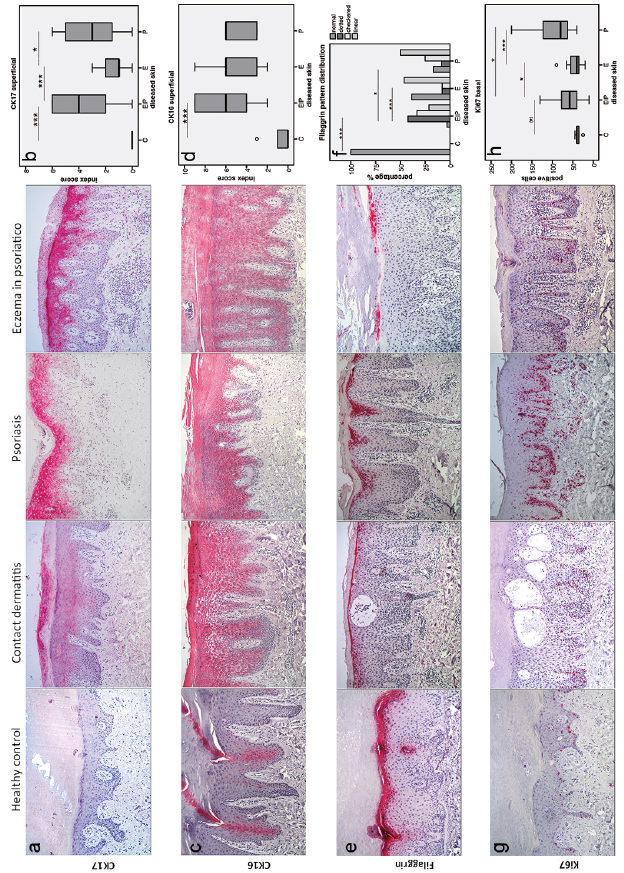 Click to show fullsize
Click to show fullsize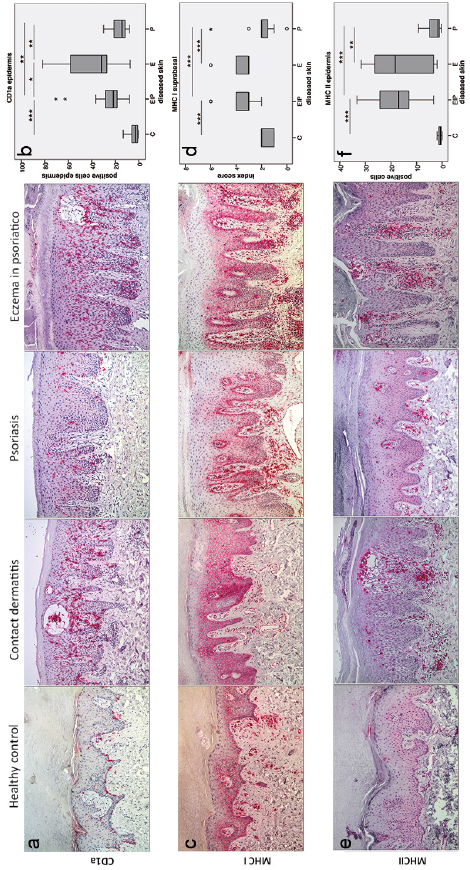 Click to show fullsize
Click to show fullsize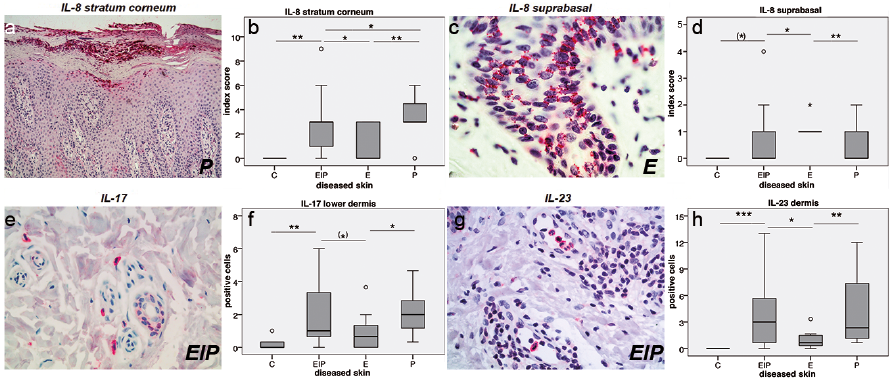 Click to show fullsize
Click to show fullsize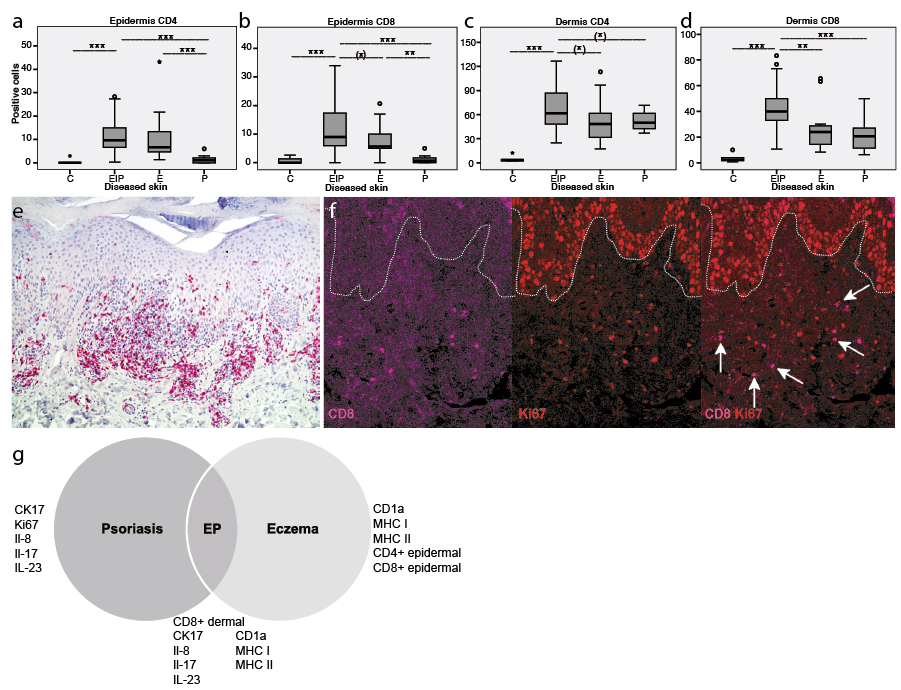 Click to show fullsize
Click to show fullsize