


1Department of Dermatology and Allergy, Charité – Universitätsmedizin Berlin, Berlin, Germany, and 2LEO Pharma A/S, Ballerup, Denmark
Substance P (SP) and its receptor neurokinin 1 (NK1R) are thought to be involved in the pathogenesis of
chronic prurigo. Here, we assessed SP serum levels, cutaneous NK1R expression, and the effects of topical aprepitant, an NK1R antagonist, in patients with chronic prurigo. SP and NK1R were increased, compared with controls, in the serum and in lesional vs. non-lesional skin of the patients, respectively. Aprepitant, in a randomized, placebo-controlled, split-sided, double-blind trial, reduced the intensity of pruritus as assessed by visual analogue scale by > 50% from base-line to day 28 (–35.2), but so did placebo vehicle (–38.1, p = 0.76). Overall clinical scores improved significantly by day 28 in both treatment groups, with no significant difference between the 2 groups (p = 0.32). Our findings imply that both SP and NK1R are involved in the pathogenesis of chronic prurigo. Parallel group-designed trials are needed to assess the efficacy of topical aprepitant treatment in this condition.
Key words: prurigo; aprepitant; substance P; NK1R; lesional skin; pruritus intensity.
Accepted Aug 29, 2017; Epub ahead of print Aug 30, 2017
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Martin Metz, Department of Dermatology and Allergy, Charité – Universitätsmedizin Berlin, Charitéplatz 1, DE-10117 Berlin, Germany. E-mail: martin.metz@charite.de
Chronic prurigo (CPG) is a debilitating disease characterized by pruritus with chronic and persistent lesions, papules and/or hyperkeratotic nodules (1). Pruritus is so severe that patients cannot suppress the urge to scratch, creating secondary scratch lesions, often with deep excoriations. The underlying pathophysiological mechanisms of CPG are unknown. In many patients, the condition is a symptom of a specific disease, including dermatological conditions with inflamed skin (e.g. atopic dermatitis) (2), or diseases unrelated to the skin (e.g. chronic kidney failure or neurological diseases) (1). Sometimes no underlying disease can be detected and a multifactorial origin is assumed (3).
Effective treatment of CPG is difficult and, in most patients, symptom resolution is not achieved. Common treatment regimens include topical therapies with emollients and glucocorticosteroids in the case of inflamed skin, and systemic treatments. Most systemic treatments, however, do not achieve sufficient symptom control (e.g. antihistamines) or are associated with unacceptable side-effects (e.g. opioid-receptor antagonists, glucocorticosteroids, anticonvulsants or anti-depressants), and none are licensed for the treatment of CPG (4). In addition, because CPG is often a comorbidity of another condition, patients can already be taking medications that are contraindicated with current systemic treatments. Hence, the need for a targeted and effective topical treatment is high (5).
Patients with chronic pruritus have been reported to show elevated expression of neurokinin 1 receptor (NK1R) on their keratinocytes (6). Substance P (SP), the main ligand for NK1R, has been strongly implicated in the mechanism of chronic pruritus (7, 8). SP levels are upregulated in chronic urticaria, one of the itchiest diseases known (9) and SP stimulates dermal mast cell degranulation (10). The main source of the increased SP, i.e. from the central or peripheral nervous system, is unknown. Patients with nodular prurigo, but neither healthy controls nor patients with lichen simplex, have been shown to have an increased density of SP-positive skin nerve fibres (11), indicating that SP released from sensory nerves in the skin may be the relevant factor in CPG. Ständer et al. (12) were the first to report the therapeutic potential of aprepitant, an NK1R antagonist, in the treatment of CPG. They demonstrated that oral aprepitant significantly reduced the intensity of pruritus in patients with chronic pruritus, especially in those with CPG, by systemically inhibiting NK1R (12, 13). Whether the observed effects were due to action on NK1R in the central nervous system (CNS) or in the periphery, however, is unknown. Evidence exists for a role of cutaneous SP in the pathogenesis of other dermatological conditions, such as psoriasis (14). A 1% aprepitant topical formulation has been shown to be effective in blocking NK1R-mediated effects in gerbils (15). However, a topical preparation of aprepitant has failed to modulate allergic type I and type IV reactions in patients and healthy individuals and to ameliorate itch in patients with chronic pruritus (16, 17). It is unclear whether the lack of efficacy in these investigations was due to insufficient epidermal penetration, or to the lack of a role for peripheral NK1R-SP interactions in pruritus.
The prospect of combining a potentially specific anti-pruritic treatment with a supporting topical treatment that would penetrate into the dermis prompted this study of SP and NK1R expression in patients with CPG and this current randomized, placebo-controlled trial. The primary aims were to assess SP levels in the serum and NK1R levels in the skin of CPG patients, and to compare the efficacy of topical aprepitant 1% gel applied over a 28-day period in patients with CPG with therapy-refractory chronic pruritus, compared with that of placebo vehicle.
A group of 46 individuals, consisting of 26 CPG patients and 20 healthy individuals, was assessed for serum levels of SP. These individuals all gave informed consent for blood samples to be taken and used for research purposes. Nineteen patients with CPG were assessed for cutaneous NK1R expression and were included in the clinical trial. These patients had CPG with symmetrical prurigo lesions at upper or lower extremities for over 6 months and therapy-resistant pruritus with a visual analogue scale (VAS, 0–10) of 6 or higher 2 days before Visit 1. Patients needed to be refractory to at least 2 previous antipruritic treatments with topical, intra-lesional or systemic corticosteroids or other immunosuppressants, antihistamines, antipsychotics, antidepressants, anticonvulsants and/or ultraviolet (UV) irradiation. Key exclusion criteria included concomitant medications that are primarily metabolized through cytochrome P450 3A4, use of topical antihistamines, UV irradiation treatment less than 6 weeks before Visit 1, corticosteroids or mast cell stabilizers on the skin less than 3 weeks prior to Visit 1 or during the course of the trial.
SP serum levels were measured by enzyme-linked immunoassay (ELISA) (R&D Systems, Minneapolis, MN, USA) analysis according to the manufacturer’s instructions. Expression of NK1R was assessed by immunohistochemistry of biopsies from lesional and non-lesional skin. Paraffin-embedded skin sections were stained with a polyclonal rabbit antibody against the second extracellular domain of human NK1R (LSBio, Seattle, WA, USA) and blind counted by an investigator (MaMe). Sections were counted at 400× magnification in 3 microscopic fields, to assess the number of NK1R-positive cells. Staining intensity was assessed by measuring expression of NK1R in the epidermis at 100× magnification.
This was a German single-centre, prospective, randomized, placebo-controlled, double-blind, left/right split-side comparison, phase IIa, trial to evaluate the effects of topical aprepitant in 19 patients with therapy-refractory CPG. The trial was initiated in September 2013 and was completed in May 2014. It was conducted in accordance with the Declaration of Helsinki with signed informed consent obtained from all patients. The trial consisted of 5 visits including Visit 1/Screening (Day –14 to –7), Visit 2 (Day 1), Visit 3 (Day 14 ± 2 days), Visit 4 (Day 28 ± 2 days) and Visit 5 (Day 42 ± 3 days). Treatment assignment concerning the right or left extremity was pre-planned according to a computer-generated randomization schedule in which the patient was assigned the next (ascending) randomization code number available at the trial site. Patients and investigators remained unaware of individual treatment assignment during the conduct of this trial; packaging and labelling contained no evidence of the product identity, and treatment could not be differentiated by smell or colour. Randomized patients received the investigational product (aprepitant gel (10 mg/g gel)) on one side of the body and placebo vehicle (gel) on the other side, applied twice daily. The patients had to return the (empty) containers at every visit to ensure compliance. In addition, 10 patients gave consent for obtaining biopsies, which were then collected from lesional and non-lesional skin prior to treatment, and from lesional skin after 28 days of treatment. Patients were randomized on Day 1 to receive treatment with topically applied 1% aprepitant gel on selected treatment areas on one upper/lower extremity and placebo vehicle on the other upper/lower extremity.
The applied gel and gel vehicle comprised diethylene glycol monoethyl ether (Transcutol® P; Gattefossé, saint-Priest, France), propylene glycol (Lyondell Chem. Comp., Huston, TX, USA), glycerol 85% (AarhusKarlshamn, Malmö, Sweden), and hydroxypropylcellulose (Klucel™ LF Pharm; Ashland Specialty Ingredients G.P., Wilmington, DE, USA) in which aprepitant (Glenmark Generics Ltd, Watford, UK) was dissolved.
The skin penetration of aprepitant in the gel formulation was assessed in vitro in pig ear skin in flow-through (1.9 ml/h) diffusion cells (PermeGear®, n = 6). The receptor fluid (acceptor) was 0.04 M isotonic phosphate buffer pH 7.4 containing 4% (W/V) bovine serum albumin, fraction V. The formulation was applied at 6 mg/cm2 and the skin concentration (epidermis and dermis, after removal of stratum corneum) was measured 21 h after application. The skin concentration was 35 ± 33 µM (mean ± standard deviation (SD)) corresponding to approximately 5% of the given dose.
The primary objective was to demonstrate the efficacy of topical 1% aprepitant gel applied twice daily on pruritus in patients with CPG, compared with placebo vehicle after 28 days of treatment. Exploratory analyses included assessments of the condition of the skin after 28 days of treatment using the Patient Global Assessment (PGA) and clinical score, the long-term effect of treatment after a follow-up period of 14 days, and safety assessments. At Visits 2, 3, 4 and 5, the clinical score of each treated area was assessed by the investigator using a score of 0 (non-existent) to 3 (severe) based on erythema, crusts, scratch artefacts and infiltration. Skin biopsies from lesional and non-lesional skin of patients were taken to assess the expression of NK1R protein and the number of NK1R-expressing cells in the dermis by immunohistochemistry (10). Pruritus intensity of each treated area was scored by patients at each visit using the VAS, ranging from 0 (no pruritus at all) to 100 (worst pruritus imaginable).
Safety was evaluated by reporting of adverse events (AE), assessing vital signs and laboratory assessments.
All randomized subjects with at least one application of the study drug were included in the full analysis set used in efficacy analyses. The safety analysis set included all subjects with at least one application of the study drug. This population was used for all safety analyses and baseline characteristics. Missing values were not imputed. All statistical tests were 2-sided with a significance level of 5%; 2-sided 95% confidence intervals (CI) were calculated if applicable. All data obtained in this trial were analysed with descriptive statistics by treatment group.
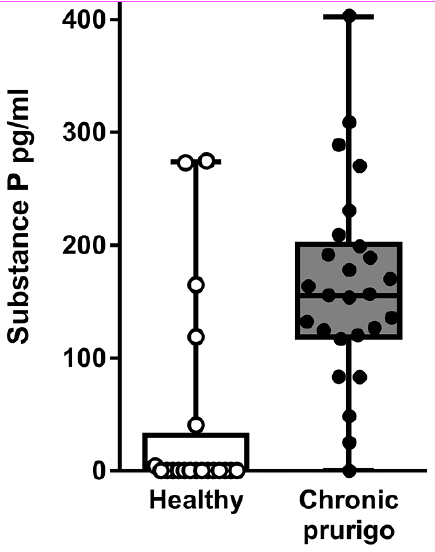
Assessment of patients with CPG (n = 26) and healthy individuals (n = 20) showed that serum SP levels were markedly increased in patients with CPG vs. healthy individuals (163.5 ± 17.3 vs. 43.7 ± 20.1; p < 0.001, Fig. 1). Demographics between these 2 groups were well matched: median age (IQR) was 69 (63–78) and 65 (60–74) years, proportion of males was 13 (50%) and 10 (50%), for CPG patients and healthy individuals, respectively. Mean itch intensity (VAS (SD)) in patients with CPG was 6.7 (2.7).
Fig. 1. Substance P is elevated in the serum of patients with chronic prurigo compared with healthy individuals. Substance P was measured by enzyme-linked immunosorbent assay (ELISA) in the serum of patients with chronic prurigo (n = 26), and age- and sex-matched healthy controls (n = 20). Boxes represent 25th and 75th percentiles, horizontal lines the median and whiskers show minimum to maximum values with the dots representing individual subjects, ***p < 0.001 (unpaired t-test).
NK1R expression in the lesional skin of CPG patients was significantly higher than in non-lesional skin as assessed by immunohistochemistry. Both the number of NK1R-positive cells in the dermis (Fig. 2A) and the intensity of NK1R immunoreactivity in the epidermis (Fig. 2B) were found to be notably increased in lesional compared with non-lesional skin (p < 0.05). Fig. 2 C–F shows representative stainings of NK1R in lesional (Fig. 2C, E) and non-lesional (Fig. 2D, F) skin in 2 individual patients.
Fig. 2. Neurokinin 1 receptor expression is increased in lesional skin of patients with chronic prurigo. (A and B) Paraffin-embedded skin sections were stained with a polyclonal rabbit antibody against the 2nd extracellular domain of human neurokinin 1 receptor and blind counted by an investigator. Sections were evaluated at 100× magnification and staining intensity was rated between 0 and +++. Boxes represent 25th and 75th percentiles, horizontal lines the median and whiskers show minimum to maximum values with the dots representing individual sections, *p < 0.05 (paired t-test). (C–F). Examples at 100× magnification of samples from 2 individual patients. (C and E) Lesional skin, (D and F) non-lesional skin.
In this clinical trial, 23 patients were screened and 19 of these patients fulfilled the eligibility criteria and completed the trial. A summary of patient demographics for this study population is provided in Table I.
Table I. Patient demographics
By the end of the 28-day treatment period, mean ± standard error of the mean (SEM) of VAS score for pruritus intensity had decreased in both groups, –35.2 ± 6.0 (66.1 ± 8.2%) in the aprepitant group vs. –38.1 ± 6.8 (58.0 ± 9.4%) in the placebo vehicle group, with no significant difference between the 2 treatment groups (p = 0.76). Fig. 3A shows the reduction in pruritus after 28 days of treatment from baseline and Fig. 3B shows the reduction in pruritus over time, which continued to decrease to Day 28.
Fig. 3. Topical application of both aprepitant and placebo resulted in reduction in pruritus intensity and improvement in clinical scores in patients with chronic prurigo. Topical aprepitant 1% on 1 extremity, and placebo on the other was applied twice daily for 28 days and pruritus intensity on each arm was assessed by patients using a visual analogue scale, ranging from 0 (no pruritus at all) to 100 (maximum pruritus imaginable). (A) Pruritus reduction from baseline to the end of the application period after 28 days. (B) Pruritus intensity over time. (C) Clinical prurigo score is a 4-point score ranging from 0–3, assessed by an investigator using the mean from a score of 0 (non-existent) to 3 (severe) for erythema, crusts, scratch artefacts and infiltration. (A, B) Data is presented as mean ± standard error of the mean (SEM). (C) Boxes represent 25th and 75th percentiles, horizontal lines represent the median and whiskers show minimum to maximum values; *p < 0.05, ***p <0.001, n.s. = not significant, using (A) unpaired t-test, (B) 2-way analysis of variance (ANOVA), and (C) paired t-test.
The prurigo lesions within the treated skin areas were scored by clinical prurigo score based on the presence and extent of erythema, crusts, scratch artefacts and infiltration before and after 28 days of treatment. The overall CPG scores at the end of the 28-day treatment period were significantly improved in both treatment groups (aprepitant (mean ± SEM): from 1.6 ± 0.2 to 1.0, p = 0.0007); placebo (mean ± SEM): from 1.6 ± 0.2 to 1.3 ± 0.2, p = 0.03), with no significant difference between the 2 groups (p = 0.32, Fig. 3C). Within the subcategories, the extent§ of skin infiltration did not change in either group, and intensity of erythema improved significantly in both groups (p = 0.015 for placebo vehicle, p = 0.008 for aprepitant) from baseline to end of treatment (Table II). In the rating of scratch artefacts and crusting, only aprepitant-treated skin showed significant improvement (p < 0.05 and p < 0.01, respectively), while placebo-treated skin did not show an improvement (p = 0.134 and p = 0.129, respectively). None of the subcategories showed a significantly different improvement between placebo vehicle and aprepitant (data not shown).
Table II. Baseline characteristics of the treatment areas
Overall, 17 patients (89%) experienced an AE during this trial. In the aprepitant arm, 14 (70%) were considered to be possibly related to the treatment vs. 11 (55%) in the placebo vehicle group (p = 0.8, Fisher exact test). The most common AEs were pain at the site of administration (55% vs. 40%) and cutaneous reactions (75% vs. 55%) such as irritation in aprepitant vs. placebo vehicle groups, respectively. Overall, 17 AEs (85%) were mild and 3 (15%) were moderate. No serious AEs occurred during treatment in either group.
High levels of SP were found in patients with prurigo compared with healthy individuals. This could: (i) have central effects on NK1R expressed in the CNS; and/or (ii) have peripheral effects on NK1R expressed in the skin. In support of the latter, we identified a strongly increased NK1R immunoreactivity in the epidermis and an increase in the number of NK1R-expressing cells within the dermis of lesional vs. non-lesional skin. These findings raise the possibility that expression of NK1R in the periphery might be involved in the pathogenesis of CPG and that a topical approach to blocking NK1R activity in the skin could be beneficial for patients with CPG. The role and relevance of this increase in NK1R expression is, as yet, unknown. The increase in NK1R-expressing cells in the dermis as well as the enhanced expression of NK1R in epidermal keratinocytes could be responsible for a higher responsiveness to SP, and consequently, could cause release of more pruritogens from lymphocytes, mast cells or other NK1R-expressing cells in the dermis, as well as from keratinocytes. Despite the strong immunoreactivity of NK1R in the epidermis, NK1R appears not to be involved in the regulation of the epithelial barrier function as transepidermal water loss, which is increased in the case of damage to the skin barrier, was similar in lesional vs. non-lesional skin, and was not significantly different between lesional skin treated with aprepitant or placebo vehicle (data not shown).
Our findings of high serum levels of SP and lesional skin levels of NK1R prompted us to perform the first randomized controlled clinical trial to specifically investigate the efficacy of topical aprepitant 1% gel (10 mg/g) in patients with CPG. The primary objective of this clinical trial was not met. Treatment with topical aprepitant 1% gel did not result in a significantly more effective treatment for pruritus vs. placebo vehicle. Previous trials have shown efficacy with oral aprepitant, but its topical effect has not been proven. Overall, the efficacy between aprepitant gel and the placebo gel vehicle was not statistically significant, as both groups showed a large improvement in pruritus intensity, with over 50% reduction, as measured by VAS. The aprepitant gel was well tolerated overall with pain and irritation at the site of administration being the most commonly experienced AE. No unexpected AEs and no serious AEs were experienced by any patient.
A potential explanation as to why the efficacy in both treatment groups was high, with a much higher-than-expected result in the placebo vehicle group, could be a systemic effect of aprepitant due to its ability to effectively penetrate the skin and enter the systemic circulation. To our knowledge, no pharmacokinetic data after the topical application of aprepitant have been previously published; however, permeation coefficient data from 1 clinical study have shown moderate permeation through the skin (16). Based on data from our in vitro diffusion study in pig ear skin, the bioavailability of aprepitant is estimated to be between 1% and 10%. Assuming a maximum absorption of 10%, the total amount of aprepitant absorbed would be 3 mg per day, i.e. less than 3% of the usually applied systemic dose (12, 18), a level which is likely to be too low to have any systemic effects. Analyses of blood samples during this trial confirmed that aprepitant was absorbed into the blood; however, the levels were found to be in a range of 30–3,000 pg/ml and did not correlate with the pruritus VAS scores (data not shown).
Another explanation for the similarity in results between aprepitant and placebo vehicle is that for NK1R to be effective, it must act on the CNS and cannot confer full efficacy in the periphery. The reduction in pruritus intensity could, in this case, be due to the gel vehicle and improved patient compliance. We believe that this is unlikely, as the observed effect of > 50% reduction is more than would be expected (19–21) and these patients had been treated for many years with most using regular emollients for long periods of time. There is also the possibility that SP drives CPG morbidity by acting on receptors other than NK1R (22). It has to be noted, how-ever, that SP is unlikely to be the only driver of CPG morbidity and that other mediators may also be involved.
We propose that the most likely reason for the similarities observed between aprepitant and placebo vehicle groups is due to the trial design and an inherent problem with the left-hand-side vs. right-hand-side design. It is highly possible that improvement of pruritus in one arm or leg resulted in the perception of an overall reduction in pruritus intensity by the patient, as has been shown in itch relief through “mirror scratching” trials (23). The significant differences observed in scratch artefacts and crusting in aprepitant-treated, but not in placebo-treated, skin further supports this hypothesis. In order to address this issue, a further, larger scale, placebo-controlled, parallel-group designed clinical trial with a topical NK1R agonist is warranted, ideally splitting patients into treatment group and placebo group so that any benefits experienced cannot be misinterpreted by the patient as an overall perception in decreased itch intensity.
This work was funded in part by I2DEAL, MaMe was supported by the Else Kröner-Fresenius-Stiftung. The authors would like to thank Gillian Brodie for editorial support in preparing this manuscript.
Conflicts of interest: SE, GH and WK are all employees of LEO Pharma.


 Click to show fullsize
Click to show fullsize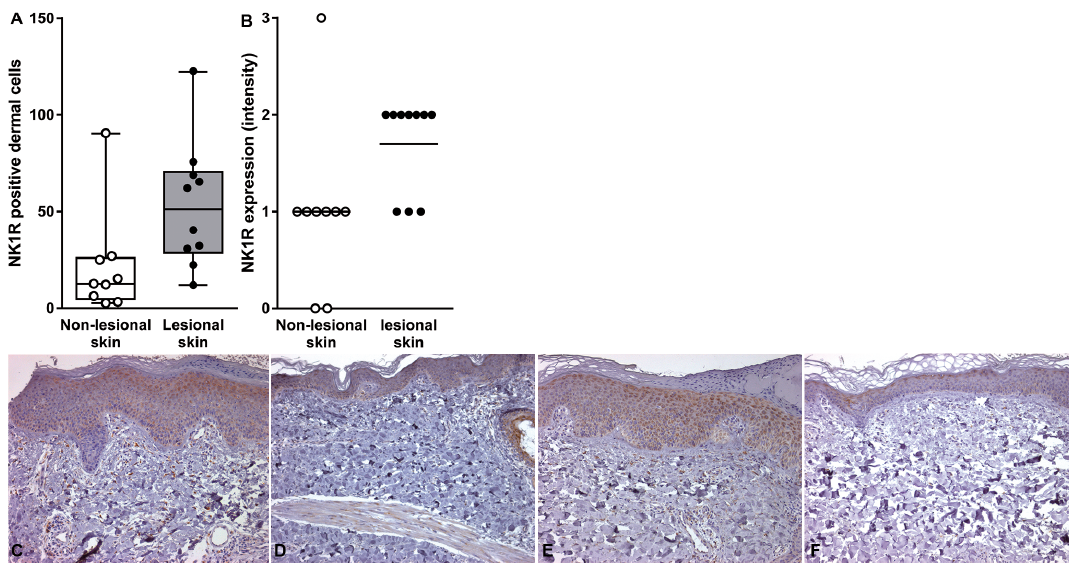 Click to show fullsize
Click to show fullsize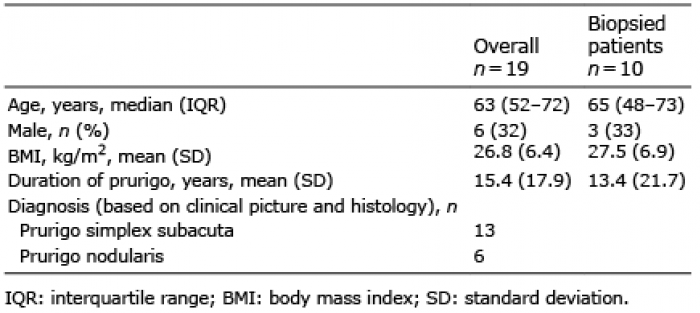 Click to show fullsize
Click to show fullsize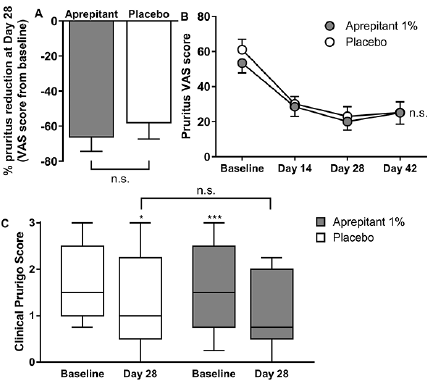 Click to show fullsize
Click to show fullsize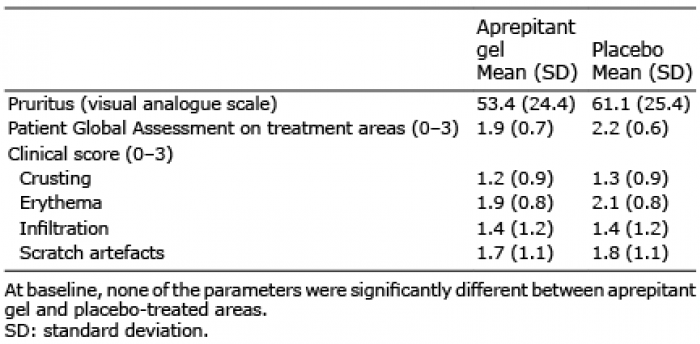 Click to show fullsize
Click to show fullsize