


1Department of Dermatology, St. George Hospital, 2Department of Anatomical Pathology, SEALS, 3Department of Plastic Surgery, St George Hospital, and 4University of New South Wales, Sydney, NSW, Australia
We investigate the epidemiology and outcomes of squamous cell carcinoma (SCC) in recessive dystrophic epidermolysis bullosa (RDEB) from the Australasian EB registry cohort. Seventeen out of 49 (34.6%) RDEB patients developed at least one SCC. Data detailing SCC was obtainable from 16/17 RDEB-SCC patients. A total number of 161 primary SCCs occurred in 16 RDEB-SCC patients with a mean of 10 SCCs per person. The earliest age of first SCC development was 16 years. Eleven out of 16 RDEB-SCC patients eventually developed metastatic SCCs. The majority of the tumours were well and moderately differentiated. The cumulative risk of SCC development by age 35 was 76.1% for RDEB-Generalized Severe (RDEB-GS) and 10% for RDEB-Generalized Intermediate (RDEB-GI). Amongst those who developed SCCs, their median time to death after first SCC was 5 years for RDEB-GI and 4 years for RDEB-GS. This is the first retrospective study of RDEB-SCC in Australasia.
Key words: recessive dystrophic epidermolysis bullosa; squamous cell carcinoma; epidemiology; prognosis.
Accepted Aug 29, 2017; Epub ahead of print Aug 30, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Prof. Dedee F. Murrell, MA, BM, FAAD, MD, FACD FRCP (Edin), Head, Department of Dermatology, St George Hospital, Gray St, Kogarah, Sydney, NSW 2217, Australia. E-mail: d.murrell@unsw.edu.au
Epidermolysis bullosa (EB), first described in 1886 (1), is a group of rare heterogeneous genodermatoses defined by mechanical fragility, blistering of mucocutaneous membranes, and compromised wound healing (2, 3). The prevalence of EB in Australia according to the Australasian EB registry (AEBR) is approximately 10.3 per million (4). Depending on the skin cleavage plain, EB is classified into 4 major types, i.e. EB simplex (EBS), junctional EB (JEB), dystrophic EB (DEB), and Kindler syndrome. DEB is broadly divided into dominant DEB (DDEB) and recessive DEB (RDEB) (2). Genetic mutations of the COL7A1 gene in DEB result in reduced or absent expression of type VII collagen, which is the main anchoring fibril that attaches the basement membrane of the epidermis to the dermis. RDEB can be further sub-divided into generalized severe (RDEB-GS), generalized intermediate (RDEB-GI). Rare variants of RDEB include RDEB inversa (RDEB-I), RDEB localized (RDEB-loc), RDEB pretibial (RDEB-pt), RDEB pruriginosa (RDEB-pr), RDEB centripetalis (RDEB-ce) and RDEB bullous dermolysis of the newborn (RDEB-BDN) (2).
Squamous cell carcinoma (SCC) is the most dreaded complication of EB. Detailed knowledge of its underlying pathogenesis is still unknown (5). Traditionally, the repetitive cycle of tissue damage and repair was thought to cause deterioration of cellular differentiation and buildup of carcinogenic mutations (6, 7). Some have proposed reduced activity of natural killer cells, up-regulation of basic fibroblast growth factor, and p53 gene mutations as potential contributors to the pathogenesis (8–10). The latest research showed that RDEB fibroblast gene expression is distinct from that of a non-RDEB fibroblasts, potentiating SCC adhesion, invasion, and growth (11). The role of collagen VII in EB tumorigenesis was also explored. In a mouse-model study of RDEB, no tumours were detected in mice without collagen VII expression whereas those expressing the amino-terminal non-collagenous NC1 domain of collagen VII were tumorigenic (12). The study demonstrated that collagen VII is a pre-requisite for epidermal tumourigenesis and NC1 domain of collagen VII promoted tumour cell invasion. However, another similar study by Pourreyron and colleagues (13) found that two out of 11 RDEB patients developed SCC without detectable levels of collagen VII collagen. The study concluded that individuals with RDEB can develop SCC regardless of type VII collagen expression. Recent studies have suggested that wound colonization with flagellated bacteria is a promotor for SCC in RDEB (14).
Unlike the pathogenesis, the epidemiology of EB is better understood with multiple case reports and case series on SCC development in EB (15–21). However, the data is limited to certain regions or states, rather than capturing all the cases within nations. The largest epidemiological study on the prevalence of SCC in EB is from the National EB Registry (NEBR) of the United States, amassing 3,280 patients with different EB subtypes (22). This study enhanced our understanding of SCC characteristics in EB including the common SCC occurrence sites, risk of SCC development, cumulative risk of death from metastatic disease, and therapeutic interventions for SCCs. A recent systematic review gathering 117 EB-SCC cases highlighted that the most frequently published cases of SCC were from RDEB patients with no sex predilection in accordance with the NEBR data (23). In contrast to the NEBR findings, however, this review found a higher incidence of SCC in Caucasians compared to other ethnic groups including Asians, Northern Africans and Hispanics. Having said that, 35.9% of the cases failed to report ethnic background of the patients in this systemic review. Reporting bias from large, established EB centers should also be considered when interpreting this data.
Australia is one of the countries where the incidence of cutaneous SCC is the highest. This is the first retrospective observational study on SCC in the Australasian EB Registry (AEBR). The aim of this study was to analyze the epidemiology and characteristics of RDEB-SCC in Australasia and to compare the findings with RDEB-SCC data from other countries.
Data was collected from February 2009 to September 2016. The study received ethical approval from the South Eastern Sydney Local Health District Human Research Ethics Committee (approved on 5 July 2012. HREC Ref: 10/108).
All of the patients in the AEBR had a diagnosis of EB confirmed through clinical assessment by EB dermatologists and/or confirmed through immunofluorescence mapping, electron microscopy, and/or gene mutation analysis. The diagnoses of RDEB-GS and RDEB-GI were made based on combination of clinical findings, collagen VII expression, and mutation analysis. Data on all RDEB patients in the AEBR was collected for this study. For those RDEB patients who developed at least one biopsy-proven SCC, we contacted all the relevant hospitals and clinics within Australia and New Zealand to access medical records.
Based on the data extracted from the AEBR database and additional data gathered, each patient’s summary on their clinical progress, pathological characteristic and treatment was generated.
Biostatistical analyses were performed using SAS OnDemand 3.5 statistical software (SAS Institute Inc., Cary, NC, USA). Risk of SCC development and SCC-related death was analyzed using survival analysis and displayed as Kaplan-Meier curves. Differences in hazard between RDEB-GI and RDEB-GS were compared using the Log-rank test. Univariate and multivariate Cox regression was used to analyze hazard ratio (HR) and confidence interval (CI), using likelihood ratio p-value of < 0.05 for statistical significance.
There were 430 patients (including deceased patients) affected with EB in Australia and New Zealand. Forty-eight (11.2%) patients had RDEB. Out of the 48 RDEB patients, 45 were living in Australia (population: 24.2 million), and 3 individuals were residing in New Zealand (population: 4.73 million).
At least one SCC was diagnosed in 35.4% (17/48) of RDEB patients. The earliest age of SCC onset within RDEB population was at 16 years, and the latest was at 62 years. The median age of SCC onset was 30 years. Of the 48 patients, 36 were aged over 16. Hence, the prevalence in those aged over 16 was 17/36 (47.2%). Sixteen out of the 17 RDEB-SCC patients lived, or are currently living in Australia. Twenty-six out of the 48 RDEB patients (54.1%) had RDEB-GI subtype, and 21 patients (43.7%) had RDEB-GS subtype. One patient from New Zealand had RDEB-I. There were 9 males and 8 females who developed SCCs. The RDEB-GS variant was the most prevalent subtype with SCC development, accounting for 64.7% (11/17) with a median age of SCC onset at 23 years (range: 16 to 32 years). The remaining 6 RDEB patients with SCC (RDEB-SCC) had the RDEB-GI variant with a median age of SCC onset at 38 years (range 34–62 years). All 17 RDEB-SCC patients were of Caucasian descent. The individual profile of the RDEB-SCC cohort is summarized in Table I. Out of 17 RDEB-SCC individuals, medical records were only accessible from 16 patients. Eleven out of the 16 (68.7%) RDEB-SCC patients died from metastatic SCC. Their ages at death ranged from 19 to 52 years with a median of 34 years. Two RDEB-SCC patients died from non-SCC-related causes including renal failure and sepsis.
Table I. Individual demographic profiles of recessive dystrophic epidermolysis bullosa (RDEB)-squamous cell carcinoma (SCC) individuals
In Australasian cohort, we have had no SCCs in our JEB population (n = 36) nor DDEB population (n = 73).
Of the 16 RDEB-SCC patients whose medical records on SCC were accessible, a total number of 161 SCCs were observed with a mean of 10 SCCs per patient. The number of SCCs from each ranged from 1 to 56 with a median of 7 SCCs. The temporal frequency of the SCCs had a median of 6 months and mode of new primary SCC every 2–3 months (range 0–143 months). Multifocal SCCs arising in close anatomical sites at the same time were counted as one. Ninety-five percent of the SCCs developed on the upper and lower extremities. Seventy percent of those arose on the hands or feet, mostly in areas of chronic ulcers and non-healing wounds. The anatomical distribution of 161 primary SCCs from our cohort is illustrated in Fig. 1. Except for one SCC on the face, all other SCCs arose from sites that had not been exposed to sunlight for any significant time due to extensive dressings over the wounds and scars.
Fig. 1. A body map outlining 161 primary squamous cell carcinomas by anatomical sites in recessive dystrophic epidermolysis bullosa (RDEB)-generalized intermediate (GI) and RDEB-generalized severe (GS).
Metastatic SCC was observed in 11 out of 16 patients. The metastases were detected by skin biopsy and/or lymph nodal fine needle aspiration, along with imaging modalities including ultrasound, computed tomography (CT), positron emission tomography (PET) and/or magnetic resonance imaging (MRI). Data specific on distant metastasis was available in only 10 of the individuals. Metastases to regional lymph nodes were noted in all 10 of these patients, and metastatic lung disease was found in 8 patients. Metastasis to vertebrae was observed in 3 patients and metastasis to liver, adrenal gland and muscle was found in one patient.
Histopathology reports corresponding to the 161 primary SCCs were obtained from 16 RDEB-SCC individuals. Only 141/161 SCC reports stated the extent of tumour differentiation. One hundred and twenty-nine out of 141 (91.4%) of primary SCCs displayed well or moderately well differentiation. Histological studies of metastatic SCC indicated that the majority (85%) exhibited well to moderate or well differentiated pathology.
A total number of 133 surgical excisions were carried out on 16 patients with SCCs. Out of 133 excisions, 18% (24/133) were incomplete. All 24 incompletely excised tumours were re-excised, and 21 re-excisions were successful. Surgical resection or amputation was recommended and refused by 3 patients. Radical radiotherapy was then utilized to manage these locally invasive SCCs. Amputation was indicated for patients with extensive local spread of the tumour involving fascia, tendon, and muscle. Partial limb amputations were performed in 7 SCCs after MRI imaging suggested tendon invasion. The mean survival time after amputation was 32 months (range 6–51 months). Metastatic SCCs were managed in a different manner to primary SCCs. Eight of 11 patients who developed metastatic SCCs received active treatment (Table I). The two patients treated with cisplatin chemotherapy did not show any tumour response. Of 3 patients administered cetuximab, two had initial shrinkage of the tumour mass, but progressed to develop pulmonary metastases (24). One of the 3 patients was further treated with methotrexate but also showed progression of disease.
The cumulative risk of developing at least one SCC for RDEB-GI was 10% by the age of 35 and increased to 66.7% by the age of 65 (median time to risk: 39 years). For RDEB-GS, 26.3% developed at least one SCC by the age of 20, and 76.1% developed SCC by the age of 35 (median time to risk: 29 years). Fig. 2 illustrates the Kaplan-Meier curve of SCC development by age according to RDEB subtypes. RDEB-GS showed earlier development of SCC compared to RDEB-GI (p = 0.01). On univariate analysis, RDEB-GS compared to RDEB-GI had 4.2 HR (95% CI: 1.4–13.0, p = 0.009). Sex and latitude of the state where the patient resides did not show any difference on univariate analysis although there was a trend towards higher incidence in Queensland. The cumulative risks of SCC-related death in RDEB-GI patients with SCC were 16.6% and 66.6% at age 35 and 52, respectively (median survival: 51 years).The cumulative risks of SCC-related death in RDEB-GS were 30% and 84.4% at age 25 and 34, respectively (median: 29 years) shown in Fig. 3. There was clear evidence of earlier age of death from metastatic SCC in RDEB-GS patients compared to RDEB-GI (p = 0.001). This was in congruence on univariate cox regression with HR of 16.4 in RDEB-GS compared to RDEB-GI (95% CI: 1.9–143.0, p = 0.001). However, age at SCC onset also had a significant impact on outcome. After adjusting for age at onset, RDEB-GS showed a trend towards the higher risk of death compared to RDEB-GI with a hazard ratio (HR) of 2.1 (95% CI: 0.12–37, p = 0.62). In RDEB patients who develop SCC, the median survival time from first SCC development was 5 years for RDEB-GI and 4 years for RDEB-GS.
Fig. 2. Kaplan-Meier survival curve: squamous cell carcinoma development by age of recessive dystrophic epidermolysis bullosa (RDEB) patients.
Fig. 3. Kaplan-Meier survival curve: squamous cell carcinoma-related death by age of recessive dystrophic epidermolysis bullosa (RDEB) patients.
Cutaneous SCC is one of the most devastating complications of RDEB with a high morbidity and mortality rate. Patients with RDEB were reported to have up to a 70-fold higher risk of developing SCC than that of unaffected individuals in the US (15). Some studies have reported SCC development amongst JEB patients (16–18). In particular, one study reported one in 4 JEB patients developed SCC in their cohort of 28 JEB patients (25). In the AEBR, however, we have had no SCCs in our JEB population (n = 36). One red-haired RDEB patient who never had an SCC had a BCC in a sun-exposed site on the forehead at age 22 (26).
This is the first retrospective study on SCC complicating RDEB performed in Australasia using data from the AEBR. In Australia, since 1996 all patients thought to have EB have had their diagnostic biopsies processed at the central lab – South Eastern Area Laboratory Services (SEALS) – based at St. George Hospital in Sydney by Professor Dedee Murrell. The children and adults with EB attend centralized clinics in Sydney, Melbourne, Adelaide and Brisbane; and in Auckland in New Zealand. To receive subsidized dressings under the Australian national EB dressing scheme established in 2009, they have to have a biopsy for direct immunofluorescence (DIF) and electron microscope (EM) or a genetic test which proves EB (27). Hence over the past 20 years, the diagnostic database and EB registry contains the majority of EB patients in Australia and New Zealand. Due to the relatively small population of 24.2 million in Australia and 4.73 million in New Zeeland as well as the rarity of RDEB, our cohort only had 48 RDEB patients. RDEB accounts for 11% of the EB population in Australasia. Consanguinity is uncommon in Australia, but common in certain ethnic groups migrating to Australia, thus the incidence of RDEB is lower than other parts of the world where consanguinity is culturally prevalent.
Australia and New Zealand have the highest prevalence of UV-related non-melanoma skin cancer worldwide (28). The age-standardized incidence rate of SCC was estimated to be 387 per 100,000 in Australia (29). A significant latitude gradient was observed with the highest rates of SCC observed in the Northern region at latitudes less than 29°S, followed by Central region (29°S –37°S) and South region (> 37°S). Taking the body surface into consideration, the face was the most common site for SCC development for both males and females, followed by the neck, dorsum of the hands and forearms (29, 30).
In comparison to the non-EB SCC population in Australia, our data shows that SCC in RDEB most frequently develops on the upper and lower extremities, particularly over bony prominences. Unlike non-EB SCCs in Australasia, these are the sites where the skin is covered with dressings with minimal sun exposure. Most of these SCCs arose from chronic non-healing ulcers, suggesting a different pathogenesis in RDEB. This agrees with the common finding observed in EB-SCC cases in the literature (15). There are a few documented cases of extracutaneous SCC, such as SCC of the hard palate and oesophageal SCC in RDEB (19, 20). This was not observed in our RDEB cohort. The difference in latitudes in SCC development seen in the non-EB Australasian group was not found in our cohort although there was a slightly higher incidence in Queensland than other states. This further suggests that sun exposure is unlikely to be directly contributing to the RDEB-SCC development. In our cohort, the youngest age at which SCC developed in RDEB was 16 years. In the literature, the youngest patient with RDEB with SCC development was only 6 years old from India (21). Both sexes are equally affected by SCC in our cohort, which is identical to that reported by the NEBR (22). Ethnicity does not, according to the NEBR data, play a role in SCC development. Certainly, RDEB-SCC has been reported in darker pigmented races, not just in Caucasians (21, 31). In our cohort, all RDEB with SCC were of Caucasian descent. However, this is most likely a reflection of the cultural background of adult patients in the AEBR. Most RDEB patients (40/48) in the AEBR are of Caucasian descent, and this is mirrored in the RDEB-SCC cohort. Furthermore, patients of other ethnicities such as Indonesian, Korean, Arabic, Chinese or Indigenous Australian are mostly under 16 years of age, and these patients will need to be followed up throughout their adult life to determine any correlations between ethnicity and risks of SCC. There is one case of RDEB-GS female of mixed Chinese/Caucasian heritage who is aged 30 and had not developed any SCCs.
Multiple primary SCCs occurred in most patients, with a mode interval from one primary to the next being 2–3 months. In our RDEB-SCC cohort, 68.7% developed metastatic SCC, which is much higher than the rate of 5.2% in the non-EB population. RDEB-SCC is highly aggressive, and we observed 29.8% of SCC development to be multifocal where multiple SCCs concurrently developed nearby each other. A number of primaries did not correlate to the metastatic behaviour of individual tumours. For example, one patient (AEBR number: 329) developed 56 primaries with no metastatic disease whereas another patient (AEBR number: 215) developed only 3 primaries with metastatic spread.
It is widely known that SCCs arising in RDEB patients are often well differentiated. Our data supported this with the most of the SCCs being well-moderately differentiated. SCC in these RDEB patients behave aggressively regardless of the tumour grade. This is unlike those in non-EB patients, where the chance of metastasis is much lower in well-differentiated tumours (32). Treatment of SCCs complicating RDEB depended largely on the presence of local invasion or metastases. The patient’s general health and preferences also played a role. The majority of early primary SCCs were managed with full thickness wide excision, in accordance with the literature. Mohs surgery is also documented, but does not confer a better prognosis and has limited availability in Australia, especially in the public sector. Surgical excision with clear margins of detected SCC did not prevent the later occurrence of regional or distant spread from another hidden cutaneous SCC. Furthermore, once the patient develops metastatic disease, there are no proven effective interventions. Working in a multidisciplinary team with plastic surgeons who appreciate the urgency required for rapid arrangement of wide excision is crucial even in the setting of well differentiated tumours.
To date, the NEBR in the United States over the 20-year-period (1986–2006) remains the largest epidemiological study of EB (21). In the NEBR cohort, 22.6% (32/141) of RDEB-GS developed SCC whereas only 9.6% (27/280) with RDEB-GI developed SCC. In the AEBR, the incidence of SCC in RDEB was more than double that of the NEBR; RDEB-GS (52.3%) and RDEB-GI (23%). It is well known that UV radiation can induce local and systemic immunosuppression via immune cell alteration and molecular changes (33). The stronger UV radiation in Australia compared to other countries resulting in relatively higher UV-induced immunosuppression could be one possible postulation for this high incidence. Although RDEB patients are heavily bandaged by dressings, the face and hands are often spared from bandaging and they receive sunlight through their daily living and activities. A similar trend to the NEBR data was observed for the cumulative risk of SCC development in RDEB with RDEB-GS carrying the highest cumulative risk with early SCC development (HR 4.2, 95% CI: 1.4–13.0, p = 0.009). The NEBR data showed that the cumulative risk of SCC development in RDEB-GS was 7.5% by the age of 20 and 51.7% by the age of 30. In our cohort, the risks were 26% at the age of 20 and 64% by the age of 30. RDEB-GI showed relatively slower and later rise in the cumulative risk of SCC development. In our cohort of RDEB-GI, the cumulative risks of SCC development were 10%, 50%, and 50% by age 35, 40, and 45, respectively. The data from the United States was more spread out and showed steady progression with the risk of 17.3%, 24.4%, and 35.8% by age 35, 40, and 45, respectively. This is due in large part to the small sample size of 6 RDEB-GI patients in our cohort. A similar trend was noted for the cumulative risk of death after SCC development. There is a very poor prognosis in RDEB patients who develop SCC. The 5-year survival rate after diagnosis of first SCC is 50% for RDEB-GI and 33.3% for RDEB-GS. The median of survival years were 5 and 4 years in RDEB-GI and RDEB-GS, respectively. After adjusting for age, there was a non-significant trend towards earlier death in RDEB-GS compared to RDEB-GI.
Given the aggressive behaviour of RDEB-SCC, early intervention is the key to improving patient survivability. International consensus guidelines, based on the presentation of this study and others, were recently published (34). Regular skin checks at least every 3 months are therefore vital for early detection of SCC. Any ulcerated areas persisting for more than 3 months, areas with pain and hyperkeratotic areas which are embedded and cannot be soaked off need to be biopsied. Taking serial photographs of chronic wounds as we have been doing since 1998 would be useful to keep track of any subtle changes. Patient education is also important for understanding the need for regular comprehensive skin checks. As non-melanoma skin cancer is so common in Australia, there is a somewhat casual attitude towards having SCC compared to other countries. We have found it rather frustrating trying to ensure compliance with regular monitoring in this at-risk population. Having a bath dedicated to EB patients to facilitate removal of dressings and soaking off crusts is helpful, though some patients prefer removing non-stick dressings “dry”. It will be interesting to investigate if bacterial colonization correlates with patients’ differing wound care practices.
This study is the first epidemiological study of SCC in EB in Australia and New Zealand. We highlighted that the cumulative risk of SCC development and associated death from SCC metastasis in Australasian cohort were much higher than the NEBR data. Patients with RDEB-GS had an earlier onset of SCC and higher mortality rate from SCC compared to patients with RDEB-GI. RDEB-SCC pursues an aggressive clinical course and high mortality. Regular full skin checks with photographic monitoring with a low threshold for biopsy is imperative for early detection and successful intervention to improve patient survivability. Education of families and surgical colleagues about the importance of compliance with a rapid (ideally within a week) excision of biopsy-proven SCCs as is done for melanoma, is imperative.
This study was funded by the Australasian Blistering Diseases Foundation and partial grant support by DebRA Australia.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize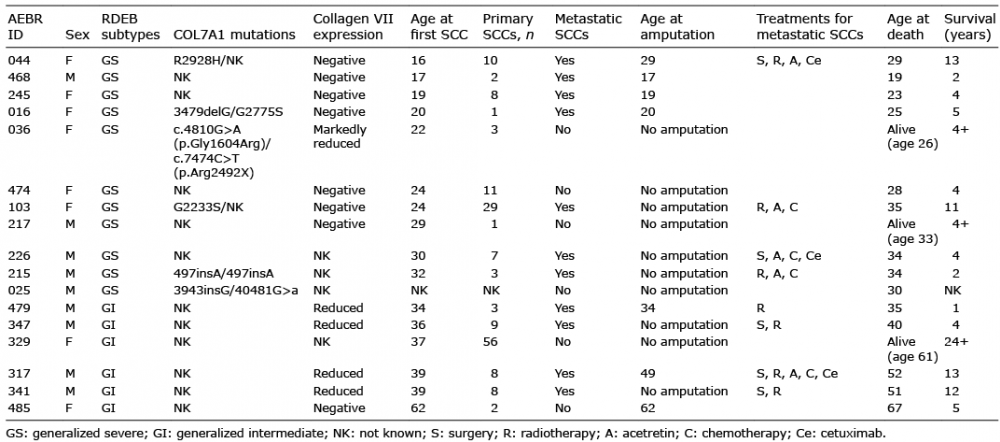 Click to show fullsize
Click to show fullsize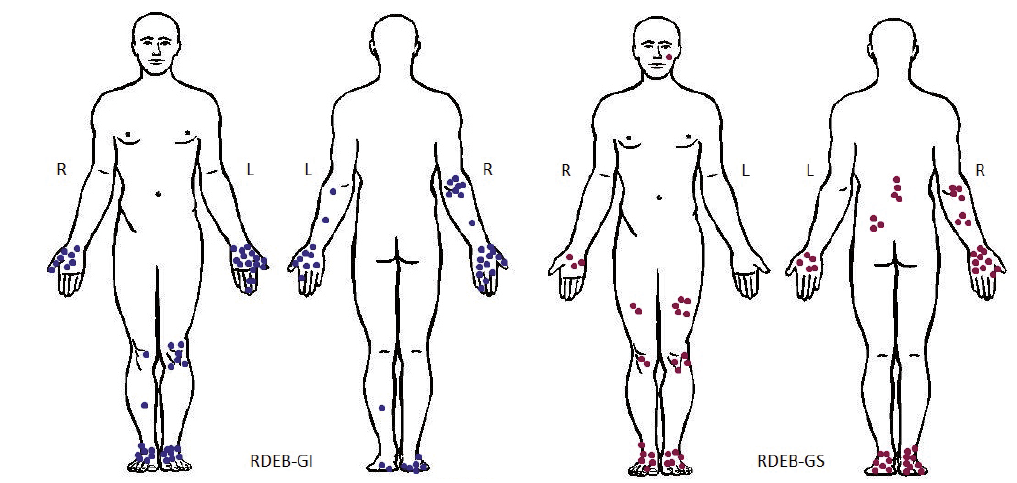 Click to show fullsize
Click to show fullsize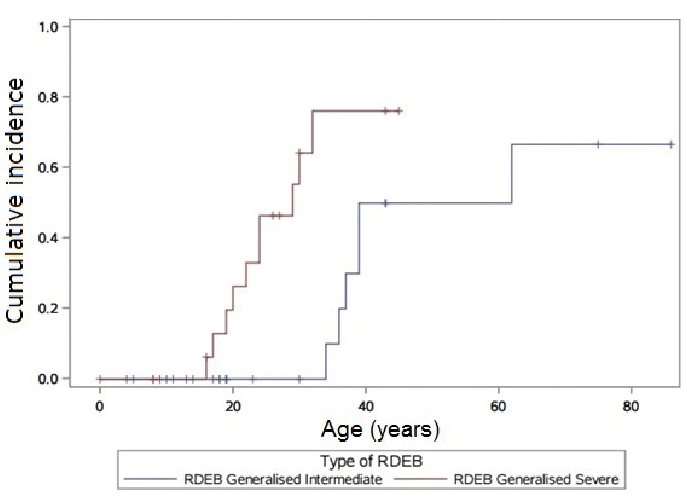 Click to show fullsize
Click to show fullsize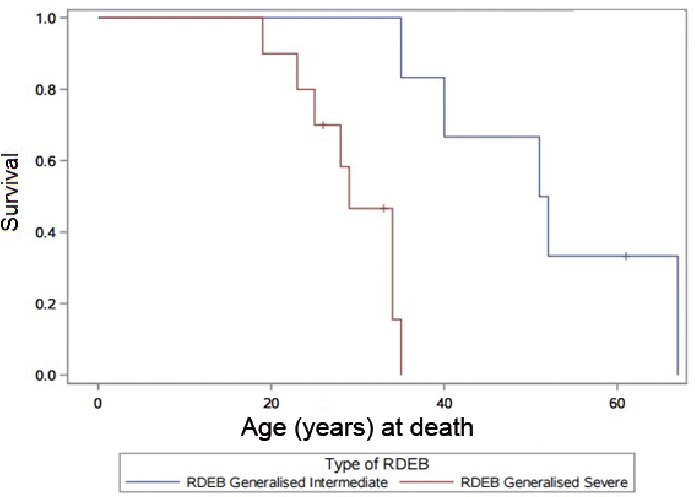 Click to show fullsize
Click to show fullsize