


1Cancer and Population Studies Group and 3Statistics Unit, QIMR Berghofer Medical Research Institute, Brisbane, Queensland, Australia, 2Institute of Cardiosvascular and Cell Sciences (Dermatology Unit), St George’s University of London, London, and 4CRUK Manchester Institute and Institute of Inflammation and Repair, University of Manchester, Manchester Academic Health Sciences Centre, Manchester, UK
Actinic keratoses (AKs) are highly dynamic lesions and AK activity has been shown to be associated with squamous cell carcinoma (SCC). We sought to explore risk factors which may affect the 12-month turnover of AKs in organ transplant recipients (OTRs). The number of incident AKs, regressed AKs and net change in AK counts were calculated. Negative binomial regression and Poisson regression models were used to estimate rate ratios (RR) for these 3 outcomes. Among 150 renal and 89 liver OTRs, those who spent > 50% of a typical weekday in the sun had a lower rate of AK regression than those who spent minimal time in the sun during a typical weekday. Age, parents’ country of origin, hair colour, skin cancer history and recent AK treatment were all significantly associated with AK turnover. Clinically, these risk factors may be used to monitor OTRs at increased risk of SCC.
Key words: actinic keratosis; incidence; regression; solar keratosis; squamous cell carcinoma.
Accepted Aug 29, 2017; Epub ahead of print Aug 30, 2017
Acta Derm Venereol 2018; 98:
Corr: Zainab Jiyad, Cancer and Population Studies Group, QIMR Berghofer Medical Research Institute, Locked Bag 2000 Royal Brisbane Hospital, Brisbane, Queensland 4029, Australia. E-mail: zainabjiyad@doctors.org.uk
Actinic keratoses (AKs) are common sun-induced lesions, a small proportion of which are pre-cancerous and progress to squamous cell carcinoma (SCC) (1). Studies based on histopathological analysis have estimated that approximately 70% of SCCs develop from AKs (2, 3). AKs are highly dynamic lesions that frequently develop, regress and recur in a relatively short period of time (4–6). As such, investigating AK turnover is a challenging process that necessitates regular follow-up at short intervals and detailed mapping. As many as 74% of AKs present at initial examination may have regressed by 12 months (5), with the risk of regression of a single AK estimated to be between 15–63% per year (7). However, following regression, a substantial number of AKs will subsequently recur (4, 5, 8).
Risk factors for AKs that have been identified in prevalence studies in general populations are increasing age, male sex, European ancestry, high cumulative sun exposure and baldness (9–11). In organ transplant recipients (OTRs), the prevalence of patients with AKs increased with longer duration of immunosuppression (12). In a recently published study, we showed that the variability of AKs in a 12-month period is associated with an increased risk of SCC (13). Specifically, we identified an association between AK incidence, net gain of AK and SCC development. However, despite this association, there is very limited literature exploring risk factors affecting the rates of incidence and regression of AKs and thus our aim was to explore this in further detail. We wanted to explore if there were modifying factors that would enable targeted surveillance of AK affected patients beyond simply counting numbers of AK present. The ultimate aim is to reduce the incidence of SCC. We examined the impact of phenotype, sun exposure and various immunosuppression-related risk factors as well as the total number of incident AKs, regressed AKs and overall net gain/loss in AK counts in a high-risk immunosuppressed population.
Renal and liver transplant recipients were recruited in the Skin Tumours in Allograft Recipients (STAR) study, which has been described in detail previously (14). The study received ethical approval from relevant institutional ethics committees in Brisbane, Australia and all participants provided written informed consent.
Successfully recruited participants underwent a full baseline skin examination by a qualified physician. All AKs and suspicious lesions were individually marked on a detailed body map and numbers of AKs were totalled up for each body site. Eye colour, natural complexion and natural hair colour were also recorded. Subsequently, we aimed to re-examine participants at 12-monthly intervals (although re-attendance time varied) and for the purposes of this study we only included participants who attended the second skin examination between 11 and 13 months after the baseline examination (i.e. 12 months ± 1). AKs were diagnosed clinically as rough erythematous papules or plaques with adherent scale (15). An incident AK was defined as an AK identified at the 12-month skin examination which was not present at the baseline examination. Similarly, regressed AKs were present at the baseline examination but absent at the 12-month skin examination.
In addition to skin examinations, participants completed a self-administered health and sun survey questionnaire at baseline. The following sun exposure behaviours were recorded: total lifetime number of painful sunburns (never/once, 2–5 times, > 5–10 times, > 10 times), overall sun exposure during occupations since leaving school (mainly indoors, indoors/outdoors, mainly outdoors), time spent in the sun during a typical weekday in the past year (hardly ever, < 50% of the time, > 50% of the time), wearing long sleeves, wearing a hat and use of sunscreen (never, < 50% of the time, more than 50% of the time, all the time). Additional information collected included age at consent to the study and age at transplantation, sex, place of birth, parents’ country of origin, level of education and history of previous skin cancer. We also recorded current immunosuppression regimen and duration of immunosuppressive therapy (based on time since first transplantation).
Site-specific AK counts were combined to calculate total body AK counts at baseline and 12 months examination. The total number of incident AKs per participant was calculated as the sum of all new AKs on all body sites identified at the 12 month skin examination. Similarly, the total number of regressed AKs was derived by adding all AKs on all skin sites that had regressed at the 12 month follow-up examination.
Where small cell numbers were present, explanatory variable subcategories were combined and reclassified to ensure adequate distribution. This change was applied to ‘eye colour’ (blue/grey, hazel/green, light/dark brown), ‘natural hair colour’ (light: blonde/red, medium: light brown, dark: dark brown/black), ‘natural complexion’ (fair, medium/olive), ‘level of education’ (left school before 15 years of age/junior/senior high, trade certificate/diploma/college/university degree) and ‘number of painful sunburns’ (< 5 times, 5 times or more). Sun protection behaviours were calculated based on use of sunscreen, wearing long-sleeves and wearing a hat for at least 50% of the time, giving a maximum of 3 points if participants used all 3 measures at least half of the time.
We used a negative binomial regression distribution to model AK counts for the outcomes ‘total number of incident AKs’ and ‘12 month AK count’ (indicative of net change in AK count). This model was felt to be most appropriate given the over-dispersion of AK counts and this was demonstrated to show good agreement with the observed distribution using the goodness of fit test. An offset of the total baseline number of AKs was applied using a log-link function to give an indication of changes over time. Due to the presence of zero baseline AK counts (n = 40), the log of the total baseline number of AKs ‘+ 1’ was used as well as the addition of 1 AK count to both outcome variables. For the outcome of ‘total number of regressed AKs’ a Poisson regression model with robust standard errors was used, as this also accounted for over-dispersion but was less susceptible to convergence issues. The calculated rate ratio (RR) provides a measurement of the effect of risk factors on the rate of AK change (based on the 3 outcome variables). As the rate of change of AKs is heavily influenced by the baseline number of AKs, participants were also stratified into those with < 10 total AKs and those with ≥ 10 total AKs, at baseline examination. For the analysis of regressed AKs, those with zero AKs at baseline (n = 40) were excluded as it was not possible for regression to occur in these participants. RRs were calculated using adjustment for age, sex and treatment of AKs in the past 3 months. A p-value of ≤ 0.05 was considered significant. Analyses were performed using the GENLIN models procedure in SPSS v21 (Armonk, NY: IBM Corp).
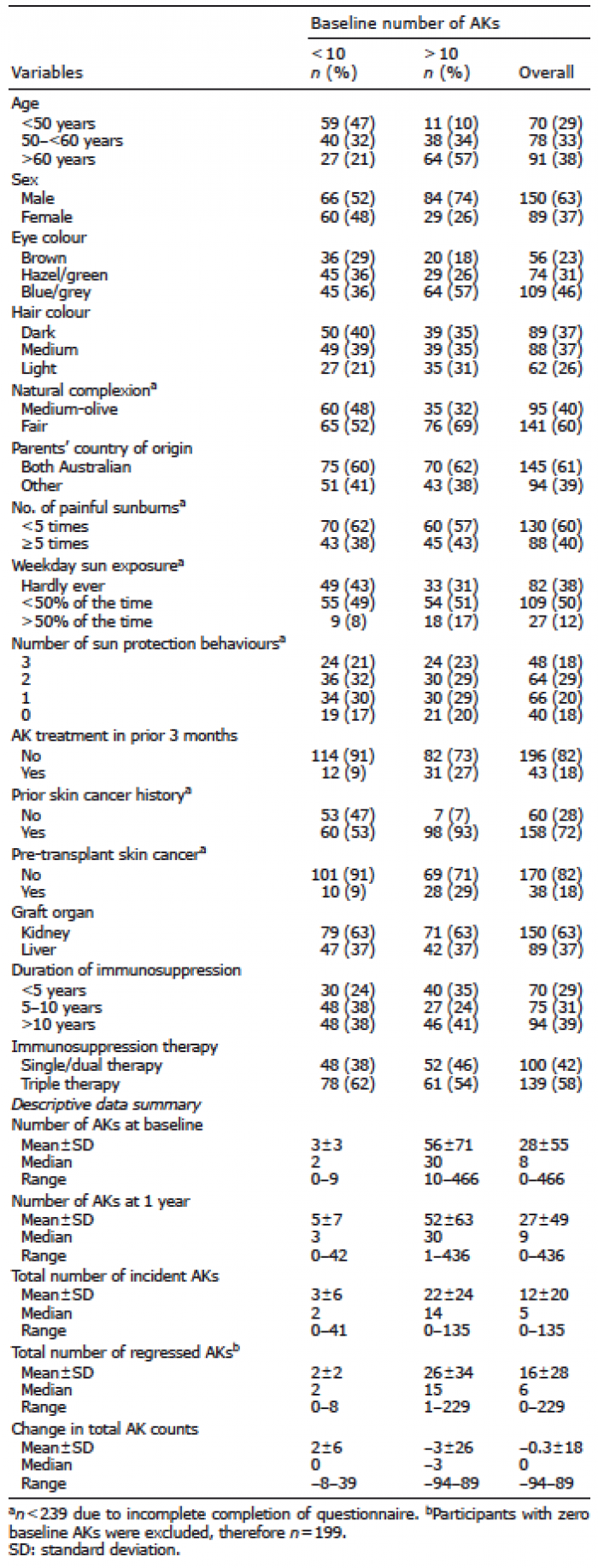
Overall, 239 OTRs completed both the baseline skin check and a second skin examination between 11 and 13 months (inclusive) after the baseline examination. The study population comprised 150 kidney and 89 liver transplant recipients, with a mean ± standard deviation (SD) age of 54 ± 12 years (Table I). The majority of participants were male (63%) and the mean duration of transplantation was 11 ± 9 years. The baseline number of AKs ranged from 0 to 466 with a median of 8 and mean 28 ± 55, with 17% of participants having zero AKs. A total of 126 participants had < 10 AKs at baseline, with the remainder (n = 113) having ≥ 10 baseline AKs. At the 12-month follow-up, the total number of AKs ranged from 0 to 436 with a median of 9 and mean 27 ± 49. No significant association was found between the natural history of AKs and sex, eye colour, natural complexion, sunburn history, sun protection behaviours or any of the immune-related risk factors such as duration of immunosuppression or type of immune therapy.
Table I. Baseline demographics and number of incident actinic keratoses (AKs), regressed AKs and change in total AKs stratified by baseline AKs<10 and AKs of ≥10
The number of incident AKs per participant varied from 0 to 135, with a median value of 5 and mean ± SD of 12 ± 20. In those with < 10 baseline AKs, the rate of incident AKs was two-thirds lower (relative ratio 0.66, 95% CI 0.46–0.95) in participants where one or both parents’ countries of origin were not Australian (Table II). Recent treatment of AKs in the past 3 months, was associated with an increased incidence of AKs in all participants, but the difference was only significant for those with ≥10 baseline AKs (OR 1.53, 95% CI 1.13–2.08).
Table II. Relative ratios (RR) of incidence, regression and total change from baseline to 12 months. Adjusted for age, sex and recent treatment of actinic keratoses (AKs) and stratified by low or high baseline number of AKs
In those with < 10 baseline AKs, the likelihood of incident AKs was 1.97 (95% CI 1.24–3.13) times greater in participants with light (blonde/red) hair colour when compared with participants with dark (dark brown/black) hair colour, although the overall variable did not reach statistical significance. No significant association was identified with any of the sun exposure behaviours or any other medical history variables.
The number of regressed AKs ranged from 0 to 229 with a median of 6 and mean ± SD of 16 ± 28 regressed AKs per participant. In those with < 10 baseline AKs, a pre-transplant skin cancer history was associated with a lower rate of AK regression than those without such a history (RR 0.47, 95% CI 0.26–0.85). When compared with participants who hardly spent any time in the sun during a typical weekday, those who were typically outside for < 50% of the time and > 50% of the time had 21% and 41% lower rates of AK regression, respectively. Treatment of AKs in the previous 3 months showed borderline significance, with a lower regression rate in participants with ≥10 baseline AKs who were receiving treatment (RR 0.79, 95% CI 0.63–1.00). No other significant associations were identified in relation to AK regression.
The overall change in AK counts from baseline skin examination to the 12 month skin check ranged from an overall loss of 94 AKs to an overall gain of 89 AKs, with a median of zero and the mean ± SD change being –0.3 ± 18. In participants with < 10 AKs at baseline, age, parents’ country of origin and prior history of skin cancer were all significantly associated with the rate of overall change in AK counts. Participants who were ≥ 60 years had a rate of change in AK counts that was 1.76 times higher than participants who were < 50 years old (95% CI 1.20–2.58). If one or both parents did not originate from Australia, the rate of change in counts was significantly decreased (RR 0.69, 95% CI 0.51–0.94). Participants with a prior history of skin cancer had a lower rate of change in AK counts, when compared to those where such a history was absent (RR 0.68, 95% CI 0.49–0.93). Recent treatment of AKs was identified as a risk factor, but was significant only in participants with ≥ 10 baseline AKs, with those receiving treatment having a rate 1.4 times greater than participants not treated (95% CI 1.15–1.70). Light hair colour was associated with a greater rate of change in AK counts in those with < 10 baseline AKs: when compared with dark hair colour, the rate of overall AK change in participants with light hair was 1.91 (95% CI 1.28–2.84) times higher; however, this variable had borderline significance (p = 0.05). No other risk factors had significant associations with overall change in AK counts.
There was considerable variation in the turnover of AKs, with the number of incident and regressed AKs within a single OTR in one year ranging from 0 to 229. The baseline prevalence of AKs also varied widely, with total baseline AK counts ranging from 0 to 466. We have identified several risk factors affecting this variation, whilst taking into account the baseline number of AKs. Overall, a significant association was more likely to be found in participants with < 10 baseline AKs, compared with those with ≥ 10 baseline AKs. We postulate that over a certain threshold of baseline AKs, this total number of baseline AKs becomes the overriding factor.
This study is novel in identifying associations with AK variability, as opposed to AK prevalence, which can be used to closely monitor OTRs at increased risk. As one would expect, the results confirm light hair colour and older age to be significantly associated with a greater rate of overall change of AKs. Moreover, OTRs with both parents being of Australian origin were more likely to have a higher rate of AK incidence and overall change in AK counts. This may reflect childhood sun exposure and ethnicity, therefore explaining the increase in AK activity in this subgroup. Interestingly, a prior history of skin cancer (pre- or post-transplant) was associated with a lower turnover in overall AK counts in those with <10 baseline AKs. It is possible that participants with skin cancer were more aware of the increased risk and took greater precautions. However, a pre-transplant history of skin cancer was associated with a lower rate of AK regression.
A significant association with sun exposure was only detected with regards to AK regression in those with ≥ 10 baseline AKs. Participants who were more likely to spend time in the sun in a typical weekday had a lower rate of regression than those who were rarely exposed to sun during a weekday. We did not find any significant association between sun protection behaviours and AK variability in our transplant cohort. This differs from the study of immunocompetent persons by Darlington et al which showed that daily application of sunscreen slowed the rate of AK acquisition, although the mean number of AKs at baseline was 4 in that study, which was much lower than the mean of 28 baseline AKs in our cohort (16). A similar result was detected by Thompson et al, showing a reduction in the mean number of AKs as well as lower incidence and higher regression rates in those randomised to daily application of sunscreen (6). However, our study varied in that participants self-reported their sun protection behaviours and we used a different categorisation system. It may be that poor recall of sun protection behaviour influenced the data collected using the self-administered questionnaire, which led to a failure to identify any significant associations with this factor in our study.
Interestingly, recent treatment of AKs with either topical therapy or cryotherapy in participants with ≥10 baseline AKs was associated with a higher incidence, greater overall change and lower regression of AKs. This may be because those with greater actinic damage are more likely to have treatment, suggesting these patients are more susceptible to variability in AKs. In part, this is supported by the finding that this association was only significant in participants with ≥ 10 baseline AKs. We confirmed there was adequate adjustment in our model to account for those with recent AK treatment by excluding participants with recent AK treatment from analyses and showing results were almost unchanged from those presented.
Our study has highlighted the influence that natural AK regression has on overall clinical control of AKs in OTRs. Previously, this may not have been fully appreciated since it was largely attributed to the success of external treatment.
We used a rigorous assessment method to carefully document total body AK counts and determine overall AK activity in OTRs. However, we acknowledge the limitations of our study: a larger study cohort would improve the RR estimates and our data is limited to OTRs, thus the highlighted associations may not impact significantly on AK change in an immunocompetent population. Furthermore, we used only one data-point to determine AK turnover, although the dynamic nature of AKs means it is likely AKs will have regressed and developed in between baseline examination and 12-month follow-up. However, we believe that a thorough annual skin examination gives a clinically meaningful overview of the activity of AKs in organ transplant recipients, based on our experience of AK evolution in non-immunosuppressed populations (5).
Our study is the first to perform a detailed assessment using a variety of risk factors to analyse the effect on the dynamics of AKs in OTRs, which we have shown to be a significant risk factor for developing SCC (13). Much of the published literature focuses on AK prevalence, but further research is required to understand the dynamics of AKs, allowing us to not only modify associated risk factors and attenuate the risk of SCC, but to also further our understanding of AKs as a whole.
Funding sources: NHMRC Program grants ID 552429 and ID 1073898.
IRB approval: QIMR Berghofer HREC reference number P1481.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize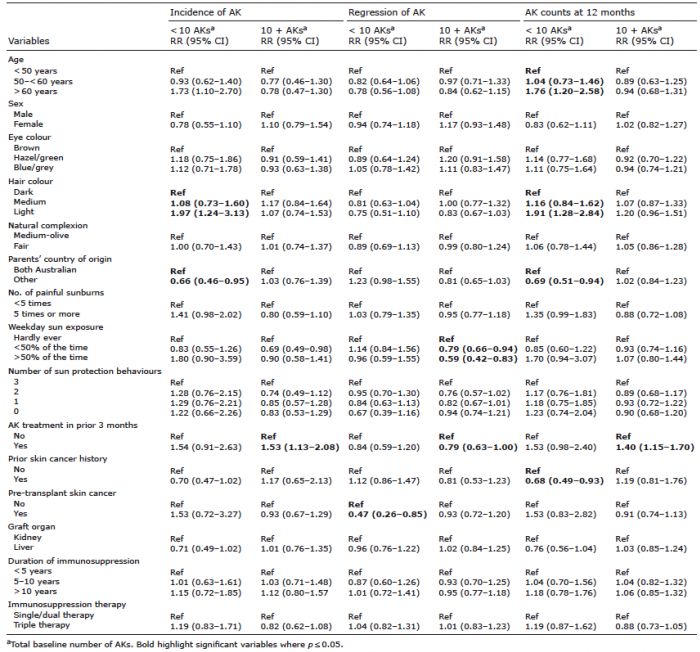 Click to show fullsize
Click to show fullsize