


Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Münster, Germany
Brachioradial pruritus (BRP) and notalgia paraesthetica (NP) represent 2 of the most common neuropathic itch syndromes. A total of 58 consecutive patients presenting at the Center for Chronic Pruritus, University Hospital Münster, were analysed with regard to clinical presentation, anatomical and morphological pathologies, impairment in quality of life, and response to treatment with topical capsaicin. Patients with BRP reported stinging and burning more often than those with NP. In the BRP group structural magnetic resonance imaging abnormalities more frequently correlated with localization of the symptoms compared with in patients with NP. In addition, intraepidermal nerve fibre density was decreased in lesional skin in patients with BRP, but not in those with NP, confirming the neuropathic origin in BRP. Topical capsaicin resulted in a significantly higher alleviation of itch and pain intensity and improvement in quality of life in patients with BRP compared with those with NP, which may reflect clinical and aetiological differences between the conditions.
Key words: dermatome; intraepidermal nerve fibre density; pain; pruritus; quality of life; radiculopathy.
Accepted Sep 13, 2017; Epub ahead of print Sep 13, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Sonja Ständer, Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: sonja.staender@uni-muenster.de
Neuropathic itch syndromes are responsible for approximately 8% of cases of chronic pruritus (1, 2), a highly prevalent and burdensome interdisciplinary symptom as revealed by the Global Burden of Disease (GBD) project (3). Disturbances at any level of the somatosensory system, from the peripheral fibres to the central nervous system, may lead to neuropathic itch syndromes (4). These syndromes share common properties, such as accompanying paraesthetic and dysaesthetic symptoms and relief through the application of cold to the skin (ice-pack sign). Symptoms may vary in their localization and intensity according to the level at which the somatosensory disturbance occurs and the underlying neuropathic mechanism (5, 6). Several different conditions may cause neuropathic itch syndromes, including systemic diseases (e.g. diabetes mellitus), radiculopathy due to nerve impingement, dermatological conditions (e.g. chronic prurigo, sensitive skin) or iatrogeny (e.g. chemotherapy); often the cause is unknown (idiopathic) (7).
Compression syndromes at the spinal level constitute relevant conditions frequently overlooked in the clinical routine (7, 8). These may develop as a result of degenerative alterations of the vertebral column, anatomical variations, tumours, abscesses or aneurysms (7). In brachioradial pruritus (BRP), compression of the cervical spinal cord or the spinal ganglia at C5/C6 occurs, causing unilateral or bilateral pruritus in the forearms (9, 10). Compression of the dorsal branches of the spinal nerves (T2–T6) leads to circumscribed pruritus between the scapulae, a condition known as notalgia paraesthetica (NP) (2, 11). These compression syndromes are often accompanied by other paraesthetic symptoms, such as stinging, tingling or burning sensations, and may lead to lichenification, excoriations or post-inflammatory hyperpigmentation as a result of chronic scratching (2, 7). If the symptoms remain localized, topical capsaicin, a transient receptor potential cation channel vanilloid-1 (TRPV-1) agonist, is the first-line topical therapy (12–14).
Although compression of large nerve fibres occurs in both BRP and NP, quotidian clinical practice suggests differences with regard to their clinical presentation and, especially, with regard to the response to topical capsaicin (15). The aim of this retrospective study of routine clinical data was to characterize both syndromes and compare them with regard to clinical presentation (itch intensity, accompanying paraesthetic symptoms), morphological pathologies (cervical/thoracic magnetic resonance imaging (MRI), intraepidermal nerve fibre density (IENFD)) in lesional skin, psychological co-morbidities (anxiety and depression), impairment in quality of life (QoL) and response to topical capsaicin.
Successive adult patients with BRP and NP presenting at the Department of Dermatology, Center for Chronic Pruritus at the University Hospital Münster, Germany, were considered for inclusion in this retrospective analysis of routine clinical data. Patients were treated and diagnosed according to German guidelines (16). The diagnosis of BRP or NP was performed according to the medical history (localization of symptoms at the onset of the disease, quality of the paraesthetic symptoms, positive ice-pack sign), physical examination (absence of primary dermatoses at the affected dermatomes) and objective examinations (pathological findings in MRI or computed tomography, reduced IENFD in lesional skin). Atopic disposition was assessed using the Erlanger Atopy Score as part of the routine clinical procedures. This study was approved by the local ethics committee (2015-262-f-S) and all patients provided written consent. The study was registered at the German Clinical Trials Register (DRKS00005189).
The analysis period comprised the first routine clinical visit (V1), in which a detailed medical history and a physical examination were performed and an 8% capsaicin patch was applied. Follow-up routine visits occurred 3 weeks (V2), 3 (V3) and 6 months (V4) after the initial visit in some patients. At follow-up visits V3 and V4, treatment with the capsaicin patch was repeated if symptoms persisted, according to treatment guidelines for these conditions. A subset of patients underwent MRI examination of the cervical and thoracic spine to assess for pathological alterations correlating with the symptoms.
A set of standardized routine instruments was used at each visit to document itch, pain, psychological variables and impact on QoL. A visual analogue scale (VAS) was used to assess the mean itch intensity in the past 24 h and the mean itch intensity in the 4 weeks prior to the visit, as well as the mean pain intensity in the 12 h prior to the visit (17, 18). In addition, clinical properties of pruritus (e.g. quality, localization, history and progress, triggers and alleviating factors) were assessed with the Neuroderm questionnaire (19), while neuropathic pain was screened using the PainDETECT Score (range: 0–35) (20). To assess anxiety and depression, patients were asked to complete the Hospital Anxiety and Depression Scale (HADS; range of each subscale: 0–21) at each visit (21, 22). The Dermatology Life Quality Index (DLQI; range: 0–30) was used to measure the impact on QoL in patients presenting with scratch lesions (23). Finally, patients were asked at each visit to evaluate the percentage improvement or worsening of their condition since treatment began (dynamic pruritus score; DPS), using a scale ranging from –100% (absolute worsening of the symptoms) to +100% (absolute improvement of the symptoms) (24).
Using a 4-mm circular blade, punch biopsies were obtained from lesional (i.e. the area in which patients reported itch or paraesthesias) and non-lesional skin (i.e. the area in which no symptoms were reported) on the forearms at dermatome C6 in patients with BRP and on the back in patients with NP under local anaesthesia with lidocaine 2%.
Quantification of the IENFD was performed as described previously (25). In brief, after fixation with 4% paraformaldehyde for at least 2 h at 4°C, biopsies were treated with sucrose solutions (5%, 10%, 20% + 10% glycerol; each for 2 h) and kept at –20°C in liquid nitrogen. Cryosections (40 μm) were then incubated with the primary antibody against the protein gene product 9.5 (PGP 9.5; rabbit polyclonal, 1:200, Zytomed, Berlin, Germany) and stained with the secondary antibody anti-rabbit-fluorescein isothiocyanate (FITC; 1:50; pig anti-rabbit immunoglobulin FITC; Dako, Glostrup, Denmark).
At 400× magnification, the number of intraepidermal nerve fibres crossing the basement membrane was divided by the length of the epidermis assessed using the Olympus DP soft analySIS Image Processing software (v. 3.2, Olympus, Tokyo, Japan) (26). This procedure was performed in 3 specimens per biopsy and the mean value was considered as the IENFD (26, 27).
Prior to treatment with an 8% capsaicin patch (Qutenza® 179 mg, 640 μg/cm, 14×20 cm), the affected area was treated with an anaesthetizing cool gel (4% lidocaine/menthol cream) for 1 h. To avoid excessive burning, scratch lesions, if present, were covered with a wound ointment. Patients then received a maximum of 4 patches, applied carefully to the affected skin without forming folds or creases, for 1 h.
Statistical analysis was performed using SPSS software 24.0 (IBM, Armonk, NY, USA). Q-Q residual plots were inspected and the Kolmogorov–Smirnov test used to analyse normality of data distribution. Group comparisons were performed using the χ2 test or Fischer’s exact test, as appropriate, for categorical data. Comparisons between patients with BRP and those with NP were performed using the non-parametric Mann–Whitney U test, while the Wilcoxon test was used for comparisons within groups. We set the level of significance for statistical comparisons to 0.05. Frequency of observations is presented as the number of observations/total number of assessments. Parametric data are presented as mean ± standard deviation (SD), while non-parametric data are shown as median [interquartile range; IQR].
A total of 58 patients was included in this observational analysis (BRP: n = 29, 19 females, age: 61.5 ± 8.1 years; NP: n = 29, 21 females, age: 62.7 ± 11.5 years). There was no difference between groups in terms of age (p = 0.66, t-test), sex (p = 0.32, χ2) or atopy scores (BRP: 5.0 ± 4.4, n = 25; NP: 4.9 ± 5.6, n = 26; p = 0.98). Screening for comorbidities, we recorded differences in the frequency of diabetes mellitus (BRP: n = 8/29, NP: n = 1/29; p = 0.025, Fischer’s exact test), hepatic conditions (BRP: n = 7/27, NP: n = 1/29; p = 0.023, Fischer’s exact test) and nephrological diseases (BRP: n = 4/27, NP: n = 0/29; p = 0.031, Fischer’s exact test). No differences (p > 0.05) were observed in the frequency of pathological conditions in other systems (cardiological, pulmonary, thyroid gland, gastro-intestinal, urogenital, gynaecological, chronic infections, haematological, lymphoproliferative, malignancies, neurological, psychiatric, rheumatological, phlebological, B symptoms and surgeries).
A total of 25 patients with BRP and 21 with NP underwent a MRI. Degenerative alterations (BRP: n = 6; NP: n = 8), stenosis (BRP: n = 5; NP: n = 2) and a combination of stenosis and degenerative abnormalities (BRP: n = 14; NP: n = 4) were recorded, while 7 patients with NP exhibited no pathologies. The localization of the pathological alterations correlated with symptom localization in 24/25 patients with BRP and 11/22 patients with NP (p < 0.001, χ2).
A total of 20 patients with BRP and 10 with NP had scratch lesions (p = 0.009, χ2). In the BRP group, 16 patients presented single lesions, while 4 had multiple lesions; 10 patients with NP had single lesions. There was no difference in the number of patients presenting with xerosis (BRP: n = 9, NP: n = 5; p = 0.22, χ2) and only one patient (NP) had a concomitant skin disease.
In total, 21/25 patients with BRP and 17/22 patients with NP reported scratching only when experiencing symptoms (p = 0.72, Fischer’s exact test), while 2/25 BRP and 1/25 NP reported scratching in the absence of symptoms (p = 1.0, Fischer’s exact test). Scratching was seen as an alleviating factor by 11/27 patients with BRP and by 15/26 patients with NP (p = 0.22, χ2) and led to satisfaction in 2/24 patients with BRP and 7/22 patients with NP (p = 0.066, Fischer’s exact test). More patients with BRP (10/22) reported scratching until bleeding compared with patients with NP (1/22; p = 0.02, χ2), whereas more patients with NP reported using objects to scratch (p = 0.01, Fischer’s exact test).
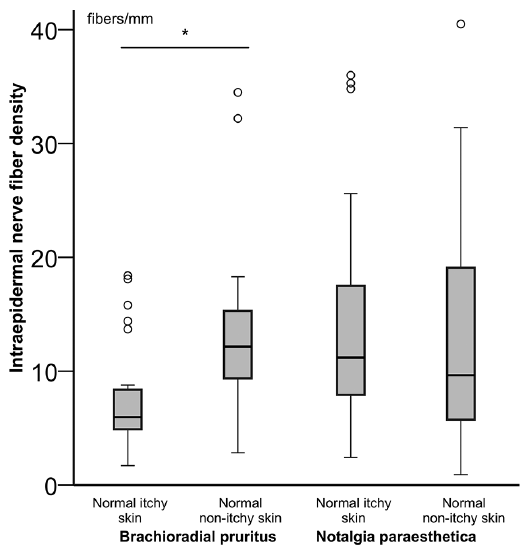
Rarefication of the IENFD in lesional skin compared with non-lesional skin was recorded in patients with BRP (lesional skin: 6.0 fibres/mm [4.9; 8.4], n = 27; non-lesional skin: 12.2 fibres/mm [9.7; 15.3], n = 18; p = 0.01, Wilcoxon) but not in those with NP (lesional skin: 11.2 fibres/mm [7.9; 17.5], n = 25; non-lesional skin: 9.6 fibres/mm [6.3; 17.6], n = 24; p = 0.47, n = 24, Wilcoxon; Fig. 1). There was no difference in the IENFD of patients presenting with scratch lesions compared with those with undamaged skin, in either the BRP group (p = 0.56) or the NP group (p = 0.87; Fig. 2).
Fig. 1. Intraepidermal nerve fibre density (IENFD) in lesional and non-lesional skin. Patients with brachioradial pruritus showed a decreased IENFD in lesional (normal-looking, itchy) compared with non-lesional (normal-looking non-itchy) skin (p = 0.01), while no difference was observed in patients with notalgia paraesthetica (p = 0.47). *p < 0.05. Circle: outlier.
Fig. 2. Intraepidermal nerve fibre density (IENFD) of lesional (normal-looking, itchy) skin stratified by overall presence of scratch lesions. Patients with brachioradial pruritus presented with no (light-grey, n = 8), single (grey, n = 15) or multiple (dark-grey, n = 4) scratch lesions. No differences in IENFD were recorded between patients with and without scratch lesions in lesional skin (p = 0.56). Patients with notalgia paraesthetica presented with (light-grey, n = 16) and without (dark-grey, n = 9) scratch lesions. No differences in the IENFD were recorded between these groups (p = 0.87). Circle: outlier.
All patients (BRP: n = 28/28; NP: n = 28/28) reported having the disease for 6 weeks or longer.
In the BRP group affected dermatomes ranged from C4 to T3, with most of the patients having involvement of C6 (n = 27/29) in combination with other dermatomes. Twenty-four patients had exclusive involvement of cervical dermatomes, and 5 had additional involvement of thoracic dermatomes. The number of affected dermatomes differed between individuals (1 dermatome: n = 1; 2 dermatomes: n = 13; 3 dermatomes: n = 8; 4 dermatomes: n = 4; 35 dermatomes: n = 3; 6 dermatomes: n = 1). In the NP group affected dermatomes ranged from C6 to L4, with all patients having involvement of the upper back (C6–T8) and 9 patients also having involvement of the lower back (T9–T12). In addition, the number of affected dermatomes varied between patients (≤ 3 dermatomes: n = 10; 4–6 dermatomes: n = 11; > 6 dermatomes: n = 8).
All patients in both groups reported neuropathic symptoms. Interestingly, all patients with BRP experienced more than one symptom at the same time (e.g. itch and stinging in 17/28 patients or itch and burning in 16/28 patients). Seven of 28 patients with NP reported having pure itch without other paraesthesias, while the majority of patients experienced a combination of neuropathic symptoms (e.g. itch and tingling in 12/28 patients or itch and stinging in 9/28 patients). The ice-pack sign was positive in 18/27 patients with BRP and 13/27 with NP (p = 0.30, χ2). Most patients reported the occurrence of peaks of itching (BRP: n = 20; NP: n = 14), while 23 reported having continuous symptoms (BRP: n = 9/29; NP: n = 14/28; p = 0.14, χ2). The most frequently reported symptoms, affective sensations, trigger factors and alleviating measures are shown in Table I.
Table I. Most prevalent paraesthetic symptoms, affective qualities, trigger factors and alleviating measures recorded for brachioradial pruritus (BRP) and notalgia paraesthetica (NP) patients using the Neuroderm questionnaire (19)
At the first routine visit (V1), prior to the application of the capsaicin patch, no differences were recorded between patients with BRP and those with NP with regard to the mean itch intensity over the previous 24 h, mean itch intensity in the 4 weeks prior to the visit, mean pain intensity in the 12 h prior to the visit, and the PainDETECT score (p > 0.05). Moreover, scores for anxiety and depression assessed by the HADS, QoL assessed by the DLQI and the patient-reported DPS did not differ between groups (p > 0.05; Table II).
Table II. Comparison of itch, pain, anxiety, depression and quality of life between patients with brachioradial pruritus (BRP) and notalgia paraesthetica (NP) throughout the routine care visits
All patients were treated with topical capsaicin at the first routine visit (V1). Eight patients with BRP and 9 with NP repeated the application of capsaicin 3 months afterwards (V3), while in 4 patients with BRP and 3 with NP capsaicin was applied once more 6 months after the initial visit (V4).
Three weeks after application of the capsaicin patch (V2), the mean itch intensity in the previous 24 h and in the 4 weeks prior to the visit, as well as the mean pain intensity in the 12 h prior to the visit were significantly lower in patients with BRP compared with those with NP (p ≤ 0.01; Table II). Thus, the DPS was higher and the DLQI score lower in patients with BRP compared with those with NP (p < 0.03, Table II). No differences were recorded in the remaining parameters (Table II). Three months after the first visit (V3), the mean itch intensity over the previous 24 h and the mean pain intensity in the 12 h prior to the visit were lower in patients with BRP compared with those with NP (p < 0.05, Table II), while the DPS was higher in patients with BRP (p = 0.01, Table II). Finally after 6 months (V4), the mean itch intensity over the previous 24 h and over the 4 weeks prior to the visit and the mean pain intensity in the 12 h prior to the visit were lower in patients with BRP compared with those with NP (p < 0.01; Table II).
Analysing each patient group separately, patients with BRP showed a decrease in the mean itch intensity over the previous 24 h (V2 and V4, p = 0.01), mean itch intensity in the 4 weeks prior to the visit (V2, p = 0.01), mean pain intensity in the 12 h prior to the visit (V2–V4, p = 0.001), PainDETECT score (V2–V4, p < 0.03), anxiety score (V2–V3, p < 0.02), depression score (V2–V4, p = 0.005) and DLQI score (V2–V4, p < 0.01) compared with pre-treatment scores. No significant changes in the analysed parameters were recorded in patients with NP.
Although BRP and NP are both considered neuropathic itch conditions, we recorded differences in the reported accompanying symptoms, such as paraesthesias, mor-phological pathologies and treatment responses.
Patients with BRP more frequently reported stinging, burning and a needle-prick sensation in addition to pruritus. These paraesthesias are typically associated with neuropathies (28). In addition, 7 patients with NP reported pure itch without concomitant neuropathic symptoms, which was not the case in any patient with BRP. These observations suggest that the neuropathic component in BRP is more pronounced and clinically defining than in NP, where other factors may also play a role.
Thus, we observed a consistent correlation between anatomical abnormalities detected by MRI and the localization of the symptoms in the corresponding dermatomes for patients with BRP (24/25), but only in half of the patients with NP. Previous observations have, however, linked NP to cervical spinal stenosis and nerve root impingement (29–32). In fact, osteopathic manipulative treatment has alleviated symptoms, as reported in a few instances (33, 34). The association between BRP and cervical spine pathology is well documented and in accordance with our findings (10, 35). Anatomical abnormalities leading to NP may be more difficult to identify using imaging techniques, explaining the discrepancy in the findings. It should be noted that the posterior rami of the spinal nerves travel backwards after leaving the intervertebral foramen, creating a pronounced angulation, and thus are more prone to traumatic injury. This is especially the case during specific movements, e.g. when protecting and elevating the scapulae and flexing the head (34). In these cases nerve impingement may be difficult to detect by standard imaging procedures, including cutaneous innervation.
Regarding cutaneous innervation, we detected a rarefication of the intraepidermal nerve fibres in lesional skin of patients with BRP, confirming previous reports (36), but not of patients with NP. Thus, earlier observations did not detect a significant difference in immunohistochemical signalling of neural markers in lesional skin of patients with NP compared with control tissue (37). Our data showed that more patients with BRP (n=20) presented with scratch lesions compared with patients with NP (n=10). In addition, scratching until bleeding was reported by more patients with BRP than by patients with NP (10/22 vs. 1/22). However, this cannot account for the reduced IENFD observed in lesional skin of patients with BRP, since no difference was recorded in the IENFD of patients presenting with scratch lesions compared with those with undamaged skin. These data suggest that cutaneous neuroanatomical alterations result from an endogenous neuropathy, rather from external scratching activity. Interestingly, epidermal nerve fibre abnormalities normalize in symptom-free periods or after remission of BRP (36), arguing for the plasticity of this neuropathic process.
Based on these findings, we hypothesize that the origin of nerve compression might contribute to the more pronounced neuropathic symptomatology in BRP compared with NP. While nerve impingement is often found at a central level in BRP, in NP nerve damage seems to occur more peripherally. Regarding the differences in cutaneous neuronal anatomy recorded between BRP and NP, central nerve compression may trigger a retrograde degeneration of small-fibres, while more peripheral impingement may not suffice to induce such alterations.
Despite the clinical and neuroanatomical differences between patients with BRP and those with NP, both groups showed similar moderate itch and pain intensities at the first routine care visit. Anxiety and depression, as well as QoL scores did not differ between groups prior to treatment. Several affective qualities attributed to the itch were similar in both groups (depressive, aggressive, stubborn, cruel), while significantly more patients with BRP described the symptoms as agonizing. This may reflect the more frequently reported accompanying paraesthesias, such as needle pricks, in the BRP group. Sex did not differ between patient groups, and thus a possible sex effect on the reported symptoms cannot explain the observed discrepancies. Regarding alleviating measures, patients with NP more often reported resorting to devices to scratch than did patients with BRP. While the arms are easily accessible for patients with BRP, the upper back is not, and thus patients with NP use devices to reach the affected areas.
Interestingly, response to capsaicin varied across these 2 groups. Patients with BRP reported a significantly higher improvement in itch and pain intensity, as well as in the DPS, and consequently in the life quality index, anxiety and depression scores. This is in line with previous studies demonstrating high efficacy of capsaicin in the treatment of BRP (12, 13), while some studies of NP point to efficacy of a capsaicin patch (14, 38–40), and other reports suggest a high variability in the response to capsaicin (15, 41).
Capsaicin exerts its effects peripherally by depleting neuropeptides from peripheral fibres and destroying small epidermal sensory nerves (42). Interestingly, cutaneous innervation was altered in patients with BRP, who responded better to treatment, but not in patients with NP. Morphological abnormalities in cutaneous nerves may thus favour the effect of topical capsaicin in patients with neuropathic pruritus. Immunohistochemical studies should focus on the underlying pathways at the molecular level to better determine the mechanisms of action of capsaicin and thus explain our clinical observations.
Patients with BRP reported sweating as a trigger factor for pruritus more frequently than patients with NP. Sweating is a common trigger for pruritus induced by atopic disposition, as is the case, for instance, in atopic dermatitis. However, the 2 patient groups did not differ in the Erlanger Atopy Score, a widely used scale to assess atopic disposition. Thus, atopic disposition does not seem to explain the clinical differences observed in the present analysis. Other trigger factors were similar between the 2 groups (scratching, being relaxed, bed warmth and tension) and are common to pruritus of various origins.
A limitation of this study of routine clinical data is the higher frequency of diabetes mellitus registered in the BRP group compared with the NP group (9). Diabetes mellitus may cause nerve damage (typically starting in the lower legs) and induce neuropathic symptoms, as well as altered peripheral nerve morphology (43). However, this condition was recorded in only 7 patients with BRP and one patient with NP, and thus cannot account for the neuropathic symptoms and morphological alterations observed in the majority of patients with BRP. Prospective studies excluding patients with diabetes mellitus and other diseases leading to neuropathy are needed.
Although regarded as neuropathic itch syndromes, there are important differences in the clinical presentation and morphological pathologies of BRP and NP. Patients with BRP more frequently report neuropathic symptoms. In addition, structural MRI abnormalities more often correlate with the localization of the symptoms in BRP, and the IENFD is decreased in lesional skin of patients with BRP but not of those with NP. Capsaicin shows higher efficacy in the treatment of BRP compared with NP, which may reflect the clinical and morphological discrepancies between the 2 diseases. Further prospective high-quality studies are needed to confirm these observations.
This article was supported by the Interdisciplinary Center for Clinical Research (IZKF; No. CTRP 07 to SST) and by the European Academy for Dermatology and Venereology (EADV, No. 2016-012 to MP).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize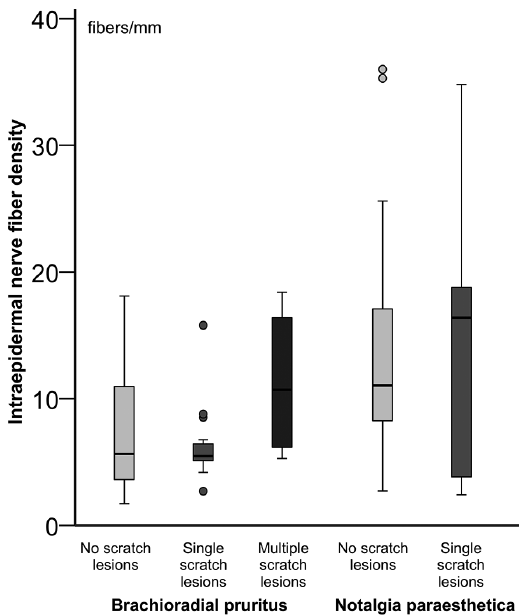 Click to show fullsize
Click to show fullsize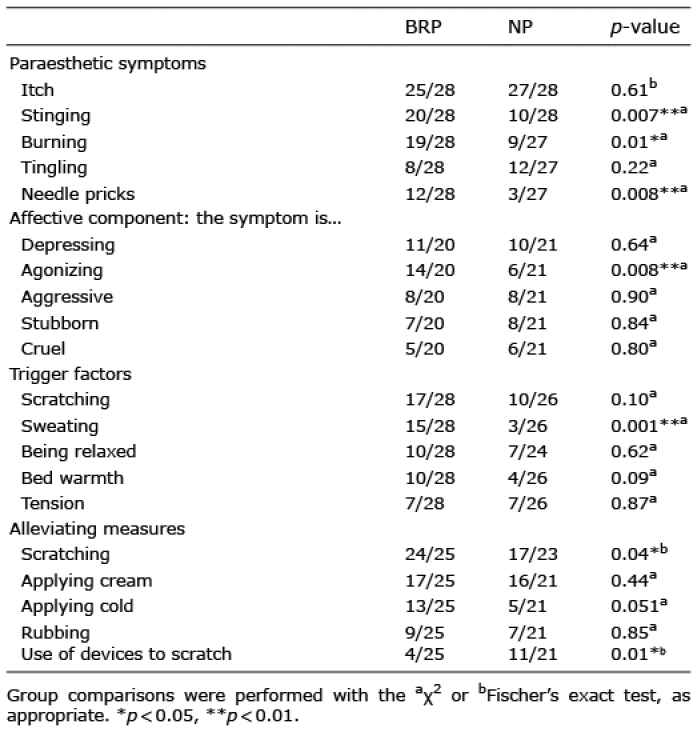 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize