


Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Carrer de Sant Quintí, 89, ES-08026, Barcelona, Spain. E-mail: splanas@santpau.cat
Accepted Sep 13, 2017; Epub ahead of print Sep 13, 2017
Primary localized cutaneous nodular amyloidosis (PLCNA) is a rare form of primary localized cutaneous amyloidosis characterized clinically by solitary or multiple nodules. Although the prognosis is usually good, an extensive work-up must be performed in all patients with PLCNA, since it is both clinically and histopathologically indistinguishable from systemic amyloidosis in up to 40% of cases.
Recently, high-frequency ultrasound (HFUS) has emerged as a non-invasive imaging method in dermatology. It has been shown to be of significant value for the study of certain skin tumours or inflammatory conditions. To our knowledge there are no published reports of ultrasound findings in PLCNA.
We report here a case of PLCNA with dystrophic calcification with ultrasound findings. Dystrophic calcification is rarely found in PLCNA, but has been reported in cases of localized amyloidosis of other organs. Thus, we suggest that PLCNA should be included in the differential diagnosis of subcutaneous nodules with dystrophic calcification.
An 84-year-old woman with a medical history of primary biliary cirrhosis, autoimmune hepatitis and Sjögren’s syndrome was referred to the dermatology department for evaluation of 2 painful lesions of 1 year’s duration on the right leg. Physical examination revealed a 3.5-cm, well-defined, yellowish, firm, nodule on the medial side of her right ankle (Fig. 1a) and a 2.5-cm, ill-defined, yellow patch with focal brown areas on the right knee. No other clinical features were observed.
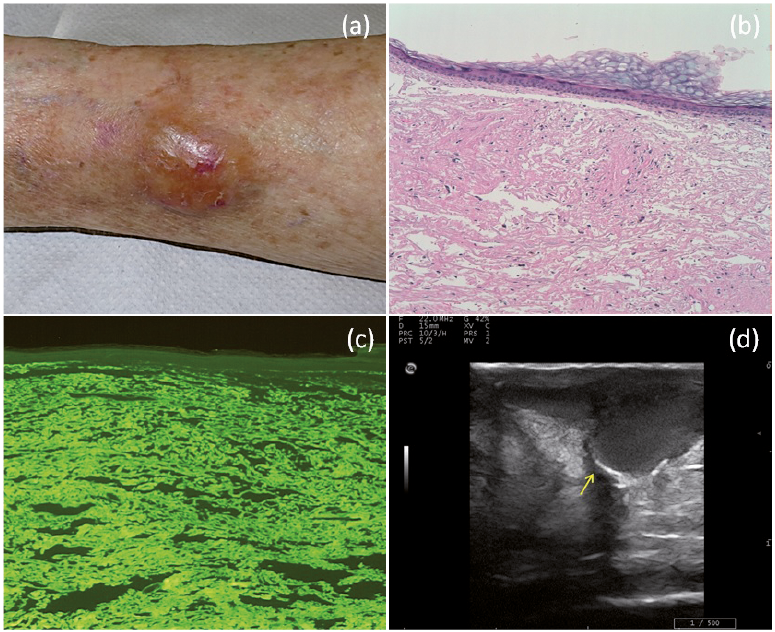
Fig. 1. Clinical, histopathologic and ultrasound features of the skin lesion. (a) A 3.5-cm, well-defined, yellowish, firm nodule on the medial side of the right ankle. (b) Diffuse eosinophilic amorphous material in the entire dermis (haematoxylin and eosin stain ×200). (c) Thioflavin staining revealed an apple-green birefringence, indicating amyloid deposits within the dermis. (d) Ultrasound image showing an ill-defined heteroechoic mass in the dermis and subcutaneous tissue, and hyperechoic lineal foci with distal acoustic shadowing suggesting calcification (arrow).
High-frequency 22-MHz skin ultrasound of the nodular lesion revealed an ill-defined heteroechoic mass in the dermis and subcutaneous tissue and hyperechoic lineal foci with distal acoustic shadowing suggesting calcification (Fig. 1d). A skin biopsy from the nodule showed a diffuse infiltration of the entire dermis and subcutaneous tissue by an eosinophilic amorphous material (Fig. 1b). A perivascular infiltrate of plasma cells with Russell bodies and the presence of focal dystrophic calcification were also observed. The eosinophilic amorphous material stained apple-green with thioflavin T (Fig. 1c), and immunohistochemistry studies revealed a predominance of kappa light chains.
An extensive work-up was performed to rule out systemic amyloidosis, including serum and urine protein electrophoresis, complete blood count, metabolic panel, electrocardiography and chest radiography, which were normal. Neither typical cutaneous findings of systemic amyloidosis nor internal organ involvement were observed. Based on the clinical, pathological and laboratory findings, a diagnosis of PLCNA was made.
Amyloidosis constitutes a heterogeneous group of diseases characterized by tissue deposition of a misfolding protein, called amyloid. Clinically, it is classified into 2 main types: systemic amyloidosis and localized amyloidosis. Primary localized cutaneous amyloidosis is characterized by amyloid deposits in the skin without internal organ involvement, and includes 3 variants: macular, lichen and nodular amyloidosis. In macular and lichen amyloidosis, amyloid derives from epidermal keratinocytes and its deposition is limited to the papillary dermis. By contrast, in PLCNA, amyloid derives from the immunoglobulin light chain produced by plasma cells, as in primary systemic amyloidosis, and may involve the entire dermis. An extensive work-up must be performed in all patients with PLCNA, since it is both clinically and histopathologically indistinguishable from systemic amyloidosis in up to 40% of cases (1, 2). Although PLCNA has been classically associated with a high risk of developing systemic amyloidosis (3, 4), recent reports have shown a much lower risk (< 7%) of progression to systemic amyloidosis (5). PLCNA usually has a good prognosis. Nevertheless, proper follow-up and systemic evaluation is always required due to the risk of progression to systemic amyloidosis. Although the pathogenesis remains unclear, PLCNA has been linked to different autoimmune diseases, such as CREST (calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia), rheumatoid arthritis, primary biliary cirrhosis and, especially, Sjogren’s disease (which is related to PLCNA in up to 25% of reported cases) (1, 2). Several therapies have been used in patients with PLCNA, but due to high rates of local recurrence, some authors recommend treating only symptomatic cases (1, 2).
Recently, high-frequency ultrasound (HFUS) has emerged as a non-invasive imaging method in dermatology. It has been shown to be of significant value for the study of certain subcutaneous pathologies, such as tumours (lipomas, epidermal cyst, pilomatrixoma and ganglions) or inflammatory conditions (6). HFUS is also considered to be a useful tool for the diagnosis and follow-up of calcium deposits, since it has more sensitivity and specificity than X-ray imaging (7). Dystrophic calcification is rarely found in PLCNA, but have been reported in cases of localized amyloidosis of other organs, such as breast (8), eyelid (9) and lungs (10). Thus, PLCNA should be included in the differential diagnosis of subcutaneous nodules with dystrophic calcification, together with other autoimmune connective tissue diseases, such as cutaneous lupus erythematosus, scleroderma or generalized morphoea.
To our knowledge, this is the first report of ultrasound findings in PLCNA with dystrophic calcification. Further research is needed to fully delineate the specific ultrasound findings of this rare condition.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize