


Department of Dermatology and Allergology, Technical University Munich, Biedersteinerstr. 29, DE-80802 München, Germany. E-mail: thomas.volz@tum.de
Accepted Sep 13, 2017; Epub ahead of print Sep 13, 2017
Hidradenitis suppurativa (HS), or acne inversa, is a chronic recurrent inflammatory skin disease mainly affecting the axillary, inguinal and anogenital region. The estimated prevalence of HS is 1% (1, 2). HS is characterized by deep-seated inflammatory nodules, abscesses and sinus tracts (3). Enhanced expression of tumour necrosis factor (TNF)-α, interleukin (IL)-1β and IL-17 has been reported in HS lesions, and treatment with the anti-TNF antibody adalimumab has been approved for therapy of moderate-to-severe HS (4–6). As response rates to adalimumab range from 40% to 60%, there is an unmet need for further therapeutic options. We report here a case of severe recalcitrant HS treated successfully with the anti-IL-17A antibody secukinumab in a patient refractory to therapy with adalimumab and infliximab. During an 8-week therapy a rapid clinical response was observed, with almost complete disappearance of inflammatory nodules and continuous reduction in the signs of cutaneous inflammation.
A 24-year-old non-smoking patient who had had HS for 6 years presented with recurrent inflammatory nodules and extensive cutaneous inflammation, mainly affecting the groins and gluteal region (Fig. 1A). Previous therapies, including a combination of clindamycin and rifampicin (each at 300 mg twice a day) or isotretinoin 30 mg per day, or anti-TNF-α treatment with adalimumab or infliximab, had had no effect on the severity and course of HS lesions. Wide excision of the abscesses and sinus tracts in both groins and gluteal regions, with subsequent secondary healing, was performed one year before presentation. At presentation the patient had recurrent HS, with many highly inflammatory nodules and extensively affected groins and gluteal area. At baseline (day 0) the patient had a Hidradenitis Suppurativa Score (HSS, modified Sartorius Score) of 90 (Fig. 2A). The HSS takes into account the number of inflamed nodules and fistulas, the dispersion of lesions and the Hurley stage, and is first calculated separately for each affected body area, then summed to produce a final score (7). Laboratory findings at baseline (week 0) revealed leukocytosis, with white blood cell count 13.26×109/l (reference range 4.0–9.0×109/l) and C-reactive protein (CRP) 4.3 mg/dl (reference range < 0.5 mg/dl). In addition, serum amyloid A showed a large increase, at 127.0 mg/l (reference range ≤ 6.4 mg/l).
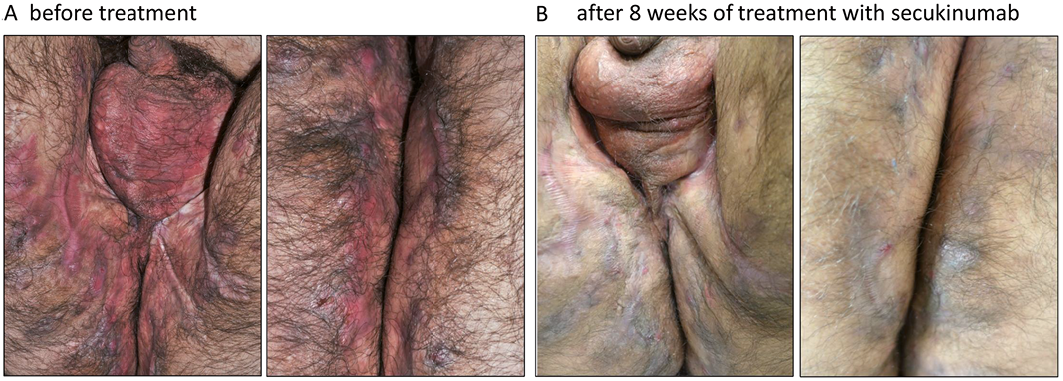
Fig. 1. Rapid clinical response of hidradenitis suppurativa (HS) to secukinumab treatment. Clinical images of the genital and gluteal region (A) before and (B) after 8 weeks of treatment with the interleukin-17A antibody secukinumab, demonstrating rapid reduction in inflammatory nodules and signs of cutaneous inflammation.
Fig. 2. Clinical and laboratory parameters during treatment with secukinumab. (A) Rapid and long-lasting reduction in severity of hidradenitis suppurativa (HS), as measured by the Hidradenitis Suppurativa Score (HSS) during treatment with secukinumab. (B) Continuous decline in serum amyloid A after onset of secukinumab therapy. (C) Normalization of white blood cell count (WBC) and reduction in elevated levels of C-reactive protein (CRP).
Secukinumab was subsequently administered, at a dose of 300 mg weekly for 1 month (days 0, 7, 14, 21 and 28), followed by injections at 4-week intervals. One week after the start of secukinumab treatment a reduction in inflammatory nodules and resolution of the signs of cutaneous inflammation were observed. This therapeutic effect continued over subsequent weeks, resulting in almost complete resolution of inflammatory nodules after 8 weeks (Fig. 1B). A continuous reduction in severity of HS, as scored by HSS, was measured at every visit (Fig. 2A). Serum amyloid A levels paralleled the course of HSS, also showing a continuous decline (Fig. 2B). In addition, normalization of white blood cell count and reduction in CRP levels were observed (Fig. 2C). No adverse effects related to secukinumab therapy were observed during the treatment period.
Treatment of severe HS is challenging. Wide surgical excision is the gold standard for extensive and severe HS lesions presenting with fistulas and sinus tracts (2). Targeting cutaneous inflammation in HS with biologics seems to be a promising strategy, especially when HS presents with a predominance of inflammatory nodules (2). Elevated TNF-α and IL-1β levels have been reported in HS lesions and the anti-TNFα antibody adalimumab was the first biologic approved for therapy of moderate and severe HS (4–6). As IL-17A gene expression in lesional skin and IL-17 serum levels could be shown to be significantly elevated in HS patients (4, 8), we decided to initiate off-label treatment with secukinumab targeting IL-17A. Strikingly, we observed a rapid decline in HS severity, as measured by the HSS after the first injection, leading to almost complete resolution of HS lesions. Moreover, signs of systemic inflammation, as measured by leucocyte counts, CRP and serum amyloid A, rapidly normalized or declined, respectively, indicating that IL-17 is a key cytokine in the pathogenesis of HS inflammation. These findings are consistent with a recently described case report of successful treatment of severe HS with secukinumab, which resulted in a reduction in the number of boils and improvement in pain (9).
In conclusion, with IL-17A antibody secukinumab treatment, our patient underwent substantial and rapid improvement in the clinical and signs of systemic inflammation due to severe HS, demonstrating that targeting IL-17 might be a novel and effective treatment option for HS. Further investigations and randomized clinical trials are needed to evaluate the therapeutic approach of targeting IL-17 in HS.
Conflicts of interest: AB and TB have been supported by Novartis in the past. All other authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize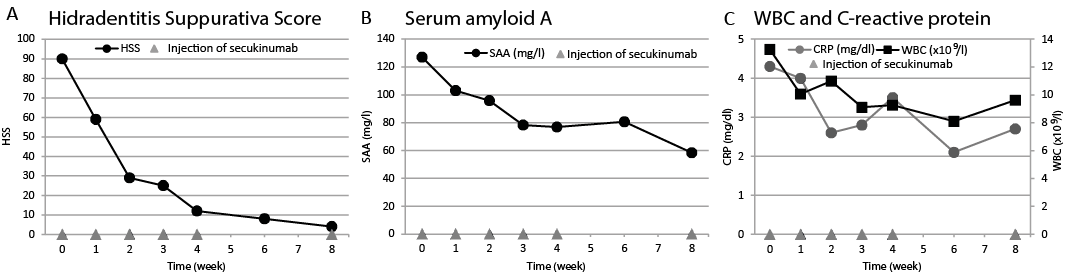 Click to show fullsize
Click to show fullsize