


1Department of Dermatology and Medical Research Center Oulu, PEDEGO Research Unit, University of Oulu, Oulu University Hospital Oulu, 2Center for Life Course Health Research, Faculty of Medicine, University of Oulu and Oulu University Hospital, 3NordLab Oulu, Medical Research Center Oulu, Oulu University Hospital and Department of Clinical Chemistry, University of Oulu, Oulu, Finland
Low grade inflammation is associated with many noncommunicable diseases. The association between skin diseases in general and systemic inflammation has not previously been studied at the population level. A whole-body investigation on 1,930 adults belonging to Northern Finland Birth Cohort 1966 was performed and high sensitive C-reactive protein (CRP) level was measured as a marker of low grade inflammation in order to determine the association between low grade inflammation and skin diseases in an unselected adult population. After adjustment for confounding factors the following skin disorders were associated with low grade inflammation in multinomial logistic regression analysis: atopic eczema (OR 2.2, 95% CI 1.2–3.9), onychomycosis (OR 2.0, 1.2–3.2) and rosacea (OR 1.7, 1.1–2.5). After additionally adjusting for body mass index and systemic diseases, the risks for atopic eczema (OR 2.4, 1.3–4.6) and onychomycosis (OR 1.9, 1.1–3.1) remained statistically significant. In conclusion, low grade inflammation is present in several skin diseases.
Key words: atopic eczema; epidemiology; fungal skin infection; low grade inflammation; rosacea.
Accepted Sep 13, 2017; Epub ahead of print Sep 13, 2017
Acta Derm Venereol 2018; 98: xx–xx.
Corr: Suvi-Päivikki Sinikumpu, Department of Dermatology, Oulu University Hospital, P.B.20, FIN-90029 Oulu, Finland. E-mail: suvi-paivikki.sinikumpu@oulu.fi
Low grade inflammation is a chronic, subclinical and systemic condition (1), which contributes to the pathogenesis of many noncommunicable diseases, such as atherosclerosis (2), type 2 diabetes (3), metabolic syndrome (4), obesity (5), and depression (6). Low grade inflammation is detectable via a minor elevation of certain inflammatory markers, such as C-reactive protein (CRP), and it is usually measured by a high sensitivity CRP (hs-CRP) test (5, 7). Many factors including age, sex, body mass index (BMI) (8), lifestyle factors (9) and ethnic background (10) have an influence on CRP level.
Although several skin diseases such as psoriasis, most eczemas and sebaceous gland diseases (7, 11, 12) have an inflammatory background, the association between skin diseases in general and systemic inflammation has not previously been studied at the population level. The relationship has, to date, only been investigated in a disease-specific manner, most comprehensively among psoriasis patients (7, 11, 12): an extensive meta-analysis of data from such studies has shown that CRP levels are elevated in patients with psoriasis compared with healthy subjects (7). Studies with limited sample size have showed that low grade inflammation is also present in chronic urticaria (n = 58) (13), lichen ruber planus (n = 55) (14) and rosacea (n = 60) (15). Recent studies have demonstrated that children and young adults with atopic eczema or allergic sensitization have elevated CRP levels (16–18). In contrast, no association has been found between acne vulgaris and elevated CRP (12).
By using data from the unique 1966 Northern Finland Birth Cohort 1966 (NFBC1966) we aimed to determine, in an unselected adult population, any association between low grade inflammation and any of the most common skin diseases.
This was a cross-sectional population-based study that drew from the NFBC1966 cohort. Since birth, cohort members, and their mothers since the 1965/1966 pregnancy (in mean from the 16th gestational week), have been followed regularly via health questionnaires and clinical health surveys, resulting in a diverse data set concerning health and life-style.
This population sample included all individuals in the two northernmost provinces of Finland whose expected day of birth fell between 1st January and 31th December 1966 (n = 12,058; 5,889 females and 6,169 males). When the cohort members reached the age of 46 years 10,321 of them were still alive and address was known in Finland. All those living within 100 km of the center of the city of Oulu (n = 3,118; 1,497 females and 1,621 males) were invited to participate in the comprehensive clinical follow-up examination. The data was collected between April 2012 and May 2013. This visit included both health questionnaires and several clinical investigations, including skin evaluation.
The Ethical Committee of the Northern Ostrobothnia Hospital District approved the present study (§94/2011), which was performed according to the principles of the 1983 Declaration of Helsinki. The participants took part on a voluntary basis and signed their informed consent. The data were handled on a group level, with personal information being replaced by identification codes, resulting in complete anonymity.
The clinical examination included a whole body skin investigation of every participant, performed by a specialist (one) in dermatology or experienced resident (two) as described (19). All skin areas were evaluated and all typical skin findings and diseases (benign and malignant skin tumors, skin infections, inflammatory skin diseases, sebaceous gland diseases, hair follicle and autoimmune skin diseases) were recorded in a pre-designed computerized database based on the International Classification of Diseases (ICD-10). The cohort members were categorized into 4 subgroups according to their need of further interventions due to skin disease: I) Subjects with no further care needed, II) those who would recover with self-treatment, III) those to whom a general practitioner visit was recommended, and IV) cases that required further treatment by a dermatologist (19).
In this study cohort members who presented with only benign skin tumors during the skin evaluation were considered as subjects with healthy skin.
Blood samples were taken after overnight fasting and were stored at –70ºC. The concentration of hs-CRP was determined by using an immune nephelometric assay (BN ProSpec, Siemens Healthcare Diagnostics Inc., Newark, DE, USA). The detection limit for hs-CRP was 0.2 mg/l. A value < 1 mg/l was defined as normal hs-CRP, 1–3 mg/l as elevated and > 3 mg/l, highly elevated according to criteria of American Heart association (20).
Sex, BMI, tobacco smoking, the use of oral contraceptives, socioeconomic status, systemic diseases and physical activity were considered as potential confounding factors because their known association with elevated CRP (8).
The information about the use of hormonal contraceptives (the data available of n = 1,930), smoking status (n = 1,859, the data missing in 71 subjects), leisure time physical activity (n = 1,859, the data missing in 71 subjects) and systemic diseases (n = 1,873, the data missing in 57 subjects) was obtained from the health questionnaires of a 46-year follow-up study. Socioeconomic status was categorised by education level (21) and data concerning education were obtained from the National Education Register, supplemented by self-reported questionnaires (n = 1,930) (22). BMI was determined according to the measured weight (kg) and height (n = 1,928, the data missing in 2 subjects). Study participants were classified into 3 groups according to BMI: (i) normal or underweight ≤ 25, (ii) overweight 25–30 and (iii) obese ≥ 30. The reasons for missing data were that all study cases did not fill the health questionnaires or come to the weighing.
The overall prevalence of all common skin diseases and the mean hs-CRP values were calculated. A Chi-square-test and Fisher’s exact test (when appropriate) were used to test difference between hs-CRP groups (< 1 mg/l, 1–3 mg/l and > 3 mg/l). Continuous variables were expressed as mean and standard deviation (SD) or median and interquartile ranges (Q1–Q3) and they were tested with the Mann–Whitney U-test.
Multinomial logistic regression analysis was used to identify associations between the presence of skin diseases and categories of hs-CRP level. Adjustments were performed for following confounding factors: Sex, tobacco smoking, the use of oral contraceptives, socioeconomic status and physical activity. Results were then additionally adjusted with BMI and systemic diseases. Those with missing data were excluded from the analysis. Crude and adjusted odds ratios (OR) with 95% confidence intervals (CI) were reported as measures of association. Statistical analyses were performed using SAS software package (version 9.4, SAS Institute, Inc) and a p-value < 0.05 was considered statistically significant.
A total of 3,118 (1,497 females and 1,621 males) cohort members were invited to participate; of these 1,930 agreed and were examined and included in the analyses (the data of hs-CRP was missing in 24 subjects; the reason for missing laboratory data was that some of blood samples or their analysis were not eligible). The participation rate was 62.0 % (n = 1,930), 69% of females and 55% of males agreed to participate to the study. All study participants were 45–46 years old at the time of data collection; a slight majority were females (n = 1,036, 53.6%). The socioeconomic status and other baseline characteristics of the participants are presented in Table SI. Skin infections, eczemas and sebaceous gland diseases were the most common skin diseases, being present in 44%, 27% and 27% of subjects, respectively. The data describing the prevalence of skin diseases in this cohort have been reported in our previous study (19).
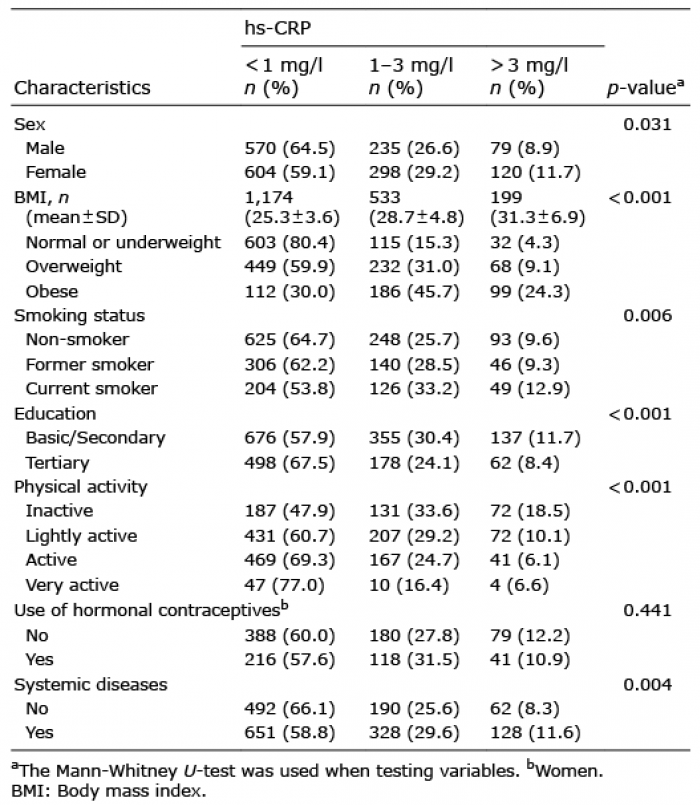
Hs-CRP data were available for all eligible (n = 1,906, n = 884 males and n = 1,022 females) participants. It was normal (< 1 mg/l) in 1,174 (61.6%), slightly elevated (1–3 mg/l) in 533 (28.0%) and highly elevated (> 3 mg/l) in 199 (10.4%) of the participants. Median hs-CRP level for females was 0.8 mg/l and 0.7 mg/l for males, (p = 0.27). (Table I and Table SI).
Table I. The association between elevated high sensitive C-reactive protein (hs-CRP) and baseline characteristics
The data of all recorded skin diseases and their associations with hs-CRP are shown in Table SII. Compared with those who had no skin diseases, hs-CRP was higher in participants with atopic eczema (p = 0.03), rosacea (p = 0.001) and onychomycosis (p = 0.01). The hs-CRP was also higher in study cases who had any skin disease that was classified as severe enough needing further evaluation or treatment, compared to those needing no further care (p = 0.016).
After adjustment for sex, tobacco smoking, the use of oral contraceptives, education and physical activity, study cases with any skin disease had a 1.8-fold greater OR for highly elevated hs-CRP levels compared with those whose skin evaluation did not result in a diagnosis. The OR was more than doubled in those who had atopic eczema when compared with those who did not have atopic eczema. The corresponding OR with rosacea was 1.7-fold higher and with onychomycosis, doubled. In participants with a skin disease requiring further treatment the OR for highly elevated hs-CRP was 1.6-fold greater than in those who did not require further treatment. (Table II).
Table II. Risk for elevated high sensitive C-reactive protein (hs-CRP) in skin disease types and in participants whose disease required further treatment
When the OR for highly elevated hs-CRP was analyzed separately in female subpopulation, those with atopic eczema (OR 2.4, 95% CI 1.1–4.9), rosacea (OR 2.0, % CI 1.3–3.3), androgenetic alopecia (OR 10.7, % CI 2.6–43.8) and tinea pedis (OR 2.0, % CI 1.2–3.3) had increased OR. In male subpopulation, the OR was increased in those with eczema staticum (OR 8.4, 95% CI 1.2–5.8) and with onychomycosis (OR 2.2, % CI 1.3–4.0).
After further adjustment for BMI and with systemic diseases, in the analyses of the whole study group, the OR for highly elevated hs-CRP in subjects with atopic eczema was 2.4-fold greater than in those without atopic eczema. The corresponding OR in those who had onychomycosis, was 1.9-fold greater when compared with those who did not have onychomycosis. If any of the sebaceous gland diseases were present, the OR for highly elevated hs-CRP was 1.4-fold higher than in its absence. Finally, if a study case had any skin disease needing further follow-up or treatment, the OR for elevated hs-CRP was 1.5-fold greater than in cases not requiring further attention (Table II).
In this study we demonstrate a previously unreported association between low grade inflammation and several skin diseases in an unselected general population sample. This association was particularly seen in patients with atopic eczema, rosacea and onychomycosis suggesting an active systemic inflammatory process in all these dermatological diseases.
Inflammation is defined as a complex biological response to a harmful stimulation of the body followed by the clinical symptoms of redness, swelling, heat and pain (23). Inflammation is also characterized by an increased blood concentration of inflammatory markers, of which CRP is the most commonly used in clinical studies, being a strong marker of non-specific inflammation (8). CRP is an acute phase protein mainly synthetized in liver cells and regulated by many cytokines (24). Many factors influence the body’s CRP level; for example, its concentration elevates slightly with age (25), and it is associated with BMI (26) and smoking (9). CRP levels also vary between racial and ethnic groups, being lowest among Caucasians (10).
Body weight has an indisputable effect on CRP levels (27) and CRP values relate to several measurements of body fat (26). Consequently, adjustment of CRP findings for BMI may mask other important drivers of CRP levels. That is the reason why we chose to adjust our results separately with BMI.
When an individual’s CRP level is only slightly elevated, their inflammation state is categorized as low grade (20), usually meaning that the inflammation displays no visible symptoms. These small CRP elevations can be measured using the hs-CRP method which is more precise than standard CRP testing. Low grade inflammation is associated with several noncommunicable diseases (2–6, 28) which together form one of the major causes for morbidity and mortality in high income countries (29).
Our study found an association between elevated hs-CRP levels and atopic eczema, rosacea and onychomycosis – diseases from various subgroups of cutaneous conditions. Previously, the association between low grade inflammation and rosacea had been reported by only two studies with limited number of participants (15, 30). A Turkish study (n = 40) demonstrated that patients with rosacea have higher levels of CRP (CRP > 0.8 mg/l) than healthy controls (15), a finding that aligns with our results. However, in the other study (n = 60) this relationship was not found (30). There is slight evidence that atopic eczema is associated with low grade inflammation: Young psychiatric patients with atopic eczema showed higher levels of inflammatory markers compared with those without eczema (16, 18). To the best of our knowledge, the association between atopic eczema and low grade inflammation, has not been previously demonstrated in an unselected adult population. Another interesting finding of our study is that cohort members with onychomycosis had elevated hs-CRP levels. This association has not been investigated previously albeit onychomycosis is so common in the general population (19, 31). Our results suggest that onychomycosis may be associated with systemic inflammation, which should be kept in mind when treating patients with fungal nail infection. However, further clinical studies in larger populations are needed to strengthen this association.
We did not detect any association between low grade inflammation and psoriasis, even though this association has been reported by many previous studies (7). It is known that CRP values in psoriasis patients correlate with PASI values (32). In our study the severity of psoriasis was mild (mean PASI 3.1, range 0.1–13.7) (19) which may have affected to results. Furthermore, the prevalence of psoriasis was quite low (p = 40) in our study which may explain the absence of statistical significance. Our results strengthens the postulate that disease severity correlates with hs-CRP level: our study cases who had skin disease in need of further care had higher hs-CRP levels than those with skin disorder not requiring treatment.
In our study, elevated hs-CRP levels (> 3 mg/l) were more common in females than males (p = 0.03). There were also more significant associations between skin diseases and elevated hs-CRP levels in females than in males. It is known that females have higher background CRP levels than males (5). This is mostly due to hormonal factors such as the use of systemic contraceptives or hormone replacement therapy (33). Furthermore, CRP levels also vary with hormonal changes during the menstrual cycle (34), which should be taken into account when interpreting our results because it is likely that many of our participants were still premenopausal.
The major strength of this study was the coverage of a wide general population (n = 1,930) with a relatively high (61%) participation rate. Further, we consider the clinical doctor-based whole-body skin investigation, rather than self-reporting, to be a significant strength. Our study population represents a normal middle-aged population; study cases with skin disease were not collected from dermatology clinics. Therefore, as opposed to similar studies, most of our participants’ skin disease was mild (7). It is noteworthy that despite the fact that the majority of our study cases had mild disease, we were nevertheless able to detect the associations with systemic inflammation. We used CRP as a marker of inflammation because it has proved to be more stable than other inflammatory markers (20) and we employed the hs-CRP method because of its ability to detect even minor inflammation. Additionally, our study cases were from a relatively ethnically homogenous population, offering stable baseline levels of hs-CRP. We were also able to survey a variety of possible confounding factors due to the unique study design, which allowed comprehensive health data collected since subjects’ birth to be taken into account.
Our study had some limitations: The phase of the menstrual cycle of female participants at the time of investigation, which may have slightly affected the results, was not recorded. Additionally, it would have been useful to have repetitive hs-CRP measurements, since so many factors (24) can easily influence the CRP value. We also admit as a limitation that NFBC1966 cohort members represent a middle-aged population and thus, our findings are not to be generalized to all age groups.
Here we provide the evidence of the association between various skin diseases and systemic low grade inflammation measured by hs-CRP testing. It is known that the presence of one inflammatory disease exacerbates the risk for others (15). Thus, patients with dermatological conditions such atopic eczema, rosacea or fungal skin infection, may carry an elevated risk for noncommunicable inflammatory diseases such as atherosclerosis, and this should be kept in mind when treating patients with cutaneous disorders.
This cross-sectional study offers evidence of the association between skin diseases and low grade inflammation but longitudinal prospective studies are needed to further investigate this relationship with specific skin diseases, with attention to risk patients of different age groups and between sex.
The study was supported by the Oulu University Hospital, the Northern Finland Cancer Association, the Academy of Finland, the Finnish Medical Foundation, the Medical Research Center Oulu, the Finnish Dermatological Society, the University of Oulu and the ERDF European Regional Development Fund – Well-being and health: Research in the Northern Finland Birth Cohort 1966 (grant no. 539/2010 A31592, 01.01.2011–31.12.2013).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize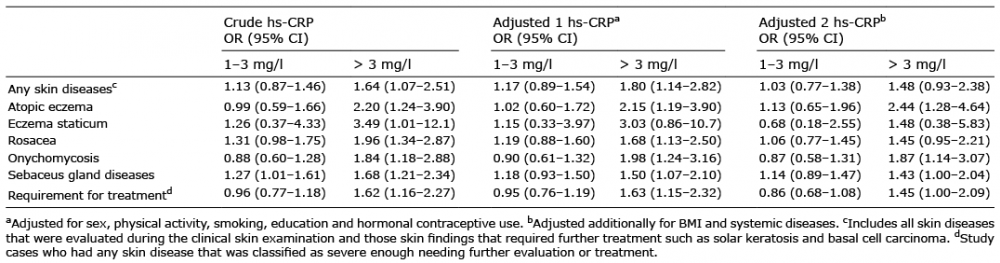 Click to show fullsize
Click to show fullsize