


1Department of Dermatology, 2Department of Ophthalmology, Soonchunhyang University Bucheon Hospital, Bucheon, 3Department of Dermatology, Soonchunhyang University Cheonan Hospital, Cheonan, and 4Department of Biostatistics, Clinical Trial Center, Soonchunhyang University Bucheon Hospital, Bucheon, Republic of Korea
Atopic dermatitis (AD) is a chronic inflammatory skin disorder. Patients with AD often experience psychological distress and poor health-related quality of life (HRQoL). The aim of this study was to investigate the association of several psychological health statuses and poor HRQoL in an adult population with AD in South Korea. A total of 37,578 adults who participated in the Korean National Health and Nutrition Examination Survey, a nationwide, population-based, cross-sectional health survey between 2008 and 2013 were included. HRQoL was assessed by EuroQoL (EQ) 5-dimension questionnaire and EQ-visual analogue scale scores. Multiple logistic regression analysis was performed to identify the association of stress, sleep duration, depressive mood, depression, suicidal ideation, and HRQoL with AD relative to matched controls. After adjusting in patients with AD confounding factors, stress, depressive mood, depression, suicidal ideation and poor HRQoL were significantly associated with AD. Dermatologists should be concerned with improving HRQoL and managing the psychological health status of adult patients with AD.
Key words: atopic dermatitis; health-related quality of life; psychological health status.
Accepted Sep 13, 2017; Epub ahead of print Sep 13, 2017
Acta Derm Venereol 2017; XX: XX–XX.
Corr: Young Lip Park, Department of Dermatology, Soonchunhyang University Bucheon Hospital, 170 Jomaru-ro, Bucheon 14584, Republic of Korea. E-mail: ylpark@schmc.ac.kr
Atopic dermatitis (AD) is a chronic inflammatory skin disorder characterized by recurrent pruritic eczematous lesions, which are often associated with other atopic manifestations such as asthma and rhinitis (1, 2). There is worldwide geographical variability in the prevalence of AD, with an incidence ranging from 1% to 20% (3). Although it appeared to plateau at 10–20% in many developed countries, the incidence continues to increase in many developing countries (2). The prevalence of AD in adults is reportedly approximately 10% according to United States (US) population-based studies (4), and ranges from 1.8% to 4.6% according to several Asian population-based studies (5–8). With an increasing prevalence in developing countries, and as one of the most common chronic diseases in developed countries, AD is currently considered a global public health concern.
However, the burden of patients with skin problems has been underestimated because dermatological diseases are usually non-fatal and thus are considered of low importance compared with other, life-threatening diseases. Even in clinics, dermatologists treating patients with AD tend to focus on improving the skin condition itself and often overlook patients’ quality of life (QoL) and other psychological concerns. Although AD is not life-threatening, it is closely related to patients’ QoL because of the irritating and disfiguring nature of the disease. In fact, skin diseases were recently demonstrated to be the fourth-most burdensome non-fatal disease according to the Global Burden of Disease Study (9). The burden includes the tremendous social and economic costs related not only to the direct cost of treatment, but also to indirect costs, such as loss of employment and productivity, and substantially reduces the health-related QoL (HRQoL) of patients with AD (10–12).
Recently, many researchers have focused on the psychological health status and HRQoL of patients with dermatological diseases; these factors have been highlighted worldwide (9, 10, 13). In many cases, AD is known to accompany many other psychological problems including stress, sleep disturbance, depression, and suicidal ideation, which are, in turn, associated with patients’ HRQoL (10, 12). Such negative impacts of AD on the psychological health and HRQoL of patients have been demonstrated previously (10, 12, 14, 15).
However, there have been few comprehensive studies investigating the associations of AD with HRQoL and psychological comorbidities using population-based study designs (8, 16, 17). In addition, previous studies have mostly included paediatric and adolescent AD patients, whereas studies focusing on adult populations have been less common (16, 18).
The aim of this study was to investigate whether various psychological health statuses, including depression, anxiety, sleep disturbance, and suicidal ideation, are associated with AD in an adult Korean population using a population-based design. In addition, the study explored the association between AD and HRQoL using the EuroQoL 5-dimension questionnaire (EQ-5D), currently the most popular preference-based instrument for measuring HRQoL and EQ-visual analogue scale (VAS) (19).
The current study was based on data from the Korean National Health and Nutrition Examination Survey (KNHANES), a nationwide, population-based, cross-sectional health survey conducted by the Korean Centers for Disease Control and Prevention, with approval from its Institutional Review Board (IRB) (approval numbers KCDC-2008-04EXP-01-C, KCDC-2009-01CON-03-2C, KCDC-2010-02-CON-21-C, KCDC-2011-02CON-06-C, KCDC-2012-01EXP-01-2C, KCDC-2013-07CON-03-4C) (20). The KNHANES adopted a multi-stage, stratified, probability-clustered sampling method based on age, sex, and geographical area. The target population of the survey was the civilian, non-institutional population of South Korea. The survey was conducted annually by trained experts, including nurses, nutritionists, and persons who majored in public health to provide statistics for establishing health-related policies in South Korea, and to research infrastructures for studies on risk factors of various diseases. The survey consisted of 4 main components: a health interview, a health behaviour survey, a health examination, and a nutrition survey.
In this study, data from KNHANES IV (2008, 2009), V (2010–2012), and VI (2013) were used to investigate the association between the presence of AD and psychological health status and HRQoL. Participants aged ≥19 years who completed questionnaires on psychological health and HRQoL were included in the study. The study design adhered to the principles outlined in the Declaration of Helsinki for research involving human subjects, and all survey participants provided written informed consent. This study was approved by the IRB of Soonchunhyang University Bucheon Hospital (approval number SCHBC 2016-12-027).
The questionnaires regarding psychological health status include sections on depressive mood, sleep duration, psychological stress, and suicidal ideation. Participants who felt sadness and despair affecting daily life for at least 2 or more continuous weeks within a recent year were categorized as having a depressive mood. Participants who were diagnosed with depression by a clinician were considered to have depression. The severity of psychological stress was classified into 4 levels: 1 (low), 2 (moderate), 3 (severe), and 4 (very severe). Sleep duration was also evaluated using the questionnaires and was classified into 4 categories: ≤ 5, 6, 7, 8, and ≥ 9 h per day. Regarding suicidal ideation, participants were asked whether they had had any thoughts of suicide during the past year.
HRQoL was evaluated with the EQ-5D, a questionnaire widely used to assess HRQoL. It consists of 5 questions assessing the level of self-reported problems with mobility (EQ-1), self-care (EQ-2), performance of usual activities (EQ-3), pain/discomfort (EQ-4), and anxiety/depression (EQ-5). One of 3 responses was selected by the participants for each question: no problems, moderate problems, and severe problems. For each EQ-5D question, subjects who reported moderate or severe problems were classified as “participants with problems”. A summary index (EQ-5D index) was calculated from the answers to all of the questions, using a formula developed by the Korean Centers for Disease Control and Prevention. For the EQ-VAS, participants chose a score between 0 (worst state of health) and 100 (best state of health) to indicate their overall HRQoL.
Demographic variables included age, sex, area of residence, income, and education level, which were acquired from the health interviews. With regard to area of residence, the 16 districts of South Korea were divided into 2 groups: (i) urban regions, including Seoul, Gyeonggi, Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan; and (ii) rural regions, including Gangwon, Chungbuk, Chungnam, Jeonnam, Jeonbuk, Gyeongbuk, Gyeongnam, and Jeju. Income status was quantified by quartile. Education level was categorized as elementary school or lower, middle-school graduate, high-school graduate, or college graduate or higher.
The other covariates analysed in this study were health-related behaviours, including smoking history and alcohol consumption. Smoking history was classified into 2 categories: ever and never. Alcohol consumption was categorized as follows: none in the past year, < once/month, once/month, 2–4 times/month, 2–3 times/week, and ≥ 4 times/week.
Statistical analyses were conducted using the Self-Assessment Survey (SAS) survey procedure (ver. 9.3; SAS Institute, Inc., Cary, NC, USA) to account for the complex sampling design and sampling weights. The demographic characteristics of the participants are presented as either means and standard error (SE) or proportions and SE. According to AD diagnosis, participants’ characteristics were compared using the Rao-Scott χ2 test (for categorical variables) and analysis of variance (for continuous variables). To assess the association between AD prevalence and psychological health status or HRQoL, multiple logistic regression analyses were performed. For the logistic regression analyses, unadjusted and adjusted models were established. The adjusted model included age, sex, monthly income, region of residency, education level, smoking status, drinking habits, and diseases that could significantly affect psychological health status and HRQoL of the participants, such as various types of cancers, chronic kidney diseases, liver cirrhosis, asthma, chronic obstructive pulmonary disease, arthritis, coronary artery diseases, and stroke. Further adjustments for psychological health status including sleep duration, psychological stress, and depressive mood were conducted when analysing the association between AD and HRQoL (adjusted Model II). The possible associations between AD and psychological health status and HRQoL are expressed as odds ratios (ORs) and 95% confidence intervals (CIs). Furthermore, the effect of sleep loss (<5 h), moderate-to-severe psychological stress, and depressive mood on HRQoL among subjects with AD was analysed. In all analyses, p-values were two-tailed, and a p < 0.05 was considered to show statistical significance.
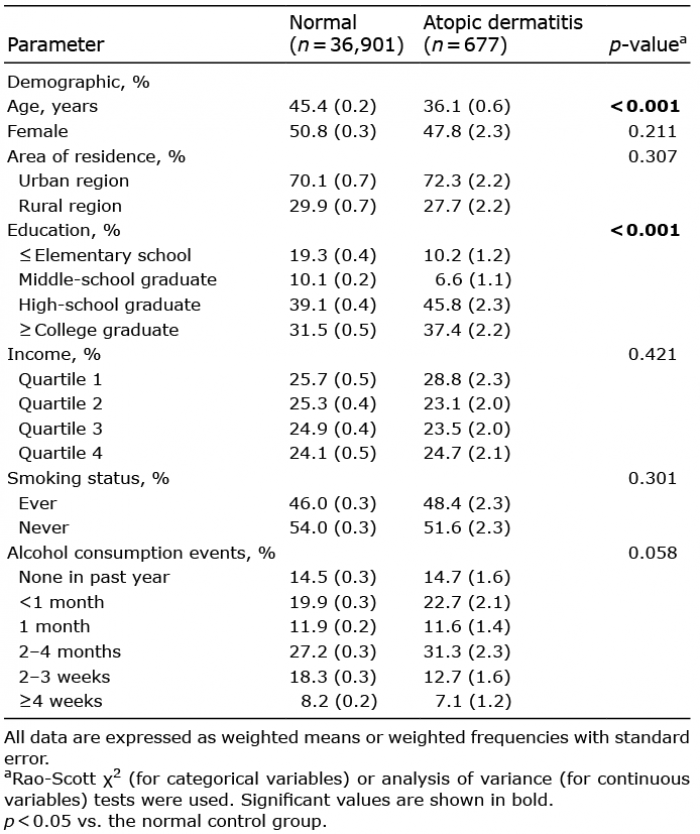
Of the 51,138 available participants, 37,578 participants aged ≥ 19 years were included in this study. Participants were further grouped into a non-AD group (n = 36,901) and an AD group (n = 677). The demographic characteristics according to AD diagnosis are shown in Table I. Subjects with AD were significantly younger (p < 0.001), and more educated (p < 0.001) compared with control participants.
Table I. Demographic characteristics of the normal and atopic dermatitis populations
Table II shows the differences in psychological health status and HRQoL scores according to AD status. Patients with AD demonstrated more severe psychological stress (p < 0.001), a higher prevalence of depressed mood and use of psychological counselling services (p = 0.001 and p = 0.001, respectively), and a higher prevalence of depression and suicidal ideation (p = 0.002 and p < 0.001, respectively) compared with non-AD subjects. Sleep duration did not differ between the 2 groups (p = 0.068). Regarding EQ-5D and EQ-VAS scores, a higher rate of some or severe pain/discomfort (EQ-4) and anxiety/depression (EQ-5) on the EQ-5D was detected in patients with vs. without AD (p = 0.003, and p < 0.001, respectively). EQ-VAS scores were significantly higher in patients with AD than in those without AD (p = 0.004).
Table II. Psychological health and health-related quality of life parameters according to atopic dermatitis (AD) status
The associations between each psychological health status component and the prevalence of AD were investigated using multivariate logistic regression analysis. After adjusting for potential confounding variables, including age, sex, monthly income, region of residency, education level, smoking status, and drinking habits, the severity of psychological stress was positively associated with AD (p for trend < 0.001) (Table III). In addition, depressed mood (OR 1.54, 95% CI 1.20–1.97, p < 0.001), prevalence of depression (OR 1.83, 95% CI 1.35–2.47, p < 0.001), suicidal ideation (OR 1.67, 95% CI 1.31–2.14, p < 0.001), and psychological counselling (OR 1.78, 95% CI 1.11–2.84, p = 0.016) were significantly associated with AD. On the other hand, there was no significant association between AD and sleep duration (p for trend = 0.070).
Table III. Odds ratios for the association between atopic dermatitis and various components of psychological health status
Table IV presents the association between the prevalence of AD and HRQoL. On multivariate analysis using tertiles of the EQ-5D index and EQ-VAS scores, the OR for AD prevalence in the third tertile compared with the lowest tertile was significantly lower for both scores (EQ-5D OR 0.53, 95% CI 0.36–0.78, p for trend < 0.001; EQ-VAS OR 0.51, 95% CI 0.34–0.78, p for trend < 0.001). When associations with each EQ-5D category were analysed, patients with AD were more likely to have some, or severe, problems with pain/discomfort (EQ-4) and anxiety/depression (EQ-5) (OR 1.79, 95% CI 1.40–2.28, p < 0.001; OR 1.66, 95% CI 1.24–2.21, p < 0.001, respectively) after adjusting for potential confounding factors (adjusted Model I). Other EQ-5D categories, including problems regarding physical activity, self-control, and daily activity, did not show any association with AD. After further adjusting for psychological health statuses, including sleep duration, psychological stress, and depressive mood (adjusted Model II), similar associations were found between AD and HRQoL parameters with adjusted Model I, with minor differences in ORs and p-values.
Table IV. Odds ratios for the prevalence of atopic dermatitis according to each component of health-related quality of life
Sleep duration, psychologically perceived stress, and depressive mood themselves may also have an effect on HRQoL in patients with AD. To evaluate such relationships, we further performed subgroup analysis using subjects with AD and examined whether sleep loss (< 5 h), perceived stress (moderate-to-severe stress), and depressive mood (≥ 2 weeks, continuously) were associated with the EQ-5D index or EQ-VAS scores on multivariate analysis. After adjusting for confounding factors, psychological stress and depressive mood showed significant associations with both scores, demonstrating decreased ORs for the third tertile compared with the lowest tertile (EQ-5D OR 0.18, 95% CI 0.10–0.32, p for trend < 0.001; EQ-VAS OR 0.29, 95% CI 0.17–0.52, p for trend < 0.001; EQ-5D OR 0.25, 95% CI 0.13–0.46, p for trend < 0.001; EQ-VAS OR 0.36, 95% CI 0.19–0.70, p for trend = 0.004, respectively). On the other hand, no significant association was found between sleep loss and HRQoL score (Table V).
Table V. Odds ratios for a sleep duration of less than 5 h, moderate-to-severe psychological stress, and depressive mood according to health-related quality of life in subjects with atopic dermatitis
This study investigated the association of AD with HRQoL and several psychological health statuses in the adult population of Korea using data obtained from the KNHANES. Psychological health status included psychological stress, depressive mood, depression, suicidal ideation, and sleep disturbance, which have all been suggested, with increasing evidence, as AD-associated psychological problems. A previous study reported a higher prevalence of depression, anxiety disorder, and suicidal ideation in patients with common skin diseases compared with a control group (10).
The prevalence of AD in adult populations was estimated to be 1.8% in this study, which was lower than that reported in most previous studies from developed countries. Since we defined the AD group as subjects currently suffering from this condition, patients who were previously diagnosed with AD but were in full remission or asymptomatic at the time of the surveys may not have been included in the AD group. These differences in AD definition may have led to the discordance in AD prevalence compared with previous reports.
The results of this study showed that adults with AD had more severe psychological stress, a higher rate of depressive mood and psychological counselling, and a higher prevalence of depression and suicidal ideation compared with non-AD adults. Most of the associations between these psychological health statuses and AD remained significant after adjusting for potential confounding factors, including age, sex, socioeconomic status, smoking status, and drinking habits. On the other hand, sleep duration, a key factor related to sleep disturbance, was not significantly associated with AD. In addition, HRQoL in adults with AD measured by the EQ-5D and EQ-VAS was significantly impaired compared with that of non-AD adults, particularly in the subcategories of pain/discomfort (EQ-4) and anxiety/depression (EQ-5)
Many studies have demonstrated a relationship between psychological stress and AD. AD and psychological stress are known to be reciprocally related and appear to form a vicious cycle (21, 22). Pruritus, a major symptom of AD, has been reported to be an important factor contributing to this vicious cycle in individuals with psychological stress (21). From previously published papers, we can infer that intense pruritus, cosmetic disfigurement, and sleep loss may impose tremendous stress on patients with AD and their social relationships while; stress may also exacerbate AD skin lesions (8, 12, 21, 23–25).
Although the mechanism by which stress affects AD remains unclear, many studies have suggested a possible link. Most of those studies demonstrated that stress stimulates the hypothalamic-pituitary-adrenal axis to induce a shift toward a T-helper type 2 (Th2) cell phenotype, which releases neuropeptides and neurotrophins, including pro-allergic cytokines such as interleukin (IL)-4 and IL-5 (23, 25). In addition, increased stress-induced endogenous glucocorticoids also disrupt the cohesion of the stratum corneum and impair epidermal antimicrobial functions, which may play a crucial role in aggravating AD skin lesions (12).
The results of this study are in agreement with the results of several previous reports (8, 26), showing that psychological stress is significantly associated with AD in adults.
An increasing body of evidence has underlined the association between AD and depression, and it is now widely known that patients with AD (both children and adults) are more likely to be depressed compared with those without AD (10, 12, 15, 27–29). Another study reported that depression and anxiety were the most common psychological problems that co-occur with AD. In this study, participants diagnosed with depression by a clinician were categorized as having depression. Regarding depressive mood, participants who felt sadness and despair affecting daily life for at least 2 or more continuous weeks within a recent year were categorized as having a depressive mood. The same questionnaire was used for screening depressive mood in the Korean version of the World Health Organization (WHO); namely, the Composite International Diagnostic Interview-Short Form, which was validated as a cost-effective screening instrument that could easily be applied to health surveys (30, 31). In agreement with previous investigations, our study demonstrated that adult patients with AD are more likely to experience depression or a depressed mood compared with controls after adjusting for possible confounding factors.
Intense pruritus, together with high rates of sleep disturbance (17) and increased healthcare costs (11, 32), may contribute toward higher rates of depression among patients with AD. From a clinical perspective, the suffering induced by pruritus, together with the social stigma of perceiving oneself as being disfigured (due to chronic eczematous skin lesions) may, in particular, impose a great psychological burden, especially in adolescents and young adults with AD.
Although the exact relationship between AD and depression has not been proven clearly, the link is likely to be bidirectional (29). That is, AD increases the risk of depression (27, 28, 33), whereas depressive symptoms may also trigger the development or aggravation of AD (21). One study demonstrated that an elevated level of central corticotrophin-releasing factor is often detected in depressed patients, which might decrease the threshold for itching, the major symptom of AD (34). In addition, stress-induced depression may also alter the immunological responses of patients with AD (35). Future studies are needed to further clarify the possible mechanism by which AD and depression are associated.
It has been demonstrated that psychological distress and low self-esteem, due to the difficulties associated with AD, increase the risk of suicidal behaviour in adolescents (36). Noh et al. (37), using data from a nationally representative sample of Korean adolescents, also found that AD was associated with an increased risk of suicidal behaviour in the 7th to 12th grade of school. However, there are fewer studies demonstrating such a relationship in adults with AD. Arima et al. (38) reported a higher prevalence of suicidal ideation among adults with AD (16.5% vs. 10.2% in non-AD adults (38)), and Kimata (39) also reported a high prevalence of suicidal ideation among patients with AD aged 15–49 years. In this study, suicidal ideation was assessed by the participant’s positive answer to the question, “In the last 12 months, did you think about committing suicide?” Considering that there are no validated items for studying suicidal ideation, the questionnaire used in this study is a relatively well-documented predictor of suicidal attempts, and has been used in many previous surveys (10, 40–43). The increased OR for suicidal ideation in adults with AD shown in this study is consistent with previous reports.
It is noteworthy that several cases of patients with skin diseases having either attempted or completed suicide have been reported by dermatologists (13, 44), and even patients with AD with mild symptoms were reported to experience suicidal ideation (39). Understanding the role of medical conditions in suicidal ideation is complex (45), but several hypotheses have been suggested to explain the relationship between AD and the risk of suicidal behaviour (37). Above all, a depressive mood caused by cosmetic disfigurement and changes in body image was frequently reported to be associated with suicidal ideation, although other psychological problems, such as stress and sleep difficulties, also need to be considered (33, 37, 38). It was also suggested that the intrinsic characteristic of the disease itself, which often shows a chronic, recurrent course despite repeated treatment, often makes patients with AD feel hopeless and leads to suicidal ideation even though such patients have no accompanying psychiatric illness (39).
In clinics, patients with AD frequently complain of difficulty falling asleep and repeated episodes of awakening during sleep because of severe pruritus. However, sleep disturbances in patients with AD are often underdiagnosed by clinicians, as demonstrated recently in a US population-based study of adults with AD (46). In fact, patients with eczema slept less, and awoke more often, which lowered overall sleep efficiency (47). Previous studies have demonstrated an association between skin eczema and sleep disturbance in patients with AD, reporting that the sleep disturbance may result in func-tional impairment of patients with AD causing daytime fatigue, irritability, and cognitive difficulties (46–48). Besides pruritus, changes in the circadian rhythm of the skin, as well as melatonin and cytokine dysregulation, in AD patients have recently been suggested as factors contributing to sleep disturbance (49–51).
There is some controversy with regard to sleep duration. In a US population study, adults with AD had higher odds of short sleep duration compared with non-AD adults (46). On the other hand, another study demonstrated that both short and long durations of sleep were associated with AD, despite the popular belief that AD only affects loss of sleep duration (17). Poor sleep quality, excessive fatigue, and the use of sedating antihistamines are assumed to be associated with sleepiness, which increases mean sleep duration (17).
In this study, the percentage of adults with AD who slept both more than 9 h, and less than 5 h, was slightly higher compared with non-AD adults, but the findings did not show statistical significance when adjusted for confounding factors.
Regardless of sleep duration, sleep quality is well known to be impaired in patients with AD (15, 17, 46). This indicates that sleep quality cannot be fully assessed by sleep duration alone, and thus should also be assessed according to other factors, including sleep latency, night-time awakenings, subjective sleep quality, and the use of sleeping medication. Further studies are needed to demonstrate more comprehensively the mechanism by which sleep disturbances and AD are associated.
In patients with chronic dermatological diseases, the measurement of HRQoL has drawn a lot of attention recently. Dermatologists have made an effort to evaluate the QoL of patients with AD using various methods, and many previously published articles demonstrated that patients with AD experienced severe impairment in their QoL and emotional well-being compared with the healthy general population (18, 52–55).
It is unsurprising that AD has a great impact on HRQoL because of the chronic clinical course of the disease. Since it has no definitive cure, patients with AD suffer not only from the symptoms caused by the disease itself, but also from a high and life-long psychosocial and economic burden (9, 10, 14).
Since HRQoL indexes both QoL directly related to the disease itself and QoL that is independent of, but possibly affected by, the disease (56), the burden of illness, outcomes of related medical treatments, and functional impairment in completing daily tasks are well-known factors affecting HRQoL (56, 57). HRQoL can be assessed generally by 3 types of instrument: generic, dermatology-specific, and disease-specific questionnaires (58). In many dermatological investigations, the Dermatology Life Quality Index (DLQI), Dermatology QoL Scales, and Skindex-29 are used to assess QoL. More specifically for AD, the QoL Index for AD (QoLIAD) is known to offer better validity (59). However, there is no definite consensual instrument for measuring HRQoL in adult AD with a high degree of validity and reliability.
EQ-5D and EQ-VAS are widely used preference-based generic measures of HRQoL; thus, the results should be carefully interpreted because of their socially and culturally dependent characteristics. We used the Korean-specific preference weight to generate EQ-5D index scores (60). The EQ-5D index used in this study has been translated into Korean, and its validity and test–retest reliability have been previously demonstrated (61).
Most previous studies investigated the HRQoL of AD with the DLQI, usually focusing on skin problems; this limited comparisons with respect to HRQoL, since the questions may not be relevant to those without skin problems (18). Thus, EQ-5D and EQ-VAS as generic instruments (rather than DLQI) have strengths for comparing AD patients with those without AD with moderate validity and reliability (14, 52). There have also been nationwide studies presenting HRQoL in patients with AD using the EQ-5D index (62, 63) and EQ-VAS (16, 62–64). Although the validity of EQ-5D and EQ-VAS as measurements of HRQoL in AD patients remain limited, they have strengths in nationwide studies for detecting general changes in different aspects of the patient’s HRQoL, further aiding public healthcare decision-making.
In the present study, a significantly poor HRQoL in adults with AD was observed; these patients also experienced more severe pain/discomfort and anxiety/depression. Intractable itching can be assumed to be a major factor contributing to physical discomfort and excessive excoriations and crusts on damaged skin, which may trigger further pain in patients with AD. Regarding anxiety/depression, previously reported data demonstrated that adults with AD were more anxious and depressed compared with non-AD adults (65, 66); this is in line with the results of the present study.
Furthermore, we found that patients with AD suffering from severe stress and depression had lower EQ-5D index and EQ-VAS scores compared with AD patients without those psychological problems. These findings indicate that psychological stress and depression may further negatively affect the HRQoL of adults with AD. Therefore, dermatologists should consider and manage these aspects comprehensively when treating patients with AD.
The present study had several strengths. First, it was based on data taken from a nationwide survey that included a large population sample; this may minimize selection bias. Secondly, the participants included in this study comprised an adult population. Considering the chronic nature and relapsing course of AD, the characteristics of adults with AD may better reflect the long-term effects of AD on HRQoL and psychological health status than those of paediatric patients.
However, there were also a number of limitations that should be considered. First, because of the cross-sectional nature of the study, causal relationships between AD and psychological health status or HRQoL could not be defined. Secondly, we included potential confounders, but it is possible that other, unidentified factors may also contribute toward these associations. Thirdly, it should be noted that, since KNHANES was designed for investigating the overall public health status of the general population, the questionnaires were quite simple and short, thereby restricting the full and detailed evaluation of each aspect of psychological health statuses. Moreover, since data collection relied mostly on self-reporting, the validity and reliability of several measurements used in the survey were limited, leading to potential miscategorization of the participants. Fourthly, since the KNHANES does not provide information on the disease severity of patients with AD, we were unable to evaluate the association between disease severity and HRQoL.
Nonetheless, this study comprehensively demonstrated the association between AD and psychological health status, as well as overall and individual components of the HRQoL. These data confirm and expand previous findings demonstrating an association between AD, various psychological health statuses and poor HRQoL. Based on such information, it is important to treat and manage patients with AD, since morbidity rather than mortality is the primary concern in the disease, similar to other dermatological diseases that are not life-threatening, but are chronic in nature (14, 53). In clinics, dermatologists should focus more on long-term strategies to improve HRQoL, as well as on managing psychological factors, especially psychological stress and depression, in adult patients with AD.
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea Government (Ministry of Education) (No. 2017R1D1A1B03029944) and by the Soonchunhyang University Research Fund.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize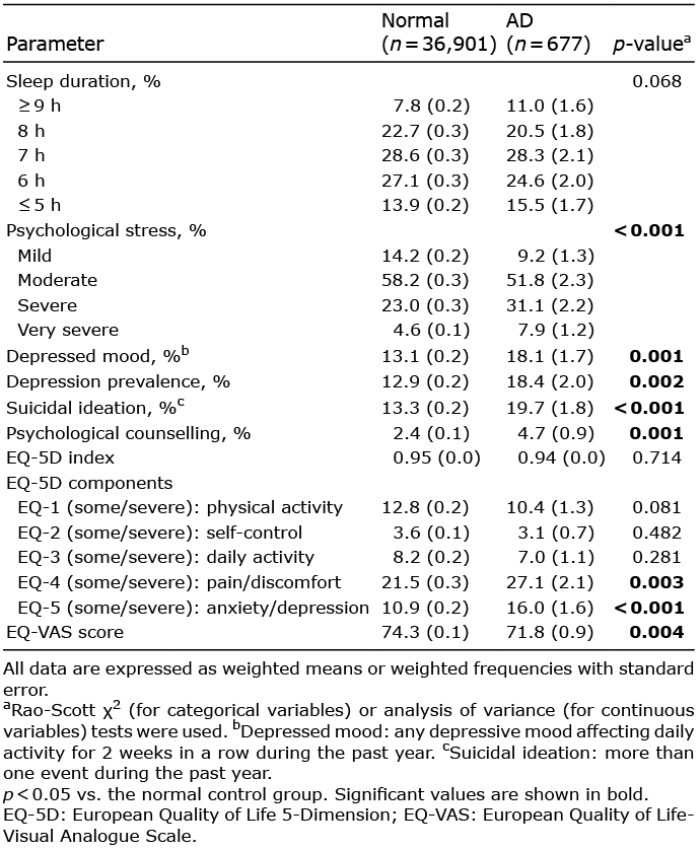 Click to show fullsize
Click to show fullsize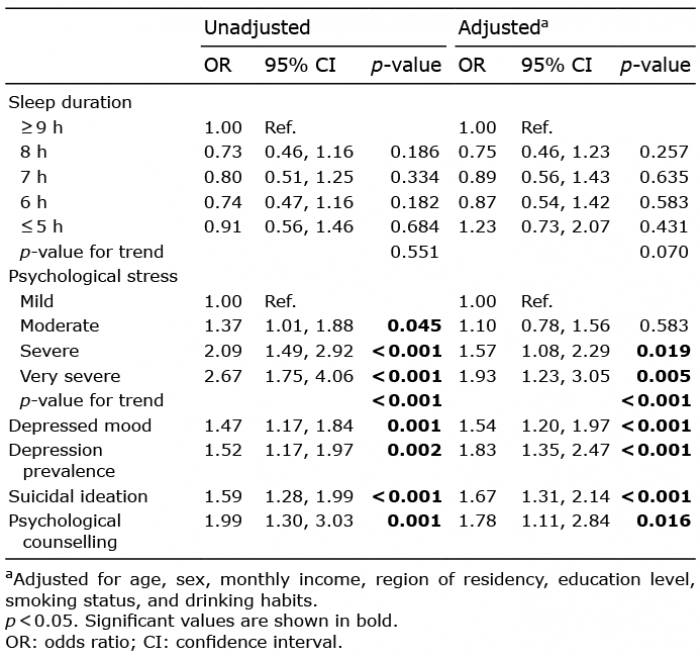 Click to show fullsize
Click to show fullsize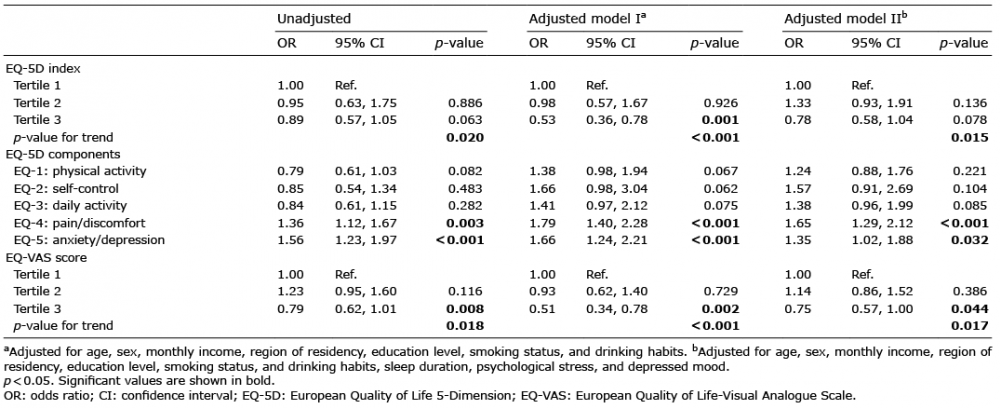 Click to show fullsize
Click to show fullsize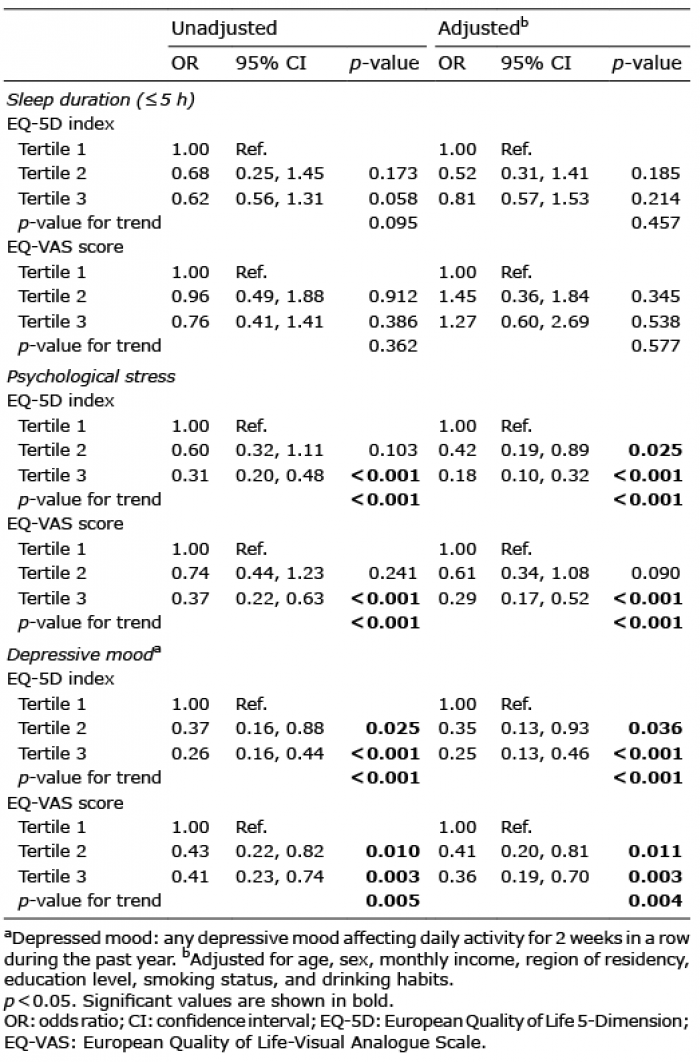 Click to show fullsize
Click to show fullsize