


1Beth Israel Deaconess Hospital and Harvard Medical School, Boston, USA, 2Department of Dermatology, University of Muenster, Muenster, Germany, 3Department of Dermatology, New York Medical College, Valhalla, USA, 4Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona, Barcelona, Spain, 5Goethe University, Frankfurt, Germany, 6Eli Lilly and Company, Indianapolis, 7Winkle College of Pharmacy, University of Cincinnati, Cincinnati, 8Department of Dermatology, University of Miami Miller School Of Medicine, Miami, USA
Itching is a prevalent plaque psoriasis symptom. Ixekizumab, an IL-17A antagonist, has demonstrated rapid, significant improvements in itch severity over 12 weeks in Phase III psoriasis trials (UNCOVER-1, UNCOVER-2). We assessed the long-term (through 60 weeks) effect of ixekizumab maintenance therapy (80-mg ixekizumab every 4 weeks [IXEQ4W]) on itch severity, using the Itch Numeric Rating Scale, in psoriasis patients who received ixekizumab, placebo, or etanercept for 12 weeks in the Phase III UNCOVER-3 trial. After 12 weeks, patients either continued or switched to IXEQ4W. Mean improvements in itch severity achieved with 12 weeks of ixekizumab (–4.7 to –5.1) were maintained through 60 weeks with IXEQ4W (–4.9 to –5.0). Patients who initially received placebo or etanercept experienced rapid itch severity improvements after switching to ixekizumab at Week 12 (Week 12, placebo: –0.6; etanercept: –3.8; Week 60, placebo/IXEQ4W: –4.9; etanercept/IXEQ4W: –4.7). Ixekizumab maintenance therapy sustained improvements in itch severity through 60 weeks.
Key words: itch; itch NRS; ixekizumab; psoriasis; maintenance;
long-term outcomes.
Accepted Sep 19, 2017; Epub ahead of print Sep 20, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Alexa B. Kimball, MD, MPH, Beth Israel Deaconess Hospital and Harvard Medical School, 375 Longwood Ave, Boston, MA 02215, USA. E-mail: kimballmdresearch@gmail.com
Psoriasis is associated with symptoms such as itching and skin pain, which can have a negative impact on health-related quality of life (HRQoL) and functional status (1–3). Itching (pruritus) is a prevalent plaque psoriasis symptom, affecting more than 60% of patients. Many patients complain that itch is their most troubling psoriasis symptom (4). Itching is frequently associated with embarrassment and impairment of sleep, mood, concentration, appetite, and sexual desire in psoriasis patients (5, 6).
Although itching is an important aspect of HRQoL in psoriasis patients, the long-term management of itch has not been well studied. Furthermore, instruments that evaluate treatment efficacy in psoriasis clinical trials, such as the Psoriasis Area and Severity Index (PASI) (7, 8), do not measure itch severity. Indeed, itch severity is not directly correlated with PASI-measured disease activity (9). Itch appears to be a domain independent from disease severity and a mediator between improvements in PASI and patient-reported HRQoL (10). To evaluate psoriasis-related itch severity in a clinical setting, the Itch Numeric Rating Scale (Itch NRS) was developed and validated as a single-item, patient-reported outcome (PRO) measure (11, 12).
Ixekizumab, a high-affinity monoclonal antibody that selectively targets IL-17A (13), was recently evaluated as a psoriasis therapy in Phase III clinical trials (UNCOVER-1, UNCOVER-2, and UNCOVER-3) and demonstrated significantly greater and clinically meaningful improvements in itch severity compared to placebo and etanercept as early as Week 1; these improvements were maintained through Week 12 (14–17).
This report describes the impact of long-term ixekizumab maintenance therapy on itch severity through 60 weeks using data from the long-term extension (LTE) period of the Phase III UNCOVER-3 trial.
UNCOVER-3 (NCT01646177) was a Phase III randomized clinical trial that evaluated ixekizumab versus placebo and etanercept in moderate-to-severe psoriasis patients (14, 15). The trial was conducted in accordance with the Declaration of Helsinki. All study sites received institutional review board approval and all patients provided written informed consent. At baseline (Week 0), patients were ≥ 18 years old with a confirmed chronic (≥ 6 months) plaque psoriasis diagnosis, ≥ 10% body surface area involvement, a Static Physician’s Global Assessment (sPGA) score ≥ 3, and a PASI score ≥ 12. Complete inclusion/exclusion criteria and detailed methodology of the initial 12-week treatment period has been described elsewhere (15). Briefly, patients were randomized 2:2:2:1 to receive one of the following 4 treatments during the initial 12-week treatment period: a 160-mg ixekizumab starting dose followed by 80 mg every 2 weeks (IXEQ2W), a 160-mg ixekizumab starting dose followed by 80 mg every 4 weeks (IXEQ4W), etanercept 50 mg twice weekly, or placebo.
At Week 12, patients entered the trial’s LTE, during which they received open-label IXEQ4W through Week 264 regardless of their treatment group before Week 12. Patients who initially received placebo were administered a 160-mg ixekizumab starting dose at Week 12 and IXEQ4W thereafter. Patients who initially received etanercept underwent a 4-week washout period before beginning ixekizumab treatment at Week 16.
Patients reported their recollection of their itch severity over the past 24 h with the Itch NRS instrument during study visits every 4 weeks through the LTE. Here we present data through Week 60 of the LTE.
The Itch NRS is a single-item PRO questionnaire that was administered at baseline and throughout the induction and LTE. At each site visit, patients self-reported itch severity using the Itch NRS by circling the integer that best described the worst level of itching due to psoriasis in the past 24 h on an 11-point numeric rating scale anchored at 0, representing “no itching,” and 10, representing “worst itch imaginable” (11). The minimal clinically important difference (MCID) was defined as a 4-point change from baseline in Itch NRS. The MCID was based on previous analyses that used anchor-based methods and was confirmed with distribution-based methods (12).
Treatment effects on change from baseline in Itch NRS scores and the proportions of patients who achieved an Itch NRS score=0 (“no itching”) and who achieved the MCID in Itch NRS score (among patients with an Itch NRS score ≥ 4 at baseline) were evaluated at each postbaseline visit using analysis of covariance (ANCOVA), including baseline score and pooled center, and Cochran-Mantel-Haenszel (CMH) test stratified by pooled center, respectively. When the ANCOVA model and CMH test were used, missing data were imputed using the last observation carried forward approach and non-responder imputation, respectively.
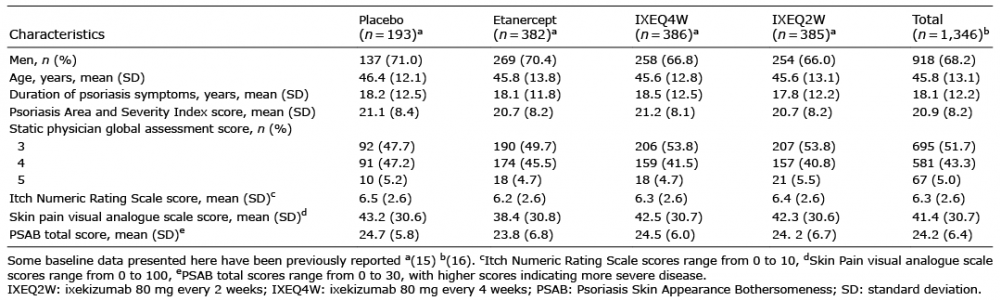
Selected patient demographic and baseline data are summarized in Table I. Patients enrolled in the UNCOVER-3 trial were mostly men, with a mean age of 45.8 years, and mean psoriasis duration of 18.1 years. Baseline clinical values (eg, PASI, sPGA, Itch NRS, Skin Pain visual analogue scale, and Psoriasis Skin Appearance Bothersomeness) were balanced between treatment arms. Additional details on patient demographics are described elsewhere (15, 16).
Table I. UNCOVER-3 patient demographics and baseline characteristics
Significant improvements in itch severity, as measured by reductions in Itch NRS scores from baseline, were observed through 60 weeks of ixekizumab treatment (Fig. 1). During the 12-week induction, statistically significant improvements in itch severity were reached as early as Week 1 among patients who received ixekizumab (least squares [LS] mean ± standard error [SE], IXEQ4W: –2.4 ± 0.1; IXEQ2W:–2.6 ± 0.1) versus placebo (–0.5 ± 0.2) and etanercept (–1.0 ± 0.1) (all comparisons, p < 0.001) (16). Significant improvements with ixekizumab versus placebo and etanercept were also reported at each subsequent visit, including Week 12 (LS mean ± SE, IXEQ4W: –4.7 ± 0.2; IXEQ2W: –5.1 ± 0.2; placebo: –0.6 ± 0.2; etanercept: –3.8 ± 0.2) (all comparisons p < 0.001) (15, 15). Itch severity improvements observed in both ixekizumab treatment groups at Week 12 were consistently maintained through the LTE (Week 12 to Week 60) after continuing or switching to the IXEQ4W maintenance dose (Fig. 1).
Fig. 1. Change from baseline in mean Itch Numeric Rating Scale (NRS) severity scores through week 60 in the UNCOVER-3 trial. Itch NRS score ranged between 0 (“no itching”) to 10 (“worst itch imaginable”). ETN: etanercept; IXEQ2W: ixekizumab 80 mg every 2 weeks; IXEQ4W: ixekizumab 80 mg every 4 weeks; LOCF: last observation carried forward; LSM: least squares mean; PBO: placebo; Nx: number of patients without missing values.
Patients who received placebo in the 12-week induction experienced rapid and significant improvements from baseline (and from Week 12) in Itch NRS score after switching to the IXEQ4W maintenance dose after Week 12 (p < 0.001; Fig. 1).
Patients who received etanercept in the 12-week induction continued to experience significant improvements from baseline in Itch NRS score after switching to the IXEQ4W maintenance dose after Week 12 (p < 0.001; Fig. 1). Following the switch to ixekizumab at Week 12, there was a slight worsening in mean Itch NRS score at Week 16 (likely an effect of the 4-week washout period), after which improvements were again evident at Week 20.
At baseline, 2.0% of all patients (range across treatment groups: 1.0% to 2.6%) reported Itch NRS scores = 0 (“no itching”). Many patients who received IXEQ4W or IXEQ2W during the induction period achieved Itch NRS scores = 0 by 12 weeks (39.4% and 45.2%, respectively). During the LTE, even more patients who remained on ixekizumab achieved Itch NRS scores = 0 with up to 60 weeks of treatment (48.2% and 47.8%, respectively) (Fig. 2).
Fig. 2. Percentage of patients (among those with an Itch Numeric Rating Scale (NRS) score >0 at baseline) who achieved Itch NRS scores = 0 (“no itching”) through Week 60 in the UNCOVER-3 trial. ETN: etanercept; IXEQ2W: ixekizumab 80 mg every 2 weeks; IXEQ4W: ixekizumab 80 mg every 4 weeks; NRI: nonresponder imputation; PBO: placebo, Nx: number of patients without missing values.
Only 5.2% of patients who received placebo in the induction period achieved Itch NRS scores = 0 by 12 weeks; however, after switching to ixekizumab in the LTE, 27.5% of these patients had achieved a score = 0 by 16 weeks, and 45.1% achieved a score = 0 by 60 weeks (Fig. 2). Among patients who received etanercept in the induction period, 21.5% achieved Itch NRS scores = 0 by 12 weeks. After switching to ixekizumab in the LTE, 33.0% of these patients had achieved a score = 0 by 20 weeks, and 45.3% achieved a score = 0 by 60 weeks (Fig. 2).
Among patients who achieved an Itch NRS score = 0 while receiving IXEQ4W during the LTE, 99.5% achieved at least 75% improvement on the PASI (PASI 75), 95.9% achieved at least 90% improvement on the PASI (PASI 90), and 81.3% achieved 100% improvement on the PASI (PASI 100) responses at Week 60. By comparison, of those with itch NRS > 0 at Week 60, 73.9% achieved PASI 75, 59.9% achieved PASI 90, and 32.5% achieved PASI 100 (for all comparisons of NRS scores = 0 vs. NRS scores > 0, p < 0.001). PASI response rates were similar between groups who received ixekizumab in the induction period and those who were switched to ixekizumab for the LTE.
The MCID on the Itch NRS (among patients with a baseline Itch NRS score ≥ 4) was achieved as early as Week 1 among a significantly higher percentage of ixekizumab-treated patients (IXEQ4W: 38.0%; IXEQ2W: 41.3%) than placebo- and etanercept-treated patients (7.0% and 14.1%, respectively) (all comparisons, p < 0.001) (15). Significantly higher percentages of ixekizumab-treated patients than placebo- and etanercept-treated patients continued to achieve the MCID at each subsequent visit, including Week 12 (IXEQ4W: 79.9%; IXEQ2W: 82.5%; placebo: 20.9%; etanercept: 64.1%) (all comparisons, p < 0.001) (15). Among patients who received ixekizumab during the 12-week induction, the percentage who achieved the MCID on the Itch NRS at Week 12 was sustained through the LTE after continuing or switching to the IXEQ4W maintenance dose (Fig. 3).
Fig. 3. Percentage of patients (among patients with an Itch Numeric Rating Scale (NRS) score ≥4 at baseline) who achieved the MCID on the Itch NRS (improvement from baseline Itch NRS score ≥4) through Week 60 in the UNCOVER-3 trial. Week 1 and Week 12 data points have been previously reported by Griffiths et al. (15) ETN: etanercept; IXEQ2W: ixekizumab 80 mg every 2 weeks; IXEQ4W: ixekizumab 80 mg every 4 weeks; MCID: minimal clinically important difference; N: number of patients in the analysis population; NRI: nonresponder imputation; PBO: placebo; Nx: number of patients without missing values.
Among patients who received placebo in the 12-week induction, there was a rapid increase in the percentage of patients who achieved the MCID on the Itch NRS after switching to the IXEQ4W maintenance dose (Fig. 3).
Among patients who received etanercept in the 12-week induction, following the switch to ixekizumab at Week 12, there was a slight worsening in the percentage of patients who achieved the MCID on the Itch NRS at Week 16, after which an increase was evident at Week 20 (Fig. 3).
Itch has been identified as a substantially problematic symptom for psoriasis patients. This LTE maintenance study demonstrates that patients who achieve significant and clinically meaningful improvements in itch severity (measured by the Itch NRS) generally experience them early in their clinical course and can maintain these improvements through at least 60 weeks with ixekizumab maintenance therapy administered every 4 weeks. This is one of the longest published follow-up studies of chronic itch in any disease and supports the long-term antipruritic efficacy of ixekizumab.
In the UNCOVER-3 trial, patients who initially received placebo during the 12-week induction period experienced rapid and significant improvements in itch severity as early as the first visit (Week 16) after being switched to ixekizumab. This rapid improvement is consistent with the effect observed in patients who received ixekizumab during the 12-week induction and these improvements were maintained through Week 60. Those patients who received etanercept during the 12-week induction experienced additional significant improvements after being switched to ixekizumab; these improvements were evident within 2 visits (8 weeks) after switching to ixekizumab and were maintained through Week 60. Notably, following the switch from etanercept to ixekizumab at Week 12, there was a slight worsening in mean Itch NRS score at Week 16. This worsening may be attributed to the 4-week washout period.
A substantial proportion (42.3%) of patients who received ixekizumab in the induction period achieved an Itch NRS score = 0 (“no itching”) within 12 weeks; this outcome was maintained throughout the LTE, with 48.0% of patients experiencing “no itching” by Week 60. While this symptom relief is highly promising, it also suggests that itch can remain a persistent problem for some patients despite treatment with highly effective therapy. Notably, in an integrated analysis of two Phase III ixekizumab clinical trials (UNCOVER-1 and UNCOVER-2) 63.8% of patients with complete skin clearance at Week 12 (i.e., PASI 100) also reported no itching (i.e., Itch NRS = 0) (18). In the integrated analysis as well as the present study, the extent and location of itch was not qualified. It is possible that some patients presented itch secondary to dry skin, atopic dermatitis, or tinea cruris. Though it should also be considered that scalp itch might be related to nearly subclinical psoriasis in some patients, which may be disregarded in the PASI 100 evaluation. Normal appearing skin previously affected by psoriasis has gene expression patterns that are not the same as unaffected skin, which suggests that subclinical factors may be active despite the unaffected appearance (19). Further research is necessary to better understand why some patients with complete skin clearance may still experience itch.
A similar pattern was observed among patients with baseline Itch NRS scores ≥ 4 who achieved the MCID on the Itch NRS. A relatively high percentage of patients (74.7%) who received placebo during induction achieved the MCID as early as the first visit (Week 16) after being switched to ixekizumab, which was consistent with the effect among those who received ixekizumab during induction. Also, among patients who had initially received etanercept, there was a slight worsening in the percentage who achieved the MCID in Itch NRS after the 4-week washout period, and this percentage increased within 2 weeks after switching to ixekizumab.
The internal validity of the results among patients initially treated with ixekizumab is reinforced by the results among patients initially treated with placebo or etanercept. For instance, patients treated with placebo who switched to ixekizumab at Week 12 experienced improvements that were consistent with patients who initiated ixekizumab treatment at earlier time points. Additionally, 27.5% of patients who switched from placebo to ixekizumab at Week 12 experienced “no itching” by their first visit (Week 16) after switching, and 45.1% of these patients experienced “no itching” by Week 60. Similar results were found in the etanercept group, where 21.5% of patients treated with etanercept during the induction period also experienced “no itching” at Week 12; after switching to ixekizumab, 45.3% of these patients experienced “no itching” by Week 60.
This long-term maintenance study demonstrates that the 12-week improvements in psoriasis itch severity achieved with ixekizumab can be consistently sustained throughout at least 60 weeks with ixekizumab maintenance therapy (IXEQ4W). Nearly half of all patients who received ixekizumab maintenance treatment experienced “no itching” throughout the study period. Whether these improvements are due to an effect specific to IL-17 inhibition or directly to overall disease improvement is worth further exploration. Of note, these patient-reported results from a clinical trial may not be representative of real-world patient experiences; however, the long-term results (after Week 12) were observed during an open-label study extension, and thus may be reasonably consistent with expected real-world outcomes in clinical practice. Notably, the long-term improvements in psoriasis itch severity reported here are consistent with the long-term improvements in psoriasis severity reported in an integrated analysis of two other Phase III clinical trials (UNCOVER-1 and UNCOVER-2) (14). In the integrated analysis, Gordon et al. (14) reported that high percentages of patients achieved marked improvements in psoriasis severity by Week 12 (as measured by proportion of patients achieving sPGA 0 or 1, PASI 75, PASI 90, and PASI 100), which were sustained through Week 60.
It should be considered that ixekizumab maintenance therapy was open-label, and thus the potential for bias exists. Also, simple imputation methods like the last observation carried forward (LOCF) and nonresponder imputation (NRI) tend to underestimate the treatment effect, and the validity of the imputation method depends on the underlying missing mechanism.
In conclusion, this study’s findings suggest that use of PRO instruments, such as the Itch NRS, to evaluate itch severity is appropriate in the clinical setting to ensure that psoriasis treatments address this most bothersome of patients’ symptoms. In addition to improvement in clinical outcomes (PASI, sPGA) and HRQoL (14), ixekizumab treatment is associated with rapid, significant, and clinically relevant improvements in itch severity. The rapid and significant resolution of itch symptoms is likely to positively impact patient satisfaction with treatment, and hence treatment adherence and persistence.
Funding for this study was provided by Eli Lilly and Company. The authors thank Cynthia Bush, ELS, and Kelly Guerrettaz of inVentiv Health Clinical for assistance with editing and manuscript preparation.
Conflicts of interest: ABK has consulting/research relationships with SUN Pharma, UCB, AbbVie, Bristol Myers Squibb Co., Dermira, Janssen, Eli Lilly and Company, and Novartis. She has been an investigator for AbbVie and Janssen. TL conducted clinical trials or received honoraria for serving as a member of the Scientific Advisory Board of AbbVie, Biogen-IDEC, Celgene, CERIES, Galderma, Eli Lilly and Company, Janssen-Cilag, La Roche Posay, Maruho, Meda, MSD, Mundipharma, Novartis, Pfizer, Sandoz, Sanofi-Aventis, Symrise, and Wolff. AG has current consulting agreements, advisory board agreements, and/or research/educational grants with Janssen Inc.; Celgene Corp., Bristol Myers Squibb Co., Beiersdorf, Inc., Abbvie, UCB, Novartis, Incyte, Pfizer, Lilly, Xenoport, Development Crescendo Bioscience, Aclaris, Amicus, Reddy Labs, Valeant, Dermira, Allergan, CSL Behring, Merck, Sun Pharmaceutical Industries. LP has received consulting fees, speaking fees and/or honoraria from AbbVie, Almirall, Amgen, Baxalta, Biogen, Boehringer Ingelheim, Celgene, Gebro, Janssen, Leo-Pharma, Eli Lilly and Company, Merck-Serono, MSD, Novartis, Pfizer, Regeneron, Roche, and Sandoz. His institution has received research funding in relationship with the treatment of psoriasis from AbbVie, Amgen, Janssen, Eli Lilly and Company, Novartis, and Pfizer. RK conducted clinical trials or received honoraria for serving as a member of the Scientific Advisory Board of AbbVie, Allmirall-Hermal, Merz, Amgen, Biogen Idec, BMS, Boehringer-Ingelheim, Celgene, GSK, Eli Lilly and Company, Galderma, Hexal, Janssen, LEO-Pharma, Medac, Merck Serono, Mitsubishi, MSD, Novartis, Pfizer, Tigercat Pharma, Regeneron, Roche Pharma, Sandoz Biopharmaceuticals, Schering-Plough, Icon, und UCB Pharma. RB and C-YL are full-time employees and stockholders of Eli Lilly and Company. GY has consulting/research relationships with Opko, Eli Lilly and Company, Pfizer, Akros, GlaxoSmithKline, LEO, Sienna, Novartis, Celgene, TREVI, Regeneron, Sanofi, Menlo Therapeutics, and Allergan.


 Click to show fullsize
Click to show fullsize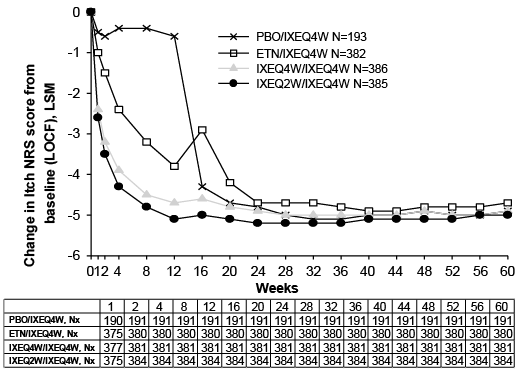 Click to show fullsize
Click to show fullsize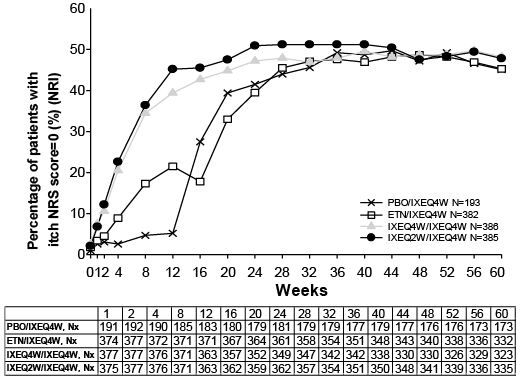 Click to show fullsize
Click to show fullsize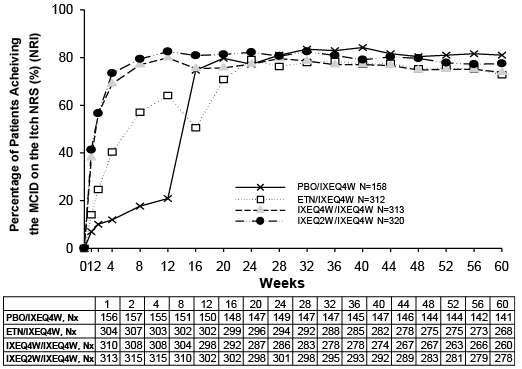 Click to show fullsize
Click to show fullsize