


Departments of 1Medical Psychology and 4Dermatology, 5Scientific Institute for Quality of Healthcare, Radboud University Medical Center, Nijmegen, 2Institute of Psychology, Health, Medical and Neuropsychology Unit, Leiden University, 3Leiden Institute for Brain and Cognition, and 6Department of Psychiatry, Leiden University Medical Center, Leiden, The Netherlands
Chronic somatic conditions, such as psoriasis, arthritis psoriatica and rheumatoid arthritis, have a large impact on patients’ lives. Tailored therapist-guided internet-based cognitive-behavioural therapy (ICBT) has been shown to be effective in improving physical and psychological well-being in these patients. Two cases are presented here, in order to provide an in-depth illustration of the course and content of this novel treatment and to investigate the therapeutic alliance in an online treatment. After face-to-face intakes, both patients received therapist-guided ICBT tailored to their specific problems and treatment goals. The treatment resulted in improved physical and psychological well-being and these clinically significant improvements were maintained at 6-month follow-up. In addition, the therapeutic relationship was evaluated positively by both patients and increased further during treatment, indicating an adequate therapeutic working alliance in this online treatment. These case reports show that tailored ICBT may contribute to improved care for patients with chronic somatic conditions.
Key words: internet-based intervention; e-health; psoriasis; rheumatoid arthritis; cognitive-behavioural therapy; personalized medicine; tailored treatment.
Accepted Sep 27, 2017; Epub ahead of print Sep 27, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Andrea W. M. Evers, Institute of Psychology, Health, Medical and Neuropsychology Unit, Faculty of Social and Behavioural Sciences, Leiden University PO Box 9555, NL-2300 RB Leiden, The Netherlands. E-mail: a.evers@fsw.leidenuniv.nl
Chronic somatic conditions, including chronic skin and pain conditions, such as psoriasis (PS), arthritis psoriatica (PsA) and rheumatoid arthritis (RA), have a large impact on patients and society at large as a consequence of their significant physical and psychosocial impact. Patients with these conditions are confronted with several physical complaints, including pain, fatigue, and itch, as well as psychological complaints, such as anxiety and depression, and experience limitations in their daily life functioning (1–4). PS, PsA and RA are all auto-immune conditions that share specific characteristics with regard to skin problems and pain symptoms. PsA and RA cause inflammatory arthritis in the joints, leading to pain, stiffness, chronic fatigue, limitations in daily life functioning, and a diminished health-related quality of life (HRQoL) (5, 6). Fatigue has been identified as a key symptom in patients with PsA and RA and was added to the core outcome set for future studies, highlighting its importance (7–9). Both PS and PsA lead to skin lesions characterized by red plaques covered with scales. Although there might be some differences with regard to the specific pathophysiological mechanisms, the experienced symptoms and burden of illness is found to be comparable in these patient groups (5, 10–12). With regard to psychological functioning, approximately 30–40% of the patients with chronic skin and pain conditions have elevated distress levels and can be considered at risk for long-term psychological adjustment problems (13–16). Therefore, a multidisciplinary approach to the treatment of these patients is vital. Psychological treat-ments, such as cognitive behavioural therapy (CBT), have been shown to be effective as an adjunct to regular medical treatments to improve physical and psychological wellbeing for patients with chronic skin and pain conditions (17–19). In addition, several studies underline the relevance of individually-tailored CBT interventions that take patient-specific risk and resilience factors into account to further improve treatment adherence and effectiveness and decrease attrition rates (20–22). How-ever, as the lack of specialized therapists and the time and travel burden for patients limit the implementation of tailored CBT, offering these interventions online might present important advantages (23). Research shows favourable effects of internet-based CBT (ICBT) for chronic somatic conditions (24–26). For example, one randomized, controlled trial (RCT) showed that unguided ICBT can improve quality of life and levels of anxiety in patients with PS, but was limited by high drop-out rates (27). Guided ICBT has been associated with lower drop-out rates and generally higher effectiveness than ICBT without therapist support (28–32). Therapist-guided ICBT has been shown to be effective for improving psychological outcomes (e.g. anxiety, depression and distress), disease-specific physical outcomes (e.g. pain, fatigue, disability) and disease-related impact outcomes (e.g. quality of life) (24, 26). These results are similar to those for traditional face-to-face approaches.
The therapeutic relationship has been shown to be an important factor in predicting treatment outcome in face-to-face treatments (33). Also in online treatments, the quality of the patient-therapist relationship might be related to treatment satisfaction and patient-reported improvements (34, 35). Preliminary evidence suggests that the therapeutic relationship in internet-based treatments is comparable to that of face-to-face treatments (34, 36–38). However, little is known about which factors contribute to a successful therapeutic relationship over the internet (34). An internet-based treatment may pose a challenge for developing a good therapeutic relationship; for example, due to the absence of any non-verbal cues. On the other hand, patients report specific advantages of internet-based treatment that may contribute to an effective therapeutic alliance, for example the anonymity that makes it easier to share personal problems (39).
The efficacy of a tailored ICBT approach for patients with chronic somatic conditions with a psychological risk profile was studied in 2 randomized, controlled trials (RCTs) for patients with PS (40) and patients with RA (41).
The current paper describes 2 cases with different diseases in order to illustrate this psychological approach, which can be used for a variety of problems reported by patients with various chronic somatic conditions, including chronic skin and pain conditions, such as PS, PsA and RA. Therefore, the selected cases experience problems that are representative of these conditions, including itch–scratch problems, chronic fatigue, physical limitations, and negative mood. The value of case reports is increasingly being recognized in addition to RCTs, as this design incorporates unique features, such as an in-depth description of the course and content of the intervention and the exploration of factors contributing to possible treatment effectiveness (42). The aim of the present article is therefore to provide an in-depth illustration of the course and content of the tailored therapist-guided ICBT, through 2 case reports differing in symptomatology and treatment goals, including challenges and obstacles that might be encountered. In addition, the development of the therapeutic alliance in the online treatment is investigated.
For the 2 RCTs from which the cases reported here were selected, inclusion criteria were a diagnosis of PS or RA, age ≥ 18 years, and a psychological risk profile (score ≥ 5 for anxiety and/or ≥ 21 for negative mood measured by the Impact of Rheumatic Diseases on General Health and Lifestyle (IRGL; 43, 44) or the Impact of Chronic Skin Disease on Daily Life (ISDL; 45). Exclusion criteria were: (i) pregnancy, (ii) insufficient understanding of the Dutch language, (iii) severe physical or psychiatric comorbidity, (iv) current treatment by a cognitive behavioural therapist, and (v) no access to a computer and internet. After a screening procedure and written informed consent, patients were randomized to the control group, who received standard medical care, or the intervention group, who received additional ICBT (for a full description of both trials, see http://www.trialregister.nl/trialreg/admin/ rctsearch.asp trial no. NTR2100 and NTR2436). For these case reports, 2 patients were selected from the RCTs who were representative for the ICBT treatment with regard to their reported problems, treatment goals and the applied cognitive-behavioural techniques.
Assessments were made with validated instruments before treatment, post-treatment and at 6-month follow-up (FU) (for comparability reasons the 3-, 9- and 12-month follow-up assessments of the RA trial were not included). Tables SI and SII give an overview of the outcome measures used for both the PS and the RA patient.
Physical functioning. Fatigue was measured with the 8-item fatigue subscale of the Checklist Individual Strength (CIS; 46, 47) in both patients. Itch was assessed in the patient with PS with the 4-item itch subscale of the ISDL. Pain was assessed in the patient with RA with the IRGL pain scale. Higher scores reflect more symptoms of fatigue, itch and pain.
Psychological functioning. For both cases, depressive symptoms were assessed with the Beck Depression Inventory (BDI; 48) and negative mood and anxiety by their respective scales of the IRGL/ISDL, with higher scores reflecting worse psychological functioning.
Impact on daily life. Role limitations due to physical health problems and emotional problems of the RAND-36 Health Status Inventory were assessed, with higher scores reflecting less impact (49, 50). For the patient with RA, the self-care and mobility scales of the IRGL were also administered, with higher scores indicating better functioning.
Cognitive-behavioural factors. Cognitive-behavioural factors were assessed, including illness cognitions of helplessness and acceptance (Illness Cognitions Questionnaire, ICQ; 51), social factors including perceived social support (IRGL/IHDL) and stigmatization (ISDL; only for the patient with PS), and worrying (Penn State Worry Questionnaire, PSWQ; 52). In addition, for the patient with PS, scratching behaviour was assessed with the subscales conscious scratching and automatic scratching of the ISDL. For the patient with RA, passive (resting, retreating, worrying) and active (pain transformation, distraction, reducing demands) pain coping was assessed with the Pain Coping Inventory (PCI; 53).
Disease-related variables. Disease activity was assessed in the patient with PS with the Psoriasis Area and Severity Index (PASI; 54), with higher scores signifying greater disease severity. The Self-Administered Psoriasis Area and Severity Index (SAPASI; 55) was also used to measure self-assessed disease severity, with higher scores indicating more severe self-perceived psoriasis. For the patient with RA, disease activity was assessed using the self-report measure Rheumatoid Arthritis Disease Activity Index (RADAI; 56), with higher scores reflecting higher self-reported disease activity. Medical treatment compliance was assessed with a questionnaire asking how often patients adhered to medical treatment prescriptions/recommendations with regard to several aspects of the medical care (57). Each question could be answered on a 5-point Likert scale, ranging from less than once a week to 7 days a week, or could be answered as “not applicable”. Total scores were constructed by calculating the mean of applicable items, with higher scores indicating greater self-reported compliance.
Therapeutic relationship. To assess the quality of the therapeutic relationship, the Working Alliance Inventory short-form (WAI-S; 58, 59) was administered after the 2 face-to-face intakes and at the end of treatment. A higher score indicates a more positive therapeutic alliance. In addition, the newly developed Internet-Specific Therapeutic Relationship Questionnaire (ITRQ; 35) was used, with higher scores reflecting a more positive therapeutic alliance.
Patient evaluation. Finally, an evaluation questionnaire was administered post-treatment to assess patients’ satisfaction with the ICBT intervention and their evaluation of the user-friendliness of the website on a 10-point scale. In addition, they were asked to evaluate on a 6-point scale whether the contact with the therapist was motivating and useful.
Post-treatment and 6 months’ follow-up scores of the 2 cases were compared with their baseline scores (pre-assessment) and to scores of normative samples (healthy controls or normative group of patients with PS or RA for outcomes that can only be assessed in patient populations). Clinically significant improvement was defined in 2 ways: (i) showing a change from baseline of more than 0.5 standard deviation (SD), using the SD of the normative sample (60), and (ii) showing an improvement from baseline of at least 30%, as recommended by the IMPPACT guidelines for clinical trials (61).
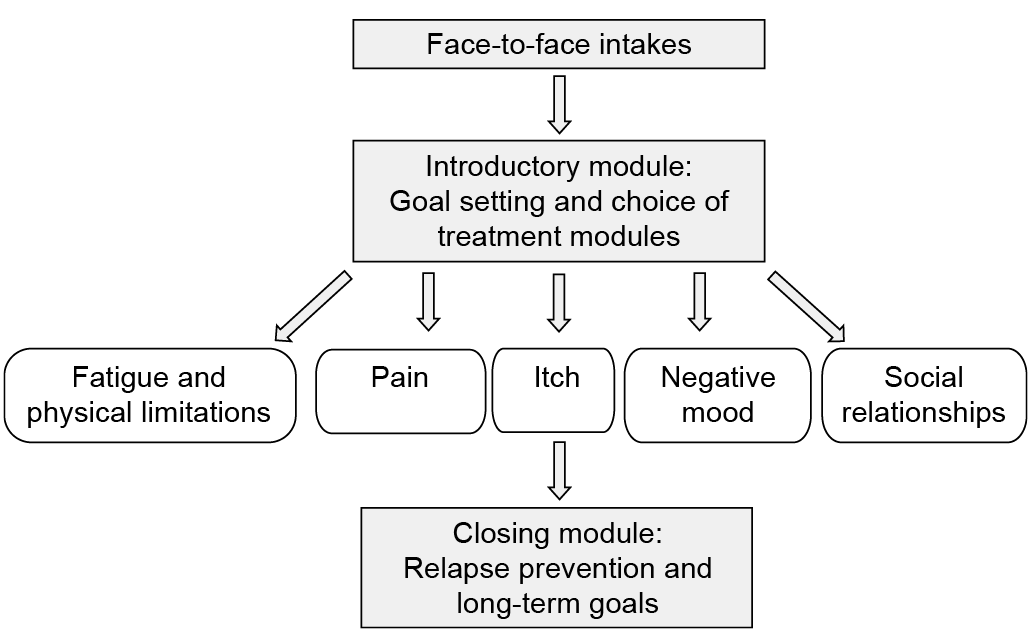
Prior to ICBT, patients were invited to attend 1 or 2 face-to-face intake sessions with the therapist, during which the treatment goals were mutually determined. Thereafter, patients started with the online intervention. The ICBT began with an introductory module, during which the specific treatment targets within one or 2 of the 5 treatment modules (pain, itch, fatigue and physical limitations, negative mood, and social relationships) were selected based on the pre-treatment assessment and the intake interviews. Next, within the chosen treatment modules a flexible protocol was used, consisting of various assignments, such as self-monitoring exercises and psycho-educational texts. The ICBT was designed as a tailored, personalized treatment. The therapist selected assignments and online texts that were most suitable to patients’ individual problems, treatment goals, and perpetuating cognitive-behavioural factors, and gave individualized feedback on assignments approximately once a week. In addition, patients could send messages to the therapist at their own discretion. The treatment concluded with relapse prevention and long-term goals (see Fig. 1 for a schematic overview of the treatment). The treatment protocol was based on techniques from face-to-face standardized treatment protocols for various chronic somatic conditions (20, 22, 62, 63).
Fig. 1. Overview of the therapist-guided, tailored internet-based cognitive-behavioural treatment.
Case description. A 64-year-old man, married, retired, had had progressive skin complaints since he was 36 years old, diagnosed as PS. PS is a chronic inflammatory auto-immune skin condition that causes red plaques covered with white scales that are frequently accompanied by itch, fatigue and, occasionally, pain. The skin condition had a large impact on his daily life. He reported having high levels of itch and, in response, he scratched a lot. He also scratched as an automatic behaviour unrelated to itch, e.g. as a habit and in stressful situations. This scratching behaviour led to skin damage and an aggravated skin condition, which resulted in even more itch. Thus, a vicious cycle of itch-scratching problems developed (64, 65). He also reported feeling depressed and anxious as a result of his psoriasis. He felt helpless in dealing with his skin complaints due to numerous unsuccessful coping efforts. In addition, due to shame with regard to his scratching behaviour, he avoided social activities, which further aggravated his negative mood. He also found it difficult to accept the unpredictable nature of his condition. This led to a high level of experienced stress and he reported that this, in turn, negatively affected the psoriasis.
The pre-assessment supported a high level of itch, scratching behaviour, negative mood and feelings of helplessness compared with a norm group (Table SI). Based on this assessment and according to the face-to-face intakes, in which the treatment goals and specific treatment modules tailored to these goals were mutually determined by the patient and therapist, the ICBT consisted of the treatment modules itch and negative mood in achieving the treatment goals of diminishing itch-scratching problems and improving mood. The course of the treatment will be described below in order to illustrate different treatment methods of the ICBT in more detail.
Treatment. The ICBT consisted of the introductory module, module itch, module negative mood, and the closing module. The patient logged in 47 times, completed 37 assignments (95% of the total given assignments), received 13 messages from the therapist, and sent 11 messages within a period of 5 months (1-week introduction module, 8-week itch module, 9-week negative mood module, 2-week closing module). In addition, one phone call was made by the therapist during the online treatment to clarify a given assignment.
Introductory module. In the introductory module, treatment goals were set. For this patient, the most important treatment goals were decreasing itch-scratching problems and improving mood. Because the itch and scratching problems were of central importance and also influenced his mood, the itch module was chosen as a starting point.
Itch module. Several psycho-educational texts and exercises were used to diminish the itch-scratching problems. First, he started to keep a self-monitoring diary on which, every day at a set time, he recorded the level of itch and the number of times he scratched himself, in addition to recurrent risk situations for itch and scratching. Next, psycho-education about the vicious cycle of itch-scratching problems was provided and exercises to decrease scratching, including habit reversal in which patients learn to replace scratching with incompatible behaviour. He indicated that the self-monitoring exercises made him more aware of his scratching behaviour and that the incompatible behaviour was helping him to control his scratching better. Attention was also paid to coping techniques to deal with triggering factors of itch and scratching. For example, since water was a triggering factor for the patient’s itch, he took shorter showers. Because the patient felt very stressed when he experienced itch, psycho-education was provided about the relationship between stress, itch, and scratching, in addition to exercises about stress-relieving strategies, such as itch-relieving thoughts and visualizations. For example, he began using self-thoughts such as “I can tolerate the itch” and “The itch will go away eventually”, which helped him stay more relaxed when the itch increased.
Negative mood module. Given the high levels of stress, the patient experienced in his daily life and the possible negative effect on his psoriasis, in the negative mood module attention was paid to stress management. Several methods to deal with stress were offered, e.g. relaxation exercises, distraction, problem-solving, and reappraising the situation. He had access within the website to various audio-tracks that contain recorded relaxation exercises (including progressive muscle relaxation, cued relaxation, and visualization exercises). He completed one exercise a day and reported that this had a positive effect on his perceived stress. He was also encouraged to regularly apply relaxing and distracting activities in his daily life, e.g. reading, gardening, cycling, and walking. In addition, cognitive restructuring techniques were applied. The patient learned to challenge dysfunctional cognitions, such as “It is pointless” and “Nothing is helping”, and transform them into more helpful thoughts such as “I can manage”. After several weeks, he indicated that he was barely stressed anymore, his depressive feelings were greatly diminished, and he withdrew less from social activities.
Closing module: relapse prevention and long-term goals. Given the progress with regard to the treatment goals, it was mutually decided to end the treatment. The closing module dealt with relapse prevention and further improvement of the attained goals. The patient stated that he achieved all of his goals. A relapse prevention plan was formulated by the patient, including detecting early signs of relapse (e.g. tension) and preventive actions (e.g. relaxation exercises).
Case description. A 26-year-old woman, living together with a steady partner, had started having pain in her wrist and knee one year previously. A few months later, she was diagnosed with RA by her rheumatologist. RA is characterized by inflammation in the joints that frequently leads to functional disability, pain, and fatigue. The patient worked as a dental assistant for 32 h a week. Pain and fatigue were her most prominent complaints, which limited her daily activities. She tried to ignore her complaints, rested very little between activities and would spend only a small amount of her time on pleasant activities. Whenever she had relatively few complaints, she was very active to make up for earlier periods of experienced loss of productivity. However, these peaks of activity were generally followed by days of exhaustion. In the long run, this over-exertion pattern had led to an increase in complaints and exhaustion. She also worried a lot about how to deal with her complaints and limitations. Her worrying and the diminishment of pleasant activities had a negative impact on her mood.
The pre-assessment supported the over-exertion pattern and showed very high levels of pain and fatigue, depressive symptoms, high levels of worrying, and low acceptance compared with a norm group (see Table SII). Based on this assessment and according the face-to-face intakes in which the treatment goals and specific treatment modules tailored to these goals were mutually determined by the patient and the therapist, the ICBT of the patient consisted of the treatment modules fatigue and physical limitations and negative mood in achieving the treatments goals of less fatigue and improved mood.
Treatment. The ICBT for the patient consisted of the introductory module, fatigue and physical limitations module, negative mood module and the closing module. In total, the patient logged in 45 times, completed 31 assignments (82% of the given assignments), received 20 messages from the therapist and sent 22 messages within a period of approximately 6 months (1-week introduction module, 10-week fatigue and physical limitations module, 7-week negative mood module, 3-week closing module).
Introductory module. In this module, treatment goals were set. For the patient, the most important treatment goals were improving her level of fatigue and, to a lesser extent, pain (e.g. better alternation of rest and activity, becoming more aware of limits) and improving her mood (e.g. less worrying, less depressive mood).
Fatigue and physical limitations module. By means of self-monitoring of daily activities and levels of fatigue, pain, and mood, it was revealed to the patient that she went on with activities for a long time without breaks, which increased her complaints. In addition, a registration of her daily activities and the amount of energy that each activity costs revealed that she overexerted herself on most days. Psycho-education with reading texts was given regarding the importance of balancing activity and relaxation to prevent symptoms from aggravating, in addition to exercises aimed at achieving this balance, e.g. structured planning of daily activities and activity pacing (alternating activity and relaxation, spreading out intense activities), balancing enjoyable, important, and necessary activities. The patient indicated that she profited greatly from planning her activities more carefully, while focusing more on enjoyable activities. Since she reported waking up very tired in the morning, attention was paid to sleep hygiene. By keeping a sleep schedule for a few days, she learned that being too busy before going to bed caused her poor sleep quality. She started addressing this problem by implementing more relaxing activities, such as reading or taking a bath before she went to bed, which diminished her fatigue complaints in the morning.
Negative mood module. In the negative mood module, psycho-education about coping with worrying and exercises about stress-management strategies was offered. The patient regularly practiced various coping techniques (e.g. planning 15 min a day for worrying, distraction, problem-solving, and challenging dysfunctional thoughts). Attention was also paid to increasing the amount of pleasant activities and the patient was asked to schedule at least one enjoyable activity per day. She was actively involved in this exercise and felt that it improved her negative mood symptoms. In addition, attention was paid to coping with dysfunctional thoughts by using techniques such as cognitive restructuring, problem-solving and distraction. Finally, relaxation exercises were provided to help her diminish her worrying further and to create more moments of relaxation in her daily life. In a telephone call, she indicated that, due to a new job, she had no time to practice these exercises at the moment. Therefore, she was offered an audio-CD with the exercises, so she could practice these in the future.
Closing module: relapse prevention and long-term goals. Given the progress with regard to the treatment goals, it was decided to conclude the treatment. In the closing module, attention was paid to relapse prevention and future goals. The patient reported having reached all of her treatment goals to a large extent. In a relapse prevention plan, she formulated early signs of relapses (e.g. increase fatigue) and preventive actions (e.g. adjust daily planning, include more time for relaxation and pleasant activities).
After completing the interventions, both case 1 and case 2 reported that the intervention had been very helpful and rated the overall intervention as a 9 on a 10-point scale. Case 1 reported that he could cope better with the itch, scratched less and had greatly diminished his feelings of helplessness and depression. Case 2 reported to be better able to respect her boundaries and stop in time. Her fatigue and pain complaints were greatly diminished, she worried less and her mood was improved. With regard to the internet-delivered aspect of the treatment, both patients evaluated the user friendliness of the website positively (case 1: 9; case 2: 10; scale 1–10). Furthermore, specific items of the ITRQ showed that they both reported as important advantages of online treatment that they had the time to think about the message to the therapist (case 1: 10; case 2: 10; scale 1–10), it was easier to share personal problems (case 1: 8; case 2: 10; scale 1–10), and that writing down their feelings and thoughts helped to clarify them (case 1: 10; case 2: 10; scale 1–10). Case 1 also reported as advantage the ease of following a treatment at home and not having to travel to the hospital (case 1: 8; scale 1–10). Furthermore, they both stated that the face-to-face intakes were a very important aspect of the treatment (10, scale 1–10). In addition, they both indicated that the contact with the therapist was very motivating (6, scale 0–6) and useful (6, scale 0–6). Finally, they both indicated a preference for internet-based treatment over other forms of treatment (phone-based, face-to-face) for future treatment.
For case 1, with regard to physical functioning, improvements were found for itch and fatigue at post- and follow-up assessments. Also, improvements were found for psychological functioning, including negative mood and depression. The level of anxiety was diminished at post-assessment, but the score at the FU showed a slight increase. The impact on daily life was at the maximal level at pre-treatment and remained stable during the treatment and at FU. In contrast, the clinician-assessed disease severity worsened slightly between pre- and FU-assessment, suggesting the possible use of more adequate cognitive-behavioural strategies to cope with the symptoms and consequences of the disease. Indeed, the level of helplessness and scratching behaviour decreased. No large differences were found with regard to the level of worrying, which was within the range of healthy controls at all assessment. Also, illness cognitions of acceptance remained overall stable. The level of social support was already high at pre-treatment and the experienced stigmatization low, and these outcomes remained stable. Also, case 1 had the maximal score for treatment compliance at pre-, post- and FU-assessment. With regard to the clinical relevance of these results, case 1 showed improvements of > 0.5 SD for all outcomes at post-assessment and FU, with the exception of anxiety and acceptance at FU. In addition, the improvement from baseline was at least 30% for most outcomes at post-assessment, with the exception of itch, acceptance, worrying and the self-assessed disease severity, and for most outcomes at FU, with the exception of itch, anxiety, acceptance, worrying and clinician-assessed disease severity (Table SI).
For case 2, large improvements were found for the physical outcomes of pain and fatigue (at FU within range of healthy controls). In addition, the psychological outcomes showed relatively large improvements, including depression, negative mood, and anxiety. With regard to the impact on daily life, self-care and emotional role functioning were at the maximal level at pre-treatment and remained stable, and relatively large improvements were found with regard to level of mobility and physical role functioning. However, the disease severity of case 2 also decreased, which makes it difficult to determine whether these improvements can be attributed to the psychological treatment alone. Nevertheless, the cognitive-behavioural factors at post-treatment indicate that she applied more adaptive pain-coping techniques, such as distracting and reducing demands, and she also rested more. No changes were found with regard to the pain-coping strategies of transforming pain and retreating. At follow-up, case 2 stated she could not complete the pain-coping measures because she did not have pain anymore. In addition, feelings of helplessness diminished, acceptance improved and her level of worrying decreased. Social support was already at the maximal score at pre-treatment and remained stable. Also, the treatment compliance was at a maximal score at all assessment points. With regard to the clinical relevance of these results, case 2 showed improvements of > 0.5 SD for most outcomes at post-assessment, with the exception of social support and the pain-coping strategies of retreating, worrying, and transforming pain, and on all outcomes at FU. In addition, the improvement from baseline was at least 30% for most outcomes at post-assessment, with the exception of pain, anxiety, and the pain-coping strategies of resting, retreating, worrying and transforming pain, and for all outcomes at FU (see Table SII).
The results of the WAI (Table I) showed that the agree-ment on treatment tasks and treatment goals was already high after the face-to-face intakes and improved even further during treatment. Also, the emotional bond was established at the maximal level after the face-to-face intakes and remained stable during the online treatment without direct face-to-face contact. In addition, results for the internet-specific aspects of the therapeutic alliance assessed with the ITRQ showed a similar pattern. More specifically, both patients reported that it was clear from the assignments and messages from the therapist that she had thought thoroughly about what is important for them at the moment, that the therapist had paid sufficient attention to their problems and treatment goals, and took their personal problems seriously.
Table I. Mean scores of cases 1 and 2 at pre- and post-assessment on the therapeutic relationship outcomes including the range of measures used
ICBT has been shown to be effective for patients with several chronic somatic conditions. These 2 case reports provide an in-depth illustration of the course and content of a therapist-guided tailored ICBT approach for patients with chronic somatic conditions, such as PS, PsA and RA, and a psychological risk profile. In addition, the development of a therapeutic alliance in an internet-delivered treatment was investigated. For both cases the tailored ICBT approach proved effective. Post-treatment clinically meaningful improvements were found with regard to their physical and psychological wellbeing, which remained stable or further improved 6 months after treatment, suggesting that both patients continued to benefit from the treatment. Also, the cognitive-behavioural factors, including illness cognitions, social support, worrying and coping strategies, showed clinically relevant improvements at post-treatment and follow-up. Furthermore, a successful therapeutic alliance was established for both patients after the face-to-face intakes, which further improved during treatment.
Over the last few years, researchers and clinicians have increasingly focused on the importance of tailoring treatment to patients’ needs in order to improve treatment efficacy and increase adherence. As psychological distress can influence disease course, adherence and treatment success, it is clinically relevant to select patients with a psychological risk profile (66, 67). Therefore, in our RCTs, only patients with a heightened distress level at risk for long-term adjustment problems were selected for the ICBT. In addition, since incorporating patient preferences may increase treatment satisfaction and lower attrition rates, the specific treatment modules were matched to the outcomes from which the patients suffered most (28). Finally, based on the cognitive-behavioural factors that were assumed to perpetuate the complaints, specific assignments were chosen within the treatment modules. For example, for both patients the negative mood module was relevant, but for case 1 the focus within the module was on diminishing feelings of helplessness and experienced stress, and for case 2 on diminishing her worrying and increasing pleasant activities. Although the HRQoL is equally diminished in chronic somatic conditions, such as PS, PsA and RA, it has been argued that different aspects of the disease might contribute to this lowered HRQoL (10). For example, in PsA and RA it has been suggested that the physical symptoms and fatigue impact the patient most, while PS might have a greater impact on mental health (including social functioning) (6, 68). Case 2, indeed, experienced high levels of fatigue and pain that limited her daily life functioning. Case 1, however, did not experience limitations in his social functioning and was also mostly impaired in his physical functioning due to the high levels of experienced itch. Nevertheless, the specific factors contributing to diminished HRQoL in a specific patient also needs to be taken into account when tailoring treatment to specific problems.
The results of the therapeutic alliance support earlier findings on the possibility of successfully forming and maintaining a therapeutic relationship in internet-delivered treatments. Since the working alliance at the beginning of treatment can be predictive of treatment outcome, as was also shown in a psoriasis RCT (40), this is an important result. There are various conceptualizations of the therapeutic alliance, but most share 3 themes: (i) collaborative nature, (ii) affective bond between patient and therapist, and (iii) ability to agree on treatment goals and tasks (33). Specific aspects of this ICBT treatment focused on these themes, which might have contributed to the development of this adequate therapeutic relationship, including the face-to-face intakes to establish the emotional bond, treatment goals that were mutually determined, the personalized treatment plan, assignments and messages, and regular contact with the possibility for the patients to send messages to the therapist at their own discretion. These aspects were highly valued by both patients. Further research is needed to investigate the development of a therapeutic alliance in internet-based treatments in more detail, for example by including other treatment modalities, such as video conferencing and chatting, where the verbal cues are not missing.
Several limitations of this study need to be taken into account. The results of the case reports do not prove the efficacy of this tailored treatment, which has been evaluated in RCTs (40, 41). In addition, it is unclear whether these results can be generalized to a broader population, including patients with physical and/or psychiatric comorbidity. ICBT might only be suitable for patients with chronic somatic conditions with moderate adjustment problems, while a face-to-face treatment is needed for those patients with severe adjustment problems or multimorbidity. Due to the tailored approach and generic treatment modules, this ICBT could also be useful for patients with other chronic somatic conditions, including patients with chronic skin conditions, chronic pain conditions, diabetes, and cardiovascular conditions, al-though future research is needed to establish this further. Furthermore, future research should aim at delineating the specific mediating and moderating factors of this tailored ICBT. In addition, more research is needed with regard to ways of establishing the clinical relevance of treatment effects.
In conclusion, ICBT offers several advantages, such as the absence of travelling time, and costs and flexibility in choosing the time of treatment. These case reports demonstrate that a therapist-guided, individually tailored ICBT treatment is feasible and can result in meaningful changes for patients with chronic somatic conditions and a psychological risk profile.
This work was supported in part by grants from Pfizer (WS682746) and ZonMw (The Netherlands Organisation for Health Research and Development) (170992803). Pfizer and ZonMw were not involved in the study design, data collection, data analysis, manuscript preparation, or publication decisions. The authors are not aware of any conflict of interest influencing this work.
The authors would like to thank IPPZ for collaboration in the design of the online programme and for ongoing technical support. We would like to thank our patient research partners Henk van Duijn, Mariette Tomas, Hen Ros†, and Ilse van Ee for their contributions to the development of the intervention website and research. We would especially like to thank the participating patients for their collaboration in this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize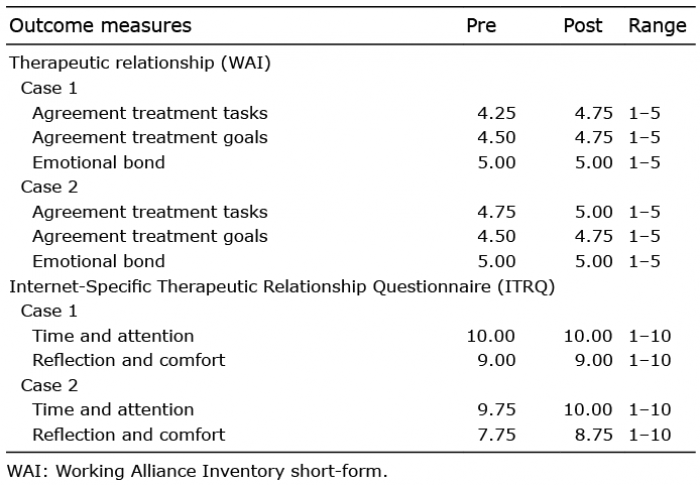 Click to show fullsize
Click to show fullsize