


1Department of Dermatology, Radboud University Nijmegen Medical Center, Nijmegen, and 2Health, Medical and Neuropsychology Unit, Institute of Psychology, Leiden University, Leiden, The Netherlands
Alopecia areata (AA) is an immune-mediated disease causing temporary or permanent hair loss. Up to 46% of patients with AA also have nail involvement. The aim of this study was to determine the presence, types, and clinical implications of nail changes in patients with AA. This questionnaire-based survey evaluated 256 patients with AA. General demographic variables, specific nail changes, nail-related quality of life (QoL), and treatment history and need were evaluated. Prevalence of nail involvement in AA was 64.1%. The specific nail signs reported most frequently were pitting (29.7%, p = 0.008) and trachyonychia (18.0%). Red spots on the lunula were less frequent (5.1%), but very specific for severe AA. Nail-related QoL was only minimally affected by nail changes. In conclusion, nail involvement is common in patients with AA and presents mostly with pitting and trachyonychia. The presence of these nail changes reflects the severity of the disease, with red spots on the lunula as a predictor for severe alopecia.
Key words: alopecia areata; quality of life; prevalence; nail disease; survey.
Accepted Oct 2, 2017; Epub ahead of print Oct 2, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Yvonne B. M. Roest, Department of Dermatology, (370), Radboud University Nijmegen Medical Center, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. E-mail: Yvonne.Roest@radboudumc.nl
Alopecia areata (AA) is an immune-mediated disease that is characterized by non-scarring hair loss. The disease may be limited to one or more discrete, well-circumscribed round or oval patches of hair loss on the scalp or body (alopecia areata focalis; AAF), or it may affect the entire scalp (alopecia areata totalis; AAT), or even the entire body (alopecia areata universalis; AAU). The natural course of the disease is unpredictable, but often benign. Spontaneous regrowth of hair occurs in 80% of patients within the first year, but relapses at any given time are not uncommon. Poor prognostic factors include bald patches persisting for more than one year, onset of hair loss before puberty, a positive family history of AA, ophiasis pattern, associated nail changes, atopy, and Down syndrome (1). Severity of AA at onset is perhaps the most important negative prognostic factor (2). A lifetime incidence between 0.57% and 3.8% has been reported in hospital-based studies worldwide (3). AA may appear at any age, but as many as 60% of patients with AA will present with their first patch before 20 years of age (4), and prevalence peaks between the 2nd and 4th decades of life (1).
AA is a lymphocyte cell-mediated inflammatory form of hair loss in which a complex interplay between genetic factors and underlying autoimmune aetiopathogenesis is suggested, although the exact aetiological pathway is unknown (5). Some studies have shown association with other auto-immune diseases, including asthma, atopic dermatitis, and vitiligo (6).
Many patients with AA also have nail involvement, with a reported incidence ranging from 9% to 46% (7, 8). Incidence is much lower in patients with focal AA than in patients with severe forms of AA (9, 10), and may be higher in children than in adults (8, 11). Nail changes may either precede the hair loss or occur months or years later, and may persist even after hair regrowth. The patho-genic mechanism of nail changes in AA is unknown, but it has been proposed that because the nails are similar in structure and growth to hair follicles, they are affected by the same inflammatory reaction that targets hair follicles in AA. Histopathological observations using light and electron microscopic techniques show that most of the nail changes in AA are found within the proximal matrix, and are less pronounced in the distal matrix, and negligible in the nail bed (12). The fact that the nail matrix is far more often involved than the nail bed results in a clinical presentation of matrix-derived nail changes that may include pitting, trachyonychia, onychorrhexis, Beau’s lines, onychomadesis, and nail thinning with or without koilonychia (8). Anonychia and scarring are not typically seen. Red spots on the lunula are rarely present, but are highly suggestive for the diagnosis AA (13). Nail bed signs are uncommon and only one case of severe onycholysis has been reported to date (14).
Studies in the field of nail changes in patients with AA are sparse. The aim of this study was to evaluate nail involvement in patients with AA, the impact on quality of life (QoL), and to evaluate a potential unmet need for treatment.
This study was conducted in collaboration with the Dutch Alopecia Patient Association between April 2013 and October 2013. A questionnaire was distributed to all 930 members of the alopecia association, together with a letter inviting participation and explaining the purpose of the study, and reply-paid envelopes. The questionnaire was completed anonymously and no incentives were given. It contained questions concerning general demographic variables, QoL, and specific nail changes thought to be attributed to AA. Also, patients experience of current and previous treatments for the nails were assessed. Nail signs assumed to be due to AA, i.e. pitting, trachyonychia, leukonychia, crumbling, red spots on the lunula, and koilonychia were illustrated with photographs. Based on these photographs, patients could indicate which of these nail features were present. If patients had other nail changes, they could report these in their own words, and these were categorized later by an experienced dermatologist. QoL was assessed using the nail psoriasis QoL scale (NPQ10), a questionnaire primarily developed and validated to measure QoL in patients with nail psoriasis (15). This scale was used unmodified for the measurement of QoL for patients with AA with nail involvement. The first question concerns the pain intensity of nail changes and the other 9 questions concern the functional impairment caused by their nail involvement in daily life. Each response is scored from 0 to 2, with the response “not” and “never” scoring 0, “sometimes” and “a little” scoring 1, and “very” and “always” scoring 2 points. The question concerning the interference of nail changes with the ability to drive a car was removed because the target population also included minors. The NPQ10 scale used therefore has a range from 0 (no impairment of QoL) to 18 (maximum impairment of QoL).
Data were entered in a database and statistical analysis was subsequently performed using Statistical Package for Social Sciences (SPSS 20.0, IBM Corp, Armonk, NY, USA). Descriptive statistics were provided using mean ± standard deviation (SD) and median (range) for normally and non-parametrically distributed numerical values, respectively. Frequencies and percentages were used for categorical variables. Missing values were not included to calculate percentages. Continuous variables with normal distribution were tested by unpaired t-test and the results are presented as mean ± SD. Categorical variables were represented by frequencies and percentages and analysed by χ2 or Fisher’s exact test. Missing values were not included in calculations of percentages. Statistical analysis of more than 2 means was performed with one-way analysis of variance (ANOVA). Statistical significance was considered at a level of 5% (p < 0.05) for all tests.
A total of 930 questionnaires were distributed and 347 were returned within 6 months, a response rate of 37.3%. Most patients (88.2%) had AA. Other respondents had other types of alopecia, mostly pattern hair loss (PHL; 8.7%). Fifty questionnaires from patients with AA were excluded because the questions concerning nail involvement were not completed, resulting in 256 questionnaires from patients with AA that were available for analysis. The 30 questionnaires from patients with PHL served as controls, because nail involvement has not been reported in these patients, while questionnaires from patients with cicatricial alopecia, telogen effluvium, and trichotillomania were excluded because of their low prevalence. Also, questionnaires from patients with AA diffusa were excluded because it was considered that some patients might not have been able to discriminate between this type of AA and other more diffuse forms of non-scarring alopecia.
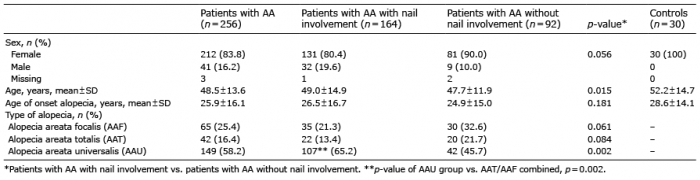
The distribution of patient characteristics is shown in Table I. Most patients had severe AA: 74.6% had AAT or AAU, while 25.4% had AAF. A vast majority of respondents were female (83.8%), and a small majority of respondents (64.1%) had experienced nail involvement at any time during the course of their AA. The incidence of nail abnormalities in the control group was 36.6%, which is significantly lower than among any group of patients with AA (p = 0.007). More than 65% of patients with AA with nail involvement had AAU (p = 0.002), while most patients without nail involvement (54.3%) had milder forms of AA. There was a tendency for nail involvement to be more frequent in males than in females (p = 0.056). The mean age ± SD of the respondents with AA was 48.5 ± 13.6 years. Patients with nail involvement were slightly older than those with AA without nail involvement. The mean age of onset of hair loss was 25.9 ± 16.1 years without significant differences between patients with AA with and without nail involvement. Nail changes developed, a mean of 7.9 years later than the alopecia (Table II).
Table I. Characteristics of patients with and without nail involvement in alopecia areata (AA) and the control group (pattern hair loss, PHL)
Table II. Characteristics of patients with nail changes divided into the 3 forms of alopecia
In over half of the patients with AA, only the fingernails were involved. Isolated involvement of the toenails was reported in 1 out of 8 patients with AA, while involvement of both toenails and fingernails was reported by one-third of respondents. The mean number of involved fingers was 7, and was similar among all 3 groups of patients with AA (p = 0.90), while the mean number of involved toenails was higher among patients with AAU than among those with AAF or AAT (p = 0.009).
A total of 164 patients with AA reported that their nails had been affected at some time during the course of the disease. This corresponds to 64.1% of the returned complete questionnaires. The reported nail signs are shown in Table III and were compared with the control PHL group.
Table III. Nail signs in patients with alopecia areata (AA) compared with control group (pattern hair loss, PHL)
Pitting, crumbling, leukonychia, and trachyonychia are the most commonly observed nail changes in AA. Of these, leukonychia and crumbling were also reported in rather high percentages in the control group. Koilonychia (3.1%) and red spots on the lunula (5.1%) were reported in a few patients with AA, but in none of the control patients. Brittleness, splitting, onychorrhexis, and onychoschizia are signs of brittle nail syndrome and were reported in approximately 10% of both the patients with AA and the controls. Onycholysis, slow nail growth, disappearing lunula, and onychomadesis were all reported once in AA (n = 1, 0.4%).
All nail features were reported more frequently in patients with AAU than in patients with AAF/AAT, but this difference was significant only for red spots on the lunula (p = 0.04).
The results for nail-related QoL are shown in Table IV (NPQ10). The mean NPQ10 of patients with nail changes and mean ± SD AA score was 0.91 ± 1.61. There was no significant difference between sex and QoL (NPQ10 was 0.84 in males and 0.92 in females, respectively). There was a tendency to a higher impairment score in patients with both toenail and fingernail involvement, compared with patients with only fingernail or only toenail involvement. (NPQ10 was 1.07, 0.88, 0.86, respectively, p = 0.066). Looking at the activities or complaints separately, patients with nail involvement were most restricted in putting on socks. The results in NPQ10 of the control patients were not significantly different from those with AA (data not shown). The mean NPQ10 in this group was 1.40. Similar to patients with AA, putting on socks was also the problem most often encountered the control group.
Table IV. Nail-specific quality of life results (NPQ10)
Twenty-two (13.8%) of the 164 patients with AA with nail involvement indicated having received any treatment for their nail disorder. Topical corticosteroids were mentioned by 4 patients, tar ointment by one, topical chlorhexidine cream by one, an unspecified cream/ointment by 2 patients, and intralesional steroids by one patient. Oral treatments included biotin (n = 2), vitamin B complex (n = 1), vitamin D (n = 1), vitamin E (n = 1), and antifungals (n = 8). Other systemic treatments, including oral corticosteroids, methotrexate, or cyclosporine were not reported. Of all mentioned therapies, 8 patients experienced positive treatment results with vitamin B complex (n = 1), vitamin D (n = 1), vitamin E (n = 1), biotin (n = 2), chlorhexidine cream (n = 1), nail hardener (n = 1), and pedicure treatment (n = 1).
Patients were asked about their desire for effective treatment of nail changes caused by AA. If patients had not received treatment in the past, they were asked about their desire to have treatment. Thirty-five percent reported a desire for such a treatment, while 65% considered their nail abnormalities too limited to justify any treatment. Furthermore, 76.9% of patients with nail changes had no confidence in the effectiveness of available treatment options, 28.7% thought that treatment would be uncomfortable, and 39.8% of the patients assumed it would be time-consuming. Fig. 1 shows the amount of time patients reported being willing to spend on treatment of their nails per day. Most patients wanted to spend less than 5 min per day. Less than 10% were willing to spend more than 15 min per day in order to improve their nails.
Fig. 1. The time patients with alopecia areata (AA) are willing to spend treating their nail abnormalities.
Nail changes occur frequently in patients with AA and indicate a poor prognostic factor (7). The aim of this study was to evaluate the prevalence and signs of nail involvement in patients with AA, the impact on QoL, and to evaluate a potential unmet need for treatment. Our results showed nail involvement in most patients with AA, more frequently in patients with AAU than in patients with AAF. Pitting, leukonychia, and trachyonychia were reported most often, but red spots on the lunula appear to be most specific for (severe) AA. QoL in patients with AA was only minimally affected by their nail changes. The nail-specific unmet medical needs appeared to be low, possibly due to lack of awareness of therapeutic options.
Among the 256 respondents in this study, nail involvement was reported in 64.1%. Severity of alopecia was a major determinant in reported incidence. Nail involvement was reported in 53.8% (35/65) of patients with AAF, while 71.8% (107/149) of the patients with AAU reported nail involvement. Patients with PHL were included as controls because nail involvement has not been reported in these patients. Also, among these controls, nail signs were reported relatively frequently, in 36.6% (11/30), but significantly less frequently than in patients with AA. The reported prevalence and incidence of nail involvement in AA in the literature ranges from 9.0% to 46% (Table V) (5, 7–9, 11, 16–18). Reported incidence was lowest in a retrospective file study focusing on several clinical characteristics of 216 Korean patients with AAT or AAU (9). Nail signs were not specified in this study, but were more frequently noted in the clinical file in early-onset patients with AA (16.9%) than in patients with late-onset AA (7.1%). A higher prevalence of nail abnormalities in children (46%) than in adults with AA (19%) was also reported by Tosti et al. (8). In our study the age of onset of AA did not differ between patients with AA with nail involvement, and those with AA without nail involvement. This might be due to the specific design of our study, which included patients who had been diagnosed, on a mean of 24 years previously. Nail abnormalities developed, on a mean of 7 years after the onset of the hair loss. This suggests that even if nail involvement is more present in children presenting with AA, nail involvement will occur in the course of the disease as frequently in patients with later onset AA. Most studies reported a lower incidence or prevalence of nail involvement in AA than our study. There are several possible explanations for this. Firstly, we reported the lifetime incidence of nail changes, while several other studies reported point-prevalence of nail changes at the time of the first visit to an outpatient clinic, or during a short period of follow-up. Secondly, our group consisted of patients with severe AA; almost 60% had AAU. Nail involvement is more frequent among patients with severe AA, not only in this study, but also in other reports (8, 11, 16, 17, 7). Sharma et al. (11) reported a prevalence of nail dystrophy of 19.1% in their whole group, with a higher incidence of 49.4% in the severe forms of AA. Garcia-Hernandez & Rodriguez-Pichardo (16) reported nail changes as a risk factor for developing severe forms of alopecia. In the study by Gandhi et al. (17), none of the patients with AAF had nail changes. A third factor that might have affected the results is the scoring of nail involvement. This study used patient-reported data with photographs in a questionnaire. Patients themselves may have a low threshold for reporting abnormalities. The relevance of this factor is underlined by the high incidence of nail abnormalities reported in the control group (36.6%). Only one other study on nail involvement in AA included a control group (11). Unfortunately, the incidence of nail involvement in their control group was not all reported, but it appears to be even higher than in patients with AA. Nail involvement was reported in 19.8% of patients with AA, leukonychia was present in 15.1% of controls, and longitudinal ridges in 26.4% of controls.
Table V. Literature overview of nail signs in patients with alopecia areata (AA)
Apart from one patient with onycholysis, only signs of nail matrix disease were observed in our study. The absence of nail bed signs, such as onycholysis and subungual hyperkeratosis, indicates that the nail matrix is the only site of inflammation in AA (12). The specific nail signs that were reported most frequently in patients with AA were pitting (29.7%), and trachyonychia (18.0%). Both of these were more frequent than among the controls. Red spots on the lunula were reported by fewer patients with AA (5.1%), but not at all reported in the control group. Patients with AAU had a significantly higher risk of developing red spots on the lunula (8.1% vs. 0.9%) than did patients with AAT and AAF. Pitting and trachyonychia were also the most common nail changes in all previous studies (8, 11, 17). Sharma et al. (11) reported that longitudinal ridging, pigmented longitudinal bands, and punctate leukonychia did not occur more often in AA than in controls. Van der Velden et al. (19) has shown recently that leukonychia is a nail feature that is not disease-specific, which presents in 65% of healthy subjects. Also in our patients, leukonychia was found as a non-specific feature. Sharma et al. (11) introduced terminal “V” nicks of the nail plate as a new change recorded in association with AA. In our study, 3.1% of patients with AA reported distal notching. However, 3.4% of controls reported the same sign. Thus, leukonychia and distal notcching does not appear to be a specific sign for AA of the nails. Three out of 274 children were reported by Tosti et al. (8) to experience onychomadesis during the acute onset of AA universalis. In our population, only one patient reported onychomadesis, making it a rare sign of AA of the nails.
Patients with AA often experience marked psychological distress. The disease can have detrimental impact on patients QoL. A recent systematic review showed that patients with AA consistently demonstrate poor QoL scores, with greater extent of scalp involvement associated with lower QoL (20). Health-related QoL in AA is similar to that of other chronic dermatological diseases, such as psoriasis or chronic dermatitis. Also, nail disease may have serious effects on QoL. For example, patients with psoriasis have a significantly lower QoL when the nails are involved than when the nails are uninvolved (21). Many tools have been used to assess QoL in patients with AA, including the Dermatology Life Quality Index (DLQI), Skindex-16, Short Form Health Survey (SF-36), and several others (20). None of these questionnaires include questions concerning nail involvement. Therefore, no date or scoring systems were available to access the contribution of nail involvement in QoL of patients with AA. In this study, we used the NPQ10 scale, which is a QoL questionnaire specifically related to the impact of nail impairments on QoL, developed for nail psoriasis (15). The results show a low impact of nail changes on the QoL of patients with AA with a mean score of 0.91, which was similar to the controls. Nail involvement in AA appears to be much less troublesome than in nail psoriasis, because the mean score in those patients was 9.9 (22). In general, nail psoriasis is more extensive, painful, and has major signs of nail bed disease, for example onycholysis, which may cause a major handicap for patients, resulting in higher scores on the QoL scale. A more specific QoL questionnaire focusing solely on nail matrix signs could be designed and validated for nail changes in AA, but from our results it is suggested that nail involvement is of major importance for only a few individual patients with AA.
A minority of 13.7% of patients with AA received any treatment for their nails. In most cases, this treatment was considered ineffective. Approximately one-third of patients with AA desire an effective treatment for their nails, while most considered their nail abnormalities too limited to justify any treatment. The unmet need for treatment in patients with AA is much lower compared with nail psoriasis patients (22), which correlates with the much higher impact nail involvement has in psoriasis, as measured by NPQ10.
In summary, nail involvement in patients with AA is common and presents mostly with pitting and trachyonychia. The severity of the nail changes reflects the severity of the disease, with red spots on the lunula as a predictor for severe alopecia. Impairment of QoL by nail involvement is limited in the majority of patients, and the unmet need for treatment is lower compared with nail psoriasis. However, the latter could be an underestimation, since lack of awareness of therapeutic options may play a role. Nail involvement should not be overlooked in trials on AA, because its presence and improvement may be a relevant factor in individual patients.
This project was funded by by the Dutch alopecia areata association, Zoetermeer, the Netherlands.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize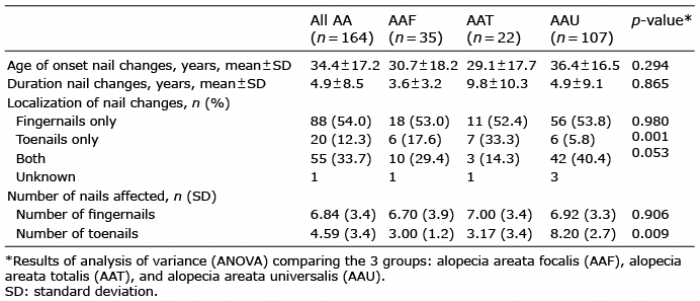 Click to show fullsize
Click to show fullsize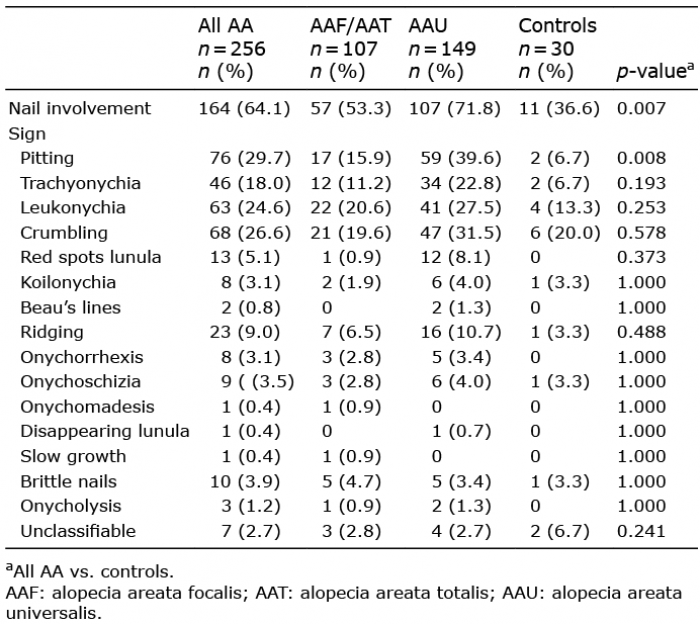 Click to show fullsize
Click to show fullsize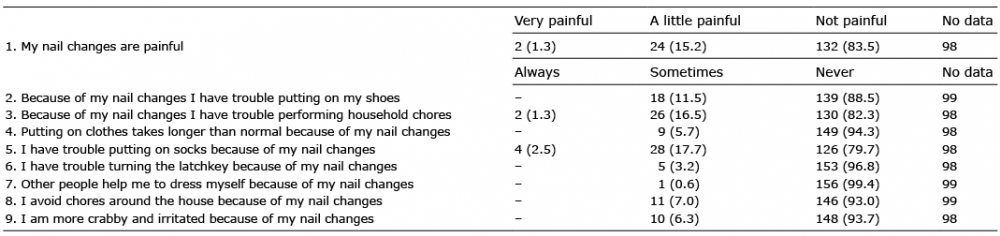 Click to show fullsize
Click to show fullsize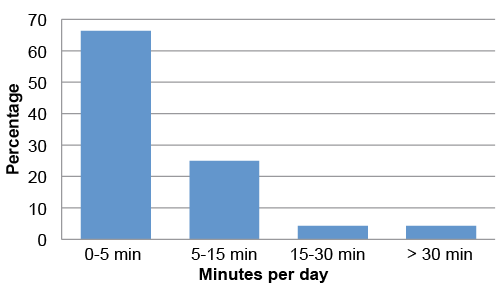 Click to show fullsize
Click to show fullsize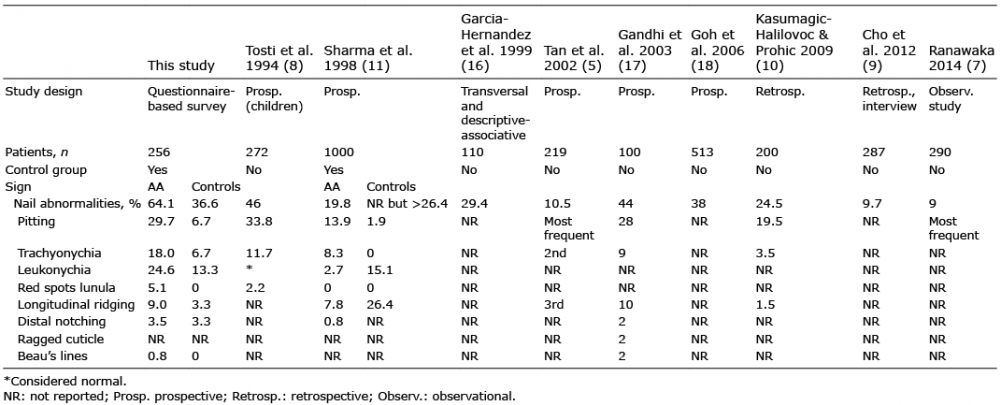 Click to show fullsize
Click to show fullsize