


1Department and Clinic of Dermatology, Venereology and Allergology, and 2Department and Clinic of Hematology, Blood Neoplasms and Bone Marrow Transplantation, Wroclaw Medical University, Wrocław, Poland
Aquagenic pruritus (AP) has a significant influence on quality of life (QoL) in patients with polycythaemia vera. This study analysed the impact of AP on patient well-being in 102 patients with polycythaemia vera. Intensity of pruritus was evaluated using a visual analogue scale (VAS), verbal rating scale (VRS) and a 4-item Itch Questionnaire. Psychosocial aspects of AP were assessed with the Hospital Anxiety and Depression Scale (HADS), EQ-5D and itch-specific QoL questionnaire (ItchyQoL). AP of mean duration 6.6 ± 8.6 years and intensity 4.8 ± 1.9 points (VAS) was present in 42/102 individuals. The prevalence of depression and anxiety among patients with AP was 23.8% and 9.5%, respectively. Depression was more frequent in the AP group (vs. non-AP). Moreover, patients with AP had higher HADS-anxiety scoring than those without pruritus (p = 0.005). A negative correlation was found between duration of AP and EQ-5D-VAS. The ItchyQol score of 37.3 ± 12.3 points was influenced by the extent (p =0.01) and duration of episodes of AP (p = 0.02). In conclusion, AP places an additional burden on patients with polycy-thaemia vera, negatively influencing their QoL.
Key words: aquagenic pruritus; polycythaemia vera; hydrophobia; anxiety; depression.
Accepted Oct 2, 2017; Epub ahead of print Oct 3, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Jacek C. Szepietowski, Department and Clinic of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chałubińskiego 1, PL-50-368 Wrocław, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Aquagenic pruritus (AP) is a debilitating dermal condition characterized by the development of intense itching, stinging, tingling or burning sensations, without observable skin lesions, brought on by contact with water of any temperature (1). AP is recognized to be a pathognomonic sign of polycythaemia vera (PV), which is one of the main clonal haematological malignant neoplasms caused by mutations of a cytoplasmic tyrosine kinase, Janus kinase 2 enzyme (either JAK2V617F or JAK2 exon 12) (2, 3). Furthermore, homozygotic mutations of JAK2 among patients with PV were found to be significantly more often associated with AP (4).
PV-associated pruritus was first reported in 1985 (1) and its estimated prevalence varies, according to data, from 31% to 69% of patients (5–7). Notably, the onset of AP precedes diagnosis of PV in almost half of cases (8).
AP has a significant influence on patients’ quality of life (QoL), depriving patients of sleep, and can lead to development of a psychological phobia and abandonment of bathing (9). Moreover, the majority of patients believe that pruritus is the most unmanageable aspect of PV, which may lead, in more severe cases, to a reduced physical and social life (1).
Although AP is recognized as the most excruciating aspect of PV, studies evaluating its impact on the psychosocial state of patients with AP are limited (1, 8). The aim of this study was therefore to analyse the clinical features of AP, and its influence on patient well-being, in a group of patients with PV.
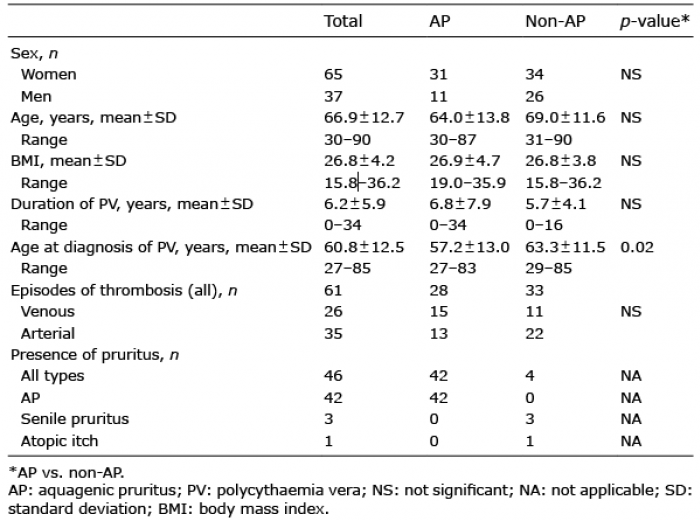
The study was conducted on a group of 102 patients (65 females, 37 males), with PV diagnosed according to the WHO criteria. All of the patients had the JAK2V617F mutation. The age range of the studied individuals was 30–90 years (mean ± standard deviation (SD) 66.9 ± 12.7 years). The majority of PV patients were treated with 5-hydroxyurea (5-HU) (71.6%) and phlebotomy (66.7%). Less frequently, patients were treated with acetylsalicylic acid (40.2%), clopidogrel (9.8%), anagrelide (7.8%) and pipobroman (2.9%). PV was adequately controlled in 45.6% of patients (10). All patients underwent a physical examination and, those who reported pruritus brought on by contact with water with no observable skin lesions, were treated as having AP. The individuals who had pruritus of origin other than AP (e.g. senile pruritus, atopic itch, etc.) were excluded from the AP group. Only 3 patients had anti-pruritic treatment with antihistamines. The detailed characteristics of the study group are shown in Table I. Patients without AP served as matched controls (with regard to age, sex, body mass index (BMI), duration of PV and number of thrombotic episodes).
The study was approved by the Ethics Committee of Wroclaw Medical University (No. 355/2016).
Table I. Characteristics of studied groups
Demographic data, disease history, PV status and treatment modalities were collected from all participants. Unidimensional scales were used to evaluate AP intensity, including a visual analogue scale (VAS) and verbal rating scale (VRS). With regard to VAS, the patients were asked to report, and mark on the 10-point scale, the maximum and mean intensity of pruritus they had experienced during the last 3 days. The scores ranged from 0 (no itch) to 10 points (worst imaginable itch). VAS scoring is as follows, mild pruritus (0–<3 points), moderate pruritus (≥ 3–7 points), severe pruritus (≥7–9 points) and very severe pruritus (≥ 9 points).
In VRS, participants assessed their itch intensity as: “mild”, “moderate”, “severe” or “very severe”. In addition, the pruritus was characterized with a 4-item Itch Questionnaire. This instrument was successfully utilized previously by our group to estimate the extent (1–3 points), intensity (1–5 points), frequency (1–5 points) and sleep disturbances (0–6 points) caused by pruritus of various types (11–17). Ratings ranged from 3 (mild pruritus) to 19 points (very severe pruritus).
In order to evaluate a wide spectrum of psychosocial aspects all patients were asked to complete the validated Polish language versions of multiple questionnaires, including the Hospital Anxiety and Depression Scale (HADS), EQ-5D and an itch-specific quality of life questionnaire (ItchyQoL).
HADS, developed by Zigmond & Snaith (18), is used as a self-evaluation rating scale of 14 items designed to measure anxiety and depression (7 items for each subscale). Responses to particular items are indicated on a 4-point Likert scale, ranging from 0 to 3 (score range for each subscale, 0–21 points), where high scores indicate more symptoms. A cut-off score of ≥ 11 points in each subscale indicates a significant number of symptoms of anxiety or depression corresponding to confirmed cases.
With regard to EQ-5D (the standardized instrument, comprising a 3-level, 5-dimensional, descriptive system, was used as a measure of health outcome), patients assessed their health-related QoL with a total of 243 EQ-5D health states (243 = 35). A utility score was assigned to each health state using the York A1 tariff (17); EQ-5D scores range between 0.594 (worst) and 1 (full health). In addition, the EQ-5D is supplemented by a visual analogue scale (EQ-5D-VAS) on which patients recorded an individual assessment of their own overall health status on the examination day on a scale of 0 to 100 (0 = worst; 100 = best imaginable health state) (19).
Patients’ AP was also evaluated with ItchyQoL, the first questionnaire solely dedicated to the assessment of itch influence on QoL, by evaluating 3 dimensions, namely, symptoms (S), function-ing (F) and emotions (E) (19). The ItchyQoL assessment consists of 22 questions, scored on a 5-point scale ranging from 1 (never) to 5 (all the time), with the sum forming the overall ItchyQol score with a range of 22–110 points. The overall ItchyQoL score corresponds to the level of pruritus-specific HRQoL impairment, with 0–30 points (very mild), 31–50 points (mild), 51–80 points (moderate) and 81–110 points (severe impairment) (20). Moreover, subscale scores of S, F and E are calculated as the mean of scores pertaining to that particular category (range 1–5 points) (21).
All data were assessed for parametric or non-parametric distribution. Pearson’s χ2 test was applied to sets of categorical data. Differences between groups were determined using the Mann-Whitney U test and Kruskal–Wallis test, or Student’s t-test, with reference to the distribution of evaluated variables (non-normal or normal, respectively). Correlations were determined by Spearman’s correlation analysis. The resulting p-values were considered nominally significant at p < 0.05 level; the Holm-Bonferroni correction for multiple comparisons was used. Statistical analyses were performed using Statistica 12 software (StatSoft, Tulsa, OK, USA).
AP was present in 42 out of 102 (41.1%) individuals, and was more common in women (31 out of 42). No individual presented a coexistence of AP with pruritus of another cause. The presence of AP was not determined with reference to control of PV.
The range of duration of AP was 0–44 years (mean 6.6 ± 8.6 years). Approximately half of the patients experienced AP every day (52.4%), while among the remaining patients pruritus tended to appear a few times per week (38.1%) or per month (9.5%).
According to VAS, the maximum intensity of AP during last 3 days was assessed as 5.2 ± 2.4 points (range 1.2–10 points), whereas mean VAS was 4.8 ± 1.9 points (range 2.5–8.7 points). With reference to VRS the AP was usually “moderate” or “mild” (38.1% and 28.6%, respectively), while “very severe” itching was experienced by 11.9%. The mean result for 4-item Itch Questionnaire in subjects with AP was assessed as 6.0 ± 2.9 points (range 3–15 points) and correlated strongly with VAS and VRS (p < 0.0001, for both variables).
With reference to HADS, the prevalence of depression and anxiety disorders among AP patients was estimated as 23.8% and 9.5%, respectively. It is worth noting that depression was significantly more frequent in this group (10/42) compared with non-AP PV controls (5/60; p = 0.03). Despite the lack of significant differences in the frequency of anxiety, patients with AP had notably higher anxiety subscale scoring than patients without AP (p = 0.005) (Table II). Moreover, AP patients with anxiety had 1.6 times higher VAS score in comparison to the rest of AP group (7.9 ± 0.5 vs. 4.9 ± 2.4), however, the use of Bonferroni–Holm adjustment returned no statistical differences.
Table II. Questionnaires’ scores and dependencies on selected clinical data
Neither EQ-5D, nor EQ-5D-VAS showed any statistical differences between these 2 groups (Table II). Of note, a negative correlation between duration of AP and EQ-5D-VAS (R = –0.45, p = 0.003) was found, whereas, with PV duration and EQ–5D-VAS, such dependence was not shown (R = –0.13, p = 0.17).
The mean ItchyQol score was assessed as 37.3 ± 12.3 points. A strong positive correlation between the intensity of pruritus, estimated with VAS, and ItchyQol was found (R = 0.66; p < 0.0001). The same phenomenon was also observed for VRS (p < 0.0001) (Fig. 1). Moreover, ItchyQol scores were significantly influenced by the extent of AP (p = 0.01) and the duration of its episodes (p = 0.02) (Fig. 2). AP-related impairment of QoL was within a range from little to moderate, with 38.1% of patients indicating little, 45.2% mild, and 16.7% moderate impact. With reference to the results for the subscales, all assessed dimensions (S, F, E) were quite equally scored, with no differences between sexes (Table III).
Fig. 1. Correlations between ItchyQoL and pruritus intensity (visual analogue scale (VAS), verbal rating scale (VRS)).
Fig. 2. Influence of the extent of aquagenic pruritus (AP) and duration of its episodes on ItchyQoL.
Table III. ItchyQoL subscales’ results among patients with aquagenic pruritus
Sleep disturbances, described as waking during the night due to itching, were observed among 16.7% of patients with AP. The group of patients with AP who had sleep disorders obtained significantly higher scores with regard to HADS-anxiety, ItchyQol and VAS (p = 0.02, p < 0.001 and p < 0.0001, respectively) (Fig. 3). It is worth noting that 33.3% of patients with AP avoided any contact with water. Moreover, patients with higher VAS scores avoided contact with water significantly more often (p = 0.003).
Analysing several other factors, including the patients’ sex, age, BMI, PV onset or duration, age at AP diagnosis or treatments applied, we were unable to find any significant relationships between these factors and the questionnaire-related scores.
Fig. 3. Sleep disturbances according to Hospital Anxiety and Depression Scale (HADS)-anxiety, ItchyQol and visual analogue scale (VAS).
PV-associated pruritus was described for the first time more than 3 decades ago, but its pathophysiology, frequency and management have not been fully established (5, 9). Amongst the limited published data focusing on the impact of AP on QoL among patients with PV, it was emphasized that AP has an unfavourable effect on patients’ sleep quality, social and occupational activities, could lead to the avoidance of contact with water, and was treated by many patients as the worst symptom of PV (5). Despite the fact that AP is a common symptom, resulting in significant distress, it remains an underestimated clinical feature of PV. This analysis is the first documentation of AP among patients with PV, which focuses only on the influence of AP on QoL issues, by means of different validated questionnaires.
In contrast to the study by Siegel et al. (8), the occurrence of AP among our patients was intriguingly lower (68.2% vs. 41.2%, respectively). This could be explained by the design of their research, which was based on an anonymous questionnaire comprising 21 open and multiple choice questions to assess PV status and AP characteristics. Comparing this method with ours it appears that the physical examination and medical interview could be more accurate for recognition of AP. Regardless of the method chosen, the limitation of our cross-sectional study was the analysis concerning only one clinical centre with no insight into clinical course of PV, which means that the extrapolation of results to patients of other regions should be conducted with some caution. Moreover, the anti-pruritics given to patients with AP could be regarded as confounding factors; how-ever, there were only 3 patients with antihistamines administered and these had no effect.
In our study anxiety and depression were found to be linked to AP. Similar findings have been reported previously in studies of other itchy dermatoses, indicating such co-occurring disorders (e.g. depression) to be more frequent among patients with pruritus and in turn, that negative emotional states can intensify the condition (22, 23). The results from our study revealed that, among patients with AP, depression and anxiety disorders are relatively frequent and, within our demographic, can be found in approximately 24% and 10% of patients, respectively. Of note, the presence of AP in studied individuals was not only responsible for an increase in the prevalence of depression, but also for exacerbation of anxiety levels. The results we have obtained may point to AP as a distressing factor, resulting in the higher probability of the development of depressive symptoms, as the recent data indicate that 12.5% of patients with a BCR-ABL-negative myeloproliferative neoplasm meet the HADS criteria for depression. This prevalence is concurrent with cases of depression reported among all of our patients with PV (14.7%) (24). The mean levels of anxiety (5.5 ± 4.4 points) for myeloproliferative neo-plasms, reported by McFarland et al. (24), were also slightly lower than those observed among our patients with AP.
Thanks to common and worldwide usage of the HADS questionnaire it is quite easy to conduct an assessment comparing not only myeloproliferative disorders, but also any other itchy condition (including dermatoses) with PV-associated AP. For instance, the HADS results obtained in our study showed comparable deterioration to some other pruritic skin disorders, including atopic dermatitis (25) or psoriasis (26), both traditionally considered as causing significant disability. Moreover, in concordance to our results, the data found for dermatological patients experiencing chronic itching also revealed that the group with pruritus had more symptoms associated with anxiety (27). In comparison with these diseases, it can be concluded that PV with accompanying AP seems to be a highly distressing condition for many patients. Some of the authors (28) implied that dissociative states could be a functional way of coping with chronic pruritus, as it may be a way to withdraw from the unpleasant experience of pruritus.
Such consequences of the influence of AP on QoL were also demonstrated by Siegel et al. (8). They measured morbidity in 441 patients with PV (180 with molecularly confirmed PV), using the EORTC QLQ-C30 questionnaire, and found a decreased overall QoL among patients with AP, primarily a more pronounced fatigue and pain, as well as higher incidence of dyspnoea and reduced role and cognitive functioning. Our findings may indirectly lead to similar conclusions, as they revealed the statistically significant correlation between pruritus intensity and water avoidance. As a consequence, it may even lead some patients with AP developing a phobia of bathing (9), which again highlights the influence of AP in patients with PV. Furthermore, abandoning contact with water could have a negative influence on a patient’s social and occupational life (i.e. role functioning).
According to EQ-5D we did not notice any significant differences between pruritic and non-pruritic patients; however, score totals were decreased in both groups and comparable to those observed in other chronic diseases, e.g. psoriasis (29), hidradenitis suppurativa (Hurley I and II) (30), bronchial asthma or chronic obstructive pulmonary disease (COPD) (31), cerebral strokes (32) or blood circulation failure qualifying for heart transplantation and heart infarcts (33, 34). This could also be explained as PV itself having a negative influence on patients’ health-related QoL.
When evaluating the ItchyQoL it was found that all of the patients with AP experienced QoL deterioration, which confirms their linkage. Surprisingly, according to our results based on this questionnaire, the impairment of AP-related QoL was, more often than not, estimated as having only a little-to-mild effect on the patient’s life, with no differences observed between symptoms, functioning and emotions. The results obtained were somehow lower than those observed for other pruritic conditions, including urticaria, dermatitis or idiopathic itch (19). The results pointed to the pruritus intensity, extent and duration of its episodes, as the most important factors related to QoL issues. It should be emphasized that AP impact on QoL in the majority of patients was also expressed through influence on sleep quality (this group also has a higher level of anxiety symptoms).
Treatment of PV-associated pruritus is challenging. The lack of insight into the pathogenesis of AP is probably the main reason for the ineffectiveness of earlier therapies. Despite the correction of morphological parameters during the treatment, with cytoreductive agents, the presence of AP could be explained by the symptomatic mode of action of these drugs, without, in fact, affecting the clinical course of the disease. Moreover, the main issue regarding treatment of AP is not only ineffectiveness of current therapies, but also the lack of ordering of any anti-pruritic treatment for patients with AP. In our study, anti-pruritics were administered to only 3 patients with AP (with no effect).
According to recent data, the innovative agents, such as JAK2-/JAK1-inhibitors and inhibitors of the mammalian target of rapamycin (mTOR), presented encouraging and promising outcomes (35, 36). Taking into account that patients with JAK2V617F-homozygous PV showed an increased frequency of pruritus compared with heterozygotes, drugs such as ruxolitinib could potentially serve as a therapeutic approach for AP management among patients with PV. This hypothesis may be confirmed by recent data on treatment with JAK2-/JAK1-inhibitors, which could bring, not only the normalization of blood morphology, but also relief in general symptoms, such as fatigue, night sweats or itching through targeting the signalling pathways of the EPO-receptor (37, 38).
In conclusion, impairments to psychosocial status are a serious problem in patients with PV. AP places an additional burden on affected patients, also impairing their QoL. This study highlights the serious impact of AP on a wide spectrum of psychosocial aspects, indicating pruritus intensity, its extent and duration as the most important factors negatively influencing patients’ well-being. These findings emphasize the need for the development of effective anti-pruritic treatments for patients with AP in order to improve their QoL. Moreover, the care of patients with PV should be facilitated by psychosocial support and mental health services.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize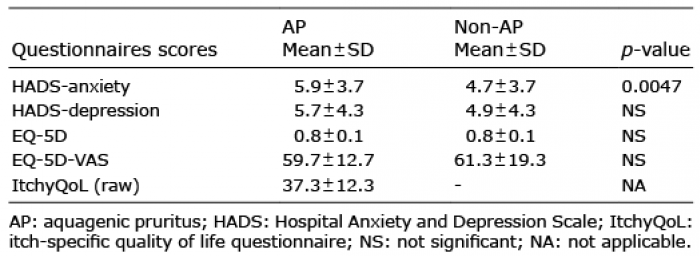 Click to show fullsize
Click to show fullsize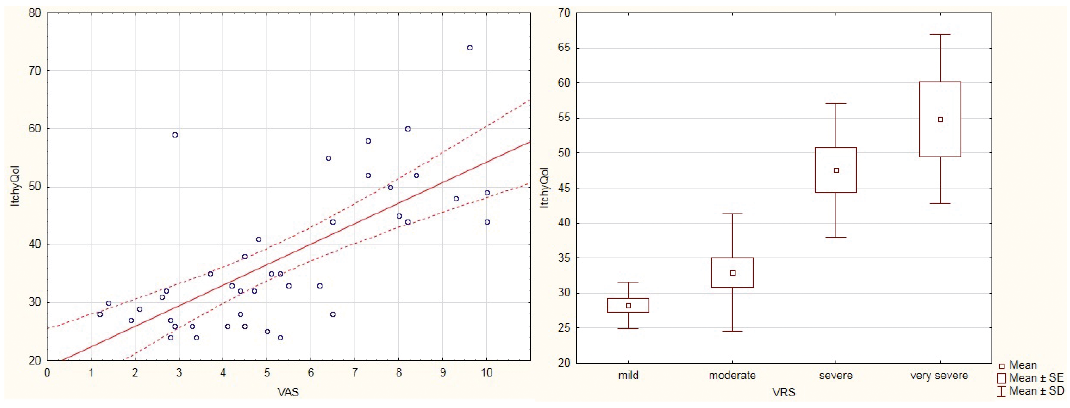 Click to show fullsize
Click to show fullsize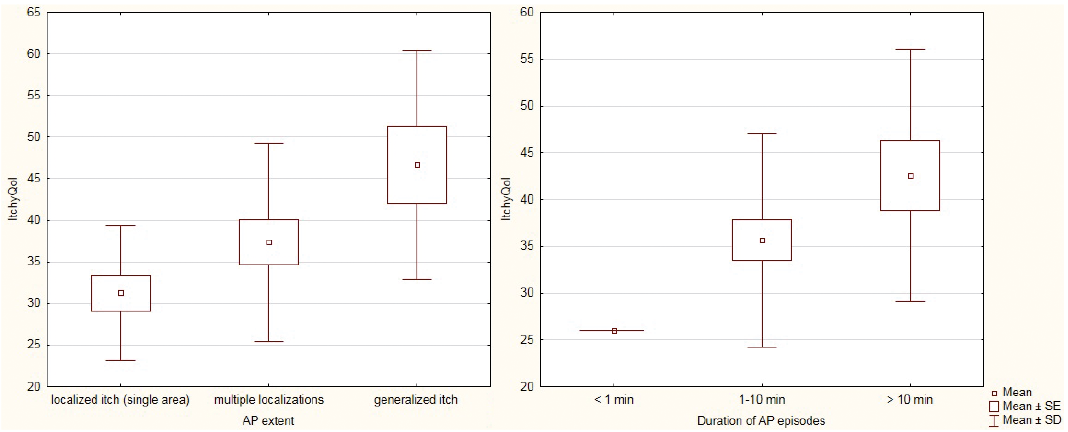 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize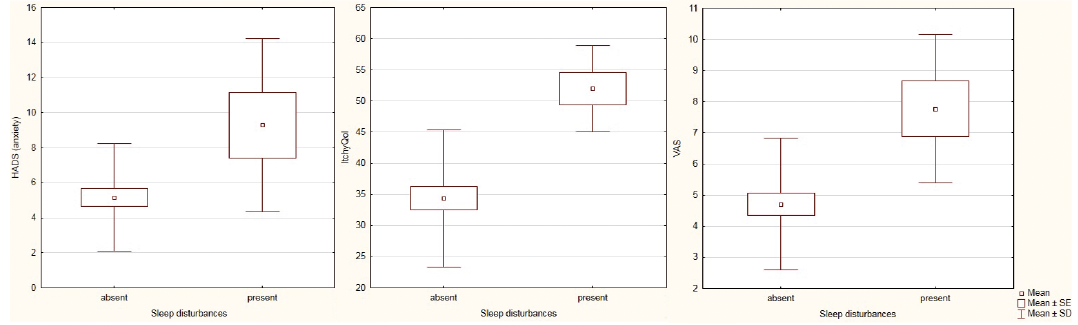 Click to show fullsize
Click to show fullsize