


1Department of Dermatology, and 2Department of Genetics, University Hospital Brest, CHU Morvan Brest, 2 avenue Foch, FR-29200 Brest, France. *E-mail: claire.abasq@chu-brest.fr
Accepted Oct 2, 2017; Epub ahead of print Oct 3, 2017
Neurofibromatosis type 1 (NF1), or von Recklinghausen’s disease, is an autosomal dominant, multisystem disorder that affects approximately 1 in 3,500 people. Up to 50% of cases of NF1 arise as a result of spontaneous mutations (1, 2). A diagnosis of NF1 is extremely difficult to communicate to patients and their parents because of the clinical variability, unpredictable evolution and uncertain prognosis of the disease. To our knowledge, only one study, published in 2000 (3), has evaluated the impact of conveying a diagnosis of NF1 to parents of an affected child.
The aim of the present study was to explore post-traumatic stress disorder (PTSD) in patients and the parents of children with NF1 following a diagnosis of de novo NF1.
Patients were recruited at the Neurofibromatosis Competence Center, Brest, France. Eligibility was based on the National Institutes of Health (NIH) criteria (1). Exclusion criteria were: familial forms of NF1 or the inability to complete the questionnaire because of cognitive or physical impairment. Familial forms were excluded because family’s background, knowledge, and experience are not the same and this could impact the final results.
A 5-page survey was posted to all eligible patients. Time to complete the survey was approximately 6 min. Questionnaire items were: demographic information, announcement circum-stances, open-ended questions on feelings after this announcement (anxiety, fear of complications), and access to further information about the disease. The final question involved the Impact of Event Scale – Revised (IES-R), as approved in French (4). The IES-R is a 22-item self-reporting instrument that assesses 3 symptoms of PTSD: intrusion, avoidance and hyper-arousal (5). The cut-off score for diagnosis of PTSD is 33 points; a score > 33 represents a diagnosis of PTSD. The study protocol was approved by the University Hospital’s ethics committee.
This study was carried out in the Brest Neurofibromatosis Competence Center, which opened in 2013. The files of 122 patients with NF1 were extracted from the centre database.
The questionnaire was sent to 53 eligible patients with the de novo NF1. Thirty-one questionnaires were returned (response rate 58.5%), comprising 12 adult patients and 19 parents of a child with NF1 (Fig. S1).
Mean patient age was 24.7 (range 2–77) years. There were 16 males and 15 females (Fig. S2, Table SI). For the children with NF1, the questionnaires were always completed by the children’s mothers (19/19).
The IES-R score was ≥ 33 in 14 cases, thus 45.2% of the patients or family members had PTSD after NF1 disclosure. Of these 14 people, 12 had IES scores > 37, thus 38.7% of the patients or family members had severe PTSD (96.8% response rate). Detailed results are shown in Table SII.
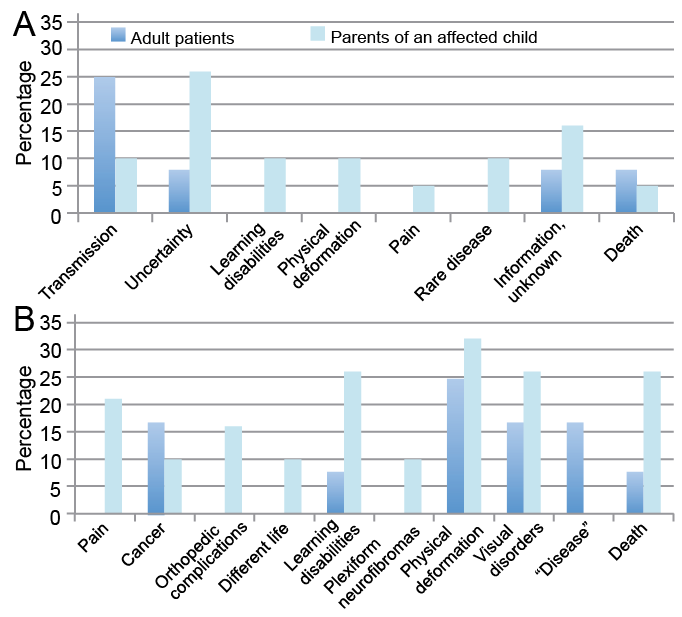
Fig. 1 shows anxiety and fear complications after diagnosis of NF1. In adult patients, genetic transmission was cited as a distress 3 times (in 25% of adult patients) (91.7% response rate). The parents of an affected child reported other feelings: uncertainty was cited 5 times (26.3% of families), learning disabilities, physical deformations, and genetic transmission were each cited twice (10.5%) (89.5% response rate).
Various complications were dreaded: adult patients mostly feared physical deformation (3 times, 25% of adult patients) (83.3% response rate). For parents, physical deformations were mentioned 6 times (31.6%), learning disabilities, visual disorders and death were each mentioned 5 times (26.3%) (94.7% response rate).
Twenty-four patients (77.4%) searched for more information on the Internet (74% response rate).
Fig. 1. Frequency of A) anxiety and (B) feared complications expressed after the first consultation.
To the best of our knowledge, this is the first study to describe the impact on patients and their families of disclosure of diagnosis in sporadic NF1. Ablon (3) reported only the parental response to the disclosure and realization that their child had NF1.
Our study shows that the diagnosis of this genetic disease is a traumatic event, as PTSD was a clinical concern in 16.1% of cases and was assessed in 45.2% of the people interviewed. The announcement was especially traumatic for the parents of the affected children, as 92.9% of the study subjects with PTSD were parents of a child with NF1. Most of these parents had a IES-R score > 37, meaning that they had severe PTSD. These data suggest that receiving a diagnosis of NF1 may be as difficult as receiving a cancer diagnosis. In previous Swedish studies describing PTSD in parents of children diagnosed with cancer, Hovén et al. (6) demonstrated that approximately half of them presented PTSD (PTSD Checklist-Civilian version was used) 4 months after diagnosis, whereas 19% of the mothers and 8% of the fathers still presented ongoing symptoms 5 years after cancer treatment (7). Hence, even if PTSD is less frequent and less severe over time, it is important to know that it can continue for a few years in some parents, and doctors must be able to detect the symptoms and suggest psychotherapeutic intervention, if necessary.
In 21 patients (67.7%), the diagnosis of NF1 was not made at the outset, and 57.1% of these cases had a positive IES-R score. Delayed diagnosis can raise questions, and patients may be tempted to search for further information on the Internet, which is often stressful because people are confronted with anxiogenic information without any sorting, criticism or expertise. Consequently, consulting the Internet was a negative experience for many patients (19/24 thought it was stressful). There are some similar data in the literature showing that the worst presentation of NF1 was regularly described on the Internet (3).
Dermatologists are generally the first physicians to suspect a diagnosis of NF1. Cutaneous manifestations are particularly important because café-au-lait spots, freckling on flexural areas, and cutaneous neurofibromas comprise 3 of the 7 clinical diagnostic criteria. In our study, dermatologists were involved in the diagnosis of NF1 in 58% of cases, which is more often than the involvement of paediatricians, geneticists and general practitioners.
Ablon (3) highlighted that the heterogeneity of NF1 presentations caused fear and anxiety among parents. This result is congruent with our study, as uncertainty was the most cited source of stress in families. Dealing with the reality of this complex and unpredictable disease, the style and circumstances of a physician’s disclosures, and the quality of information, are significantly important. In the case of genetic diseases, the familial issue is central, leading to some guilt for the parents and unfairness for the patient (8, 9); physicians could refer their patients with NF1 to neurofibromatosis clinics for genetic advice.
Guidelines for sensitive disclosure of bad news highlight the systematic planning of a second visit to answer patients’ questions and evaluate their understanding. The next visit should occur soon after the initial disclosure, and the patient may be accompanied for support (10). Patients, and especially parents of children with NF1, may benefit from a post-diagnosis consultation led by a nurse and/or psychologist.
Some study limitations should be considered. A small, heterogeneous sample was investigated. However, the response rate was high considering this is based on postal questionnaires in which response rate is usually approximately 10–20%. While this is a retrospective study, the preliminary monocentric study brings arguments to perform a larger, prospective study. Robust methods for measuring PTSD in larger, prospective studies are still needed to generalize the results. Finally, the people who answered the survey might be the most concerned patients and family members, which might inflate the rate of PTSD. Furthermore, the diagnosis of PTSD was based only on the results of the IES-R score with no clinical examination. We also note that mothers always filled in the survey for their child, yet mothers are at higher risk of PTSD than fathers (11). This selection bias is typically found in self-reported questionnaires.
In conclusion, a high level of PTSD was found following sporadic NF1 disclosure, especially in the parents of children with NF1. Better communication would be possible in order to minimize the post-traumatic stress symptoms in patients and their families if physicians were fully aware of the characteristics of this disease, its evolution and prognosis. Scheduling a second visit, in order to answer patients’ questions and evaluate their understanding, is fundamental in order to discuss psychosocial care.


 Click to show fullsize
Click to show fullsize