


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
A growing body of research has indicated that pruritus is an important feature of hidradenitis suppurativa (HS). This study evaluated pruritus and pain among 103 patients with HS. Pruritus and pain intensity were assessed with a visual analogue scale, numerical rating scale and 4-item Itch Questionnaire. Dermatology Life Quality Index (DLQI) was implemented to assess quality of life (QoL) issues. Various clinical features and factors influencing pruritus were also examined. Pruritus and pain during the last week were reported among 41.7% and 77.5% of patients, respectively. The presence of pruritus did not have an impact on DLQI, nor did it show interaction with the pain in this regard. The presence of pain was a crucial contributor, even more relevant than disease severity. Nonetheless, intensity of pruritus correlated positively with DLQI. The most troublesome symptom of HS was pain, followed by exudation, pruritus, appearance and smell, consecutively. Pruritus of mild-to-moderate intensity is a common HS-associated symptom that adversely affects patients’ QoL.
Key words: hidradenitis suppurativa; acne inversa; pain; pruritus; visual analogue scale; numerical rating scale.
Accepted Oct 2, 2017; Epub ahead of print Oct 3, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Cha?ubi?skiego 1, PL-50-368 Wroc?aw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Hidradenitis suppurativa (HS) is a chronic, inflammatory, debilitating disease of a relapsing nature, predominantly involving nodules, abscesses and suppurating lesions of the apocrine gland-bearing areas of the skin. The estimated prevalence of HS is approximately 1% of the general population, with a predominance amongst women (1). HS is accompanied by physical and psychological symptoms, causing a substantial decline in the quality of life (QoL) of patients. Fever and fatigue are often present in extreme cases and may prevent individuals from performing common everyday tasks (2, 3). The pathogenesis of HS is multifactorial and not fully understood. A growing body of research has focused on the underlying cause and accompanying symptoms of this disease, mainly concerning the problem of pain management.
Recent insight into the histopathological course of events during disease progression has reported an increase in mast cells at all stages of HS (including perilesional skin), accompanying the inflammation of involved skin (4). Mast cells, together with other immune cells infiltrating HS skin, produce and secrete a variety of mediators and pro-inflammatory cytokines. Their peripheral effects are responsible for the signs and symptoms observed in various skin diseases, such as cutaneous swelling and pruritus, which could also be the cause of such symptoms observed among patients with HS. Therefore, this study was undertaken to evaluate both pruritus and pain among patients with HS. Furthermore, it is the one of the first studies to thoroughly describe the clinical characteristics of HS-related pruritus, its frequency and exacerbating factors. A better insight into those accompanying symptoms may help physicians and patients to achieve an improvement in QoL.
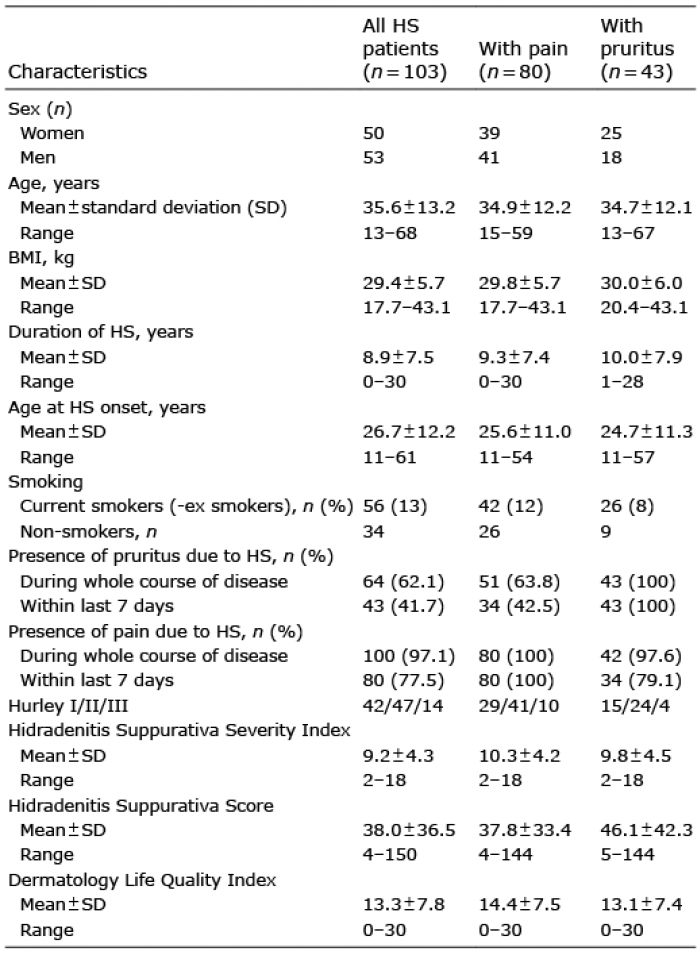
This study was conducted on a group of 103 consecutive patients (50 women, 53 men) age range 13–68 years (mean 35.6 ± 13.2 years) with HS diagnosed in accordance with well-established clinical criteria (5). Disease duration ranged from 0 to 30 years (mean 8.9 ± 7.5 years). The clinical evaluation of disease severity was made according to Hidradenitis Suppurativa Score (HSS), Hidradenitis Suppurativa Severity Index (HSSI) and, additionally, based on the 3-degree scale proposed by Hurley (6–8) (Table I). A mean body mass index (BMI) of 29.4 ± 5.7 kg/m2 qualified the patients as overweight. The rate of active or ex-smokers was 67.0%. All patients with any pruritic/painful skin condition of any type or those receiving any anti-pruritics or pain-killers (e.g. antihistamines, immunomodulators/immunosuppressants, etc. (> 5 half-lives washout period)) were excluded. Individuals who had pruritus or related pain constituted the groups for separate, further analyses, with a more detailed examination of these symptoms.
Table I. Characteristic of hidradenitis suppurativa (HS) patients with pain or pruritus within last 7 days
Pruritus and pain intensity were evaluated using a visual analogue scale (VAS) and numerical rating scale (NRS). Pruritus was additionally assessed with a 4-item Itch Questionnaire (9–11). This instrument was used previously by our group to successfully assess the various types of pruritus (12–14). Dermatology Life Quality Index (DLQI) was also implemented to assess QoL issues.
With regard to VAS, the patients were asked to report and mark on the 10-cm long horizontal line the maximal (VASmax) and mean (VASmean) intensity of pruritus and pain they had experienced from HS lesions during the last 7 days. The same assessment was also conducted with NRS; the participants assessed their pruritus and pain intensity by selecting a number from 0 to 10. The scores for both above-mentioned tools ranged from 0 (no pruritus/pain), to 10 points (worst imaginable pruritus/pain). With reference to VAS scoring, mild (> 0–< 3 points), moderate (≥ 3–< 7 points) and severe or very severe pruritus (≥ 7–10 points) could be distinguished (15). The respective NRS cut-off points for worst (≤ 6; > 6–8; > 8–10) and mean pain (≤ 5; > 5–7; >7–10) were also established (16). The 4-item Itch Questionnaire was used to estimate the extent (1–3 points), intensity (1–5 points), frequency (1–5 points) and sleep disturbances caused by HS-related pruritus (0–6 points) during the 7 days prior to the examination. Rating ranges were from 3 (mild pruritus) to 19 points (very severe pruritus).
Beside of pruritus or pain severity, various clinical features of these symptoms were assessed; including their exact location (for both), pruritus quality and descriptors (itching, burning, prickling, warming, stinging and tingling) and the most common factors responsible for its aggravation or alleviation. The patients were also asked to define the most troublesome symptom of their disease.
The study was approved by the local ethics committee (opinion No. KB-432/2015) and written informed consent was obtained from all individuals studied.
All data were assessed for parametric or non-parametric distribution. Correlations were determined by Pearson’s correlation coefficient or Spearman’s correlation analysis with reference to the distribution of evaluated variables. Differences between groups were determined using the Student’s t-test or the Mann–Whitney U test, where applicable. Multivariate analysis was applied when there were 2 or more dependent variables. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using Statistica 12 software (StatSoft, Tulsa, OK, USA).
Lesion-linked pruritus and pain were reported by the majority of patients during the course of the disease: 62.1% (64/103) and 97.1% (100/103), respectively. Pruritus within the last 7 days before examination was reported by 41.7% (43/103) of patients with HS, whereas pain was reported by 77.5% (80/103) individuals. The distribution of lesions did not differ significantly between the whole group of patients with HS, the subgroup with pruritus or the subgroup experiencing pain. Pruritus severity was assessed as 5.0 ± 2.1 points, 5.5 ± 2.3 points, and 4.6 ± 1.9 points (for VASmax, NRSmax and 4-item Itch Questionnaire, respectively). The pain intensity was evaluated as 7.3 ± 2.4 points (VASmax) and 7.5 ± 2.5 points (NRSmax). The scores for mean pruritus/pain intensity are shown in Table II.
Table II. Maximal and mean intensity of pruritus and pain among studied patients with hidradenitis suppurativa
According to the cut-offs, just over half (51.2%) of patients with HS reported having moderate pruritus, and more (65.0%) reported mild pain (Fig. 1). The pruritus and pain intensity correlated positively with each other (p < 0.01); however, co-occurrence of pruritus and pain in one location at the same time was assessed as 59.5%. Pruritus was observed predominantly in the buttocks area (90% of pruritic lesions) and armpits (83% and 87% of pruritic lesions). Except for the buttocks (82%), pain was distributed quite equally between armpits, inguinal area, abdomen, chest and anogenital area (57–69% of painful lesions for each separate region).
Fig. 1. Hidradenitis suppurativa (HS)-linked pruritus and pain intensity rates among studied individuals. The diagrams were based on cut-offs established for visual analogue scale (VASmean) and numerical rating scale (NRSmean) values for pruritus and pain, respectively.
Surprisingly, multivariate analysis of variance revealed that the presence of pruritus did not have an impact on QoL assessed with DLQI (p = 0.79), nor did it show interaction with the pain in this regard (p = 0.18). The presence of pain was a crucial contributor (p = 0.002), even more relevant than disease severity (p = 0.04). Nonetheless, the pruritus intensity correlated significantly with DLQI (r = 0.45, p = 0.004; r = 0.48, p = 0.002 for VAS and NRS, respectively). Moreover, it is worth noting that patients with Hurley III and active smokers tended to rate their pruritus substantially higher (p > 0.05, detailed data not shown). The pain intensity correlated negatively with QoL, assessed with DLQI, and additionally with disease severity, evaluated with HSS and HSSI (r = 0.48, p < 0.0001; r = 0.3, p = 0.01; r = 0.57, p < 0.0001, respectively (the same values for VAS and NRS)). Such a trend was also observed for Hurley staging (p = 0.05). Of note, patients reporting pruritus or pain had more affected body areas (p = 0.03 and p = 0.04, respectively).
Similar numbers of patients experienced pruritus every day (34.9%), a few times per week (32.6%) or per month (30.2%). Only one patient reported its occurrence less than once per month. Pruritus appeared mostly as short itching episodes of up to 10 min duration (79.1%). The majority of patients described their pruritus as a burning (46.5%) or stinging (25.6%) sensation. Feelings of tickling, tweaking and prickling were less frequent (18.6%, 16.3% and 14.0%, respectively). Excoriations were observed among 6/43 patients (14.0%). Pruritic sensations were usually experienced during the evening (51.2% estimated the occurrence as “frequent” or “permanent”), while during the morning, afternoon or night pruritus of such frequency was reported more rarely (16.3%, 16.3% and 18.6%, respectively). The pruritus was relatively rarely responsible for problems falling asleep and waking during the night; such issues were reported as “permanent” or “almost permanent” for only 1/43 and 5/43 patients with HS, respectively. None of the patients reported the need for hypnotics.
The most common factors exacerbating intensity of pruritus were increased sweating, heat (including hot water exposure) and physical activity. No specific alleviators of pruritus intensity were found (Table III).
Although both pruritus and pain negatively influenced QoL, the pain was reported as the most troublesome symptom of HS, consecutively exceeding exudation, pruritus, appearance and smell. Nonetheless, the pruritus was irritating (62.8%) or burdensome (46.5%) for the majority of patients with HS (16.8% found it unbearable).
Table III. Factors responsible for aggravation or alleviation of hidradenitis suppurativa (HS)-linked pruritus intensity
As pain is reported as the most troublesome symptom of HS, that is most likely why it is also one of the most frequently evaluated subjective symptoms among patients with HS (17). The results of our study have somewhat confirmed this, as the pain evaluated by other groups dealing with HS was of similar frequency and intensity. For instance, it was described as hot, burning, pressure, stretching, cutting, sharp, taut, splitting, gnawing, sore, throbbing, and aching, and scored 3.6 ± 3.2 points (NRS) (18) and 4.5 ± 2.4 (VAS) (19). Moreover, it was also positively correlated with DLQI and various scoring systems of disease severity, including HSS (6) or HSSI (7). Our study, additionally focused on pain distribution, showed no dependence with its location.
Of many subjective symptoms accompanying HS, pruritus seems to be one of the most overlooked/under-appreciated. However, HS is not usually considered a pruritic disease, although pruritus is often mentioned as a symptom associated with it, mainly in its prodromal stage (20–24). The importance of pruritus as an initial symptom of HS has been emphasized in a recent study by Ring et al. (22). Unexpectedly, it was found that the rate of pruritus (as well as dysaesthesia) as a prodrome was even higher than in patients with herpes zoster. Importantly, in the questionnaire used, “itching” was not mentioned as one of the predetermined options; it was disclosed only if patients answered the item “other symptoms” and wrote “itching” in response. The authors, therefore, expected even higher rates of this symptom. This finding can be regarded as clinical proof of the results of studies by Dutch researchers (4, 25), who demonstrated an increased presence of mast cells and inflammatory cell infiltration in HS lesions of all stages, as well as in perilesional skin in both acute and chronic phases of the disease. This may suggest that these cells are also important in the initial, subclinical phase of HS pathogenesis. In other research, by Esmann et al. (24), the patients reported pruritus as one of the causes of the disease’s negative psychosocial impact, resulting in a reduction in QoL. In a recent large survey-study, involving 421 patients with HS, it was demonstrated that pruritus of significant intensity (mean VAS 3.7 ± 3.2) was a predictive factor for low EQ-5D index values (26).
Nonetheless, to the best of our knowledge, our current study is the one of the first to define the clinical characteristic of pruritus in patients with HS. The results of our study were similar to those presented by Riis et al. (26), showing that pruritus in HS is mostly of mild to moderate intensity. Moreover, it was concurrent with the study by Vossen et al. (25) with regard to many aspects, including pruritus intensity (mean NRS score 5.4 ± 2.5 for patients reporting any pruritus), correlation with pain intensity, number of affected areas, Hurley III and smoking dependence. They, however, reported a higher prevalence (67.3%).
What is interesting, both the intensity of pruritus, as well as pain, were connected with decreased QoL as assessed by DLQI. The results of our study, however, showed an important difference between those 2 symptoms. Primarily, the pain presence was the main and only contributor for decreased QoL (except for disease severity). Furthermore, we did not find a correlation between pruritus intensity and disease severity as we did with respect to pain. It was, therefore, not surprising that patients with HS reported that pain was the most troublesome symptom of disease. The predominance of pain accompanying fully developed lesions might explain pruritus as being just the initial symptom of HS flares. This could also be the reason for discordant co-occurrence of pain and pruritus in one location at the same time (< 60%). Although, analysing our results, it seems that the major deficiency of the study is the lack of evaluation of pruritus with regard to disease flares. Based on our patients’ reports, sweat was the most frequent aggravating factor of pruritus. Similar results were also found among the patients with atopic dermatitis (27) and pruritus ani (28).
The most probable explanation of the presence of pruritus in HS is the inflammation of the involved skin, including perineural infiltrate, with a subsequent cascade of released mediators, hence the results of the above-cited studies by the group of van der Zee (4, 25). It should also be mentioned that pruritus may be an adverse effect of the therapy as some of the frequently used agents, such as acitretin or topical clindamycin, are also known instigators of pruritus.
In conclusion, both pain and pruritus seem to be important symptoms negatively influencing the well-being of patients with HS. Despite the high frequency of those symptoms associated with the disease, HS has been essentially ignored in pain and pruritus medicine literature. Although published data are scarce, based on Horváth et al.’s (29) study it should be highlighted that both anticonvulsants and selective serotonin reuptake inhibitors/serotonin-norepinephrine reuptake inhibitors, present neuropathic pain-relieving properties. These properties offer not only control of HS-associated pain, but also have a beneficial effect on pruritus and depression. It is hoped that greater knowledge of the pathophysiology and potential treatment options available for HS, may help put pain and pruritus specialists in a better position to contribute to the overall care of patients.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize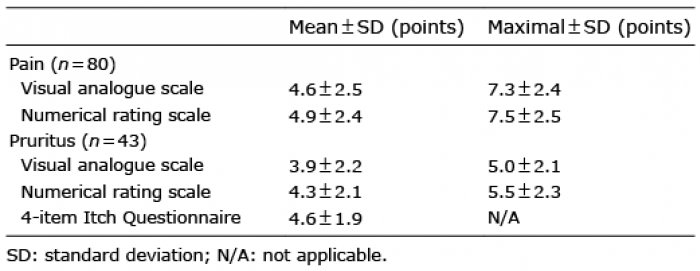 Click to show fullsize
Click to show fullsize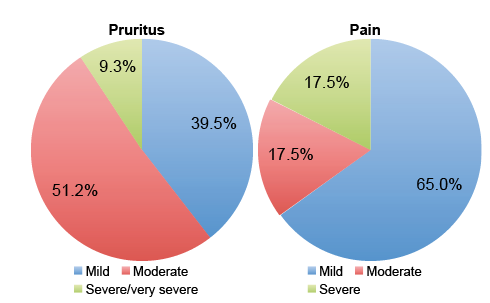 Click to show fullsize
Click to show fullsize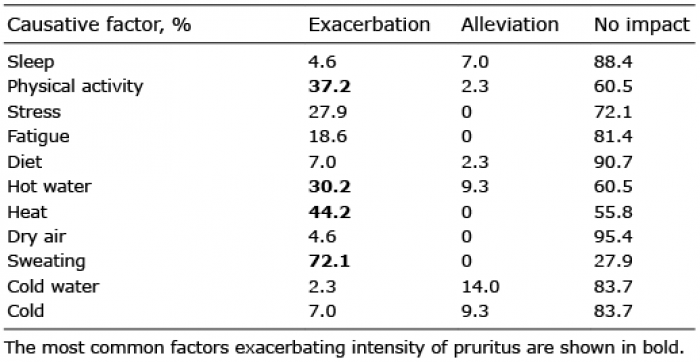 Click to show fullsize
Click to show fullsize