


Pediatric Dermatology Unit, Department of Medicine DIMED, University of Padova, Via Gallucci, 4, IT-35128 Padova, Italy. *E-mail: anna.bellonifortina@gmail.com
Accepted Oct 16, 2017; Epub ahead of print Oct 19, 2017
Psoriasis is a chronic inflammatory disease that affects up to 1.37% of children in Europe (1). Recent studies report that, not only in adults, but also in children, psoriasis may be associated with certain morbidities, including obesity, hypertension, dyslipidemia, diabetes mellitus, metabolic syndrome (2–8). Most of these studies, however, have been designed as multicenter studies, and thus may have limitations because of the inter-institution variations in data-collecting methodologies, data interpretation, different populations studied or limited number of patients investigated.
We performed a single-centre study, investigating the association between psoriasis and body mass index (BMI) and central obesity (waist-to-height ratio; WHtR) in 107 children with psoriasis and 107 age- and sex-matched controls.
From 2013 to 2016 a single-centre, cross-sectional study of 107 consecutive children with psoriasis (mean age 9.94 ± 3.48 years) and 107 age- and sex-matched children without psoriasis (control group) was performed at the Pediatric Dermatology Unit, Padua University, Padua, Italy.
The children in the control group were recruited from among children consecutively attending the Pediatric Dermatology clinic for non-inflammatory diseases (i.e. warts, naevi, moles, etc.). Children with and without psoriasis were from the same geographical area, with similar demographic characteristics and, presumably, similar lifestyles. The following data were collected for each patient: physical examination, height, body weight, BMI, WHtR, duration and family history of psoriasis.
Psoriasis severity was classified as mild or moderate-to-severe according to Psoriasis Area Severity Index (PASI) and body surface area (BSA). When PASI was ≥ 10 and/or BSA was > 10% psoriasis was designated as moderate-to-severe (8).
BMI (in kg/m2) allowed us to classify children as normal weight (< 85th and > 5th percentile), overweight (≥ 85th and < 95th percentile) or obese (≥ 95th percentile) (9).
Waist circumference (WC) was measured twice, midway between the lowest border of the rib cage and the upper border of the iliac crest, at the end of normal expiration, using inextensible anthropometric tape with the patients standing erect and relaxed with arms at their sides and feet positioned close together. The mean values were considered for analysis. Evaluation of central obesity was performed using WHtR, calculated as WC (in cm) divided by height (in cm). Patients with a WHtR ≥ 0.5 were classified as having central obesity (8).
Descriptive statistics are presented as counts and percentages for categorical variables and mean ± standard deviation (SD) for continuous data. The distribution of continuous variables was tested for normality using the Kolmogorov–Smirnov test. The χ2 test and Fisher’s exact test were used to compare categorical variables and the Student’s t-test or Mann–Whitney U test to compare continuous variables between groups. Odds ratios (OR) and the corresponding 95% confidence intervals (95% CI) were estimated. The independent associations between disease status (patients with psoriasis and those without) and the clinical and analytical variables were assessed using multivariable logistic regression models. The level of statistical significance was set at α = 0.05. Data were collected in a database using Microsoft Excel 2016 for Windows 10 and statistical analyses were performed with SPSS version 23.0 (Statistical Package for Social Science Inc., Chicago, IL, USA) for Microsoft Windows 10.
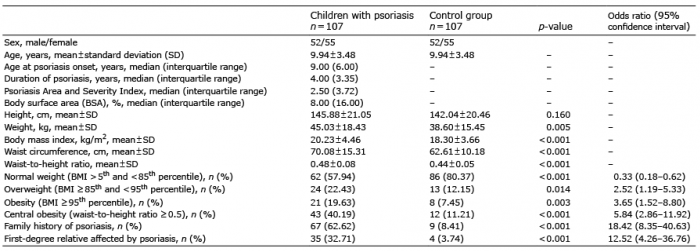
Demographic data are shown in Table I. A family history of psoriasis was present in 67 out of 107 (62.62%) children, of whom 35 (32.71%) reported that first-degree parents were affected. Paternal imprinting was found in 37.38% children with psoriasis; maternal imprinting was found in 20.56% children with psoriasis (p < 0.001).
Table I. Demographic, anthropometric and clinical data of children with psoriasis and control group
Children with psoriasis, compared with those without, had a higher prevalence of family history of psoriasis (62.62% vs. 8.41%; p < 0.001). The median age of psoriasis onset was 9.00 years, median psoriasis duration 4.00 years, median PASI 2.50, and median BSA 8.00%.
Children with psoriasis, compared with children without, had a higher prevalence of overweight (BMI ≥ 85th and < 95th percentile; OR 2.52; 95% CI 1.19–5.33; p = 0.014), obesity (BMI ≥ 95th percentile; OR 3.65; 95% CI 1.52–8.80; p = 0.003), overweight/obesity (OR 3.16; 95% CI 1.70–5.87; p < 0.001) and central obesity (WHtR ≥ 0.5) (OR 5.84; 95% CI 2.86–11.92; p < 0.001).
Overweight/obese children with psoriasis, compared with overweight/obese children without, had a higher prevalence of central obesity (OR 5.74; 95% CI 1.81–18.20; p = 0.002). Normal-weight children with psoriasis, compared with normal-weight children without, had a higher prevalence of central obesity (OR 3.66; 95% CI 1.30–10.25; p = 0.010). Multivariate analysis showed that only central obesity was independently associated with psoriasis (OR 3.20; 95% CI 1.40–7.30; p = 0.006).
Central obesity was associated with duration of psoriasis (p = 0.043). Multivariate analysis revealed the independent association between central obesity and duration of psoriasis (p = 0.021). In particular, central obesity increased by 18% for each year of disease duration (OR = 1.18) (Table SI).
Children with moderate-to-severe psoriasis, compared with children with mild psoriasis, presented no statistically significant difference in the age of onset of psoriasis, overweight, obesity, or central obesity (p = 0.885; p = 0.290; p = 0.508; p = 0.329).
Children with psoriasis in this study had a significantly greater prevalence of excess of adiposity and central obesity than children without, using both BMI (OR 3.16; 1.70–5.87) and WHtR (OR 5.84; 2.86–11.92). Since BMI and WHtR are markedly influenced by the age of patients, we carefully matched the patients with psoriasis with a control group of the same age.
Our findings are in accordance with previous studies. However, multivariate analysis showed that only central obesity (WHtR ≥ 0.5) was independently associated with psoriasis (OR 3.20; 1.40–7.30), in accordance with some recent studies (7, 8).
BMI percentile remains the standard method for identifying overweight and obese children, but WHtR identifies children with central obesity and is considered a better indicator of metabolic risk than BMI (8, 10). The importance of WHtR parameter was highlighted in a large prospective study of children (10). This study showed that WHtR ≥ 0.5 in childhood was associated with an increased cardio-metabolic risk later in life, with children with WHtR ≥ 0.5 2–5 times more likely to have cardio-metabolic risk factors.
In fact, we found that normal weight children with psoriasis also had a higher prevalence of central obesity (OR 3.66; 1.30–10.25) than normal weight children without, as reported recently in a multicentre Australian study (8).
Central obesity (WHtR ≥ 0.5) was associated with duration of psoriasis; central obesity increasing 18% for each year of disease duration (OR 1.18; 1.03–1.36).
This finding is in contrast with the multicentre study of Paller et al. (7), in which no correlation between psoriasis duration and central obesity was reported.
On the other hand, in adult patients with psoriasis, some studies found a correlation between duration of psoriasis and prevalence of metabolic syndrome (2, 11), and metabolic syndrome is strongly related to central obesity.
In conclusion, these data confirm the association between psoriasis and central obesity in children reported in other multicentre studies, and emphasize the importance of careful assessment of comorbidities in children with psoriasis.
Funding sources: Supported in part by University of Padua under Project CAEPAE.


 Click to show fullsize
Click to show fullsize