


1Department of Dermatology, Hokkaido University Graduate School of Medicine, North 15 West 7, Kita-ku, Sapporo 060-8638, 2Hamasaka Skin Clinic, and 3Sapporo Institute of Dermatopathology, Sapporo, Japan. *E-mail: h-ujiie@med.hokudai.ac.jp
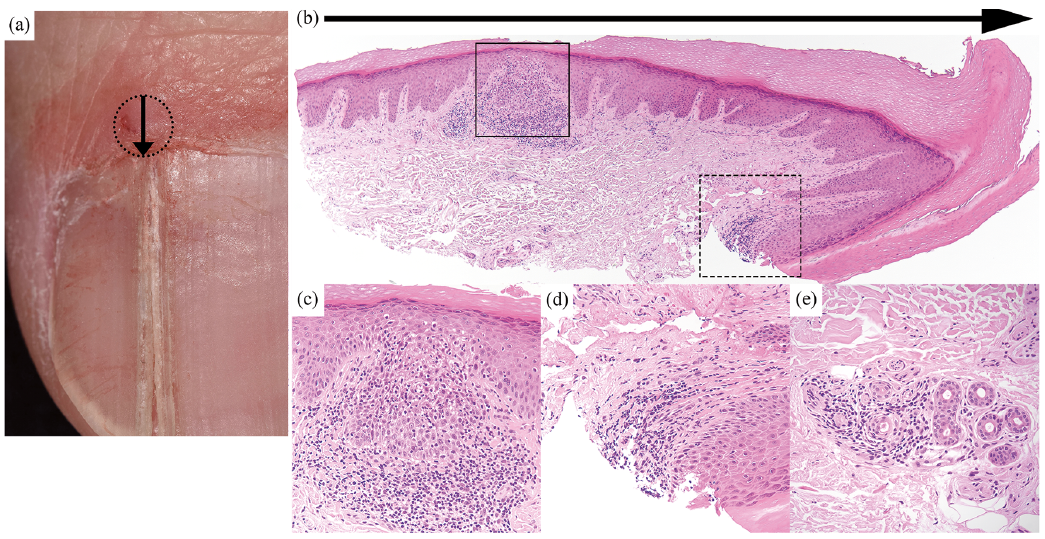
A 38-year-old man presented with a split right thumbnail. He had noticed the nail change 6 months earlier. Physical examination revealed a longitudinal split of the right thumbnail, accompanied by a skin-coloured papule on the proximal nail fold (Fig. 1a). It was initially suspected that a mucous cyst on the proximal nail fold had caused the nail change. The papule was punctured with an 18-gauge needle, but no mucous fluid was observed. A biopsy specimen of the papule on the proximal nail fold showed superficial perivascular lymphocytic inflammatory infiltrates with a focal lichenoid pattern at the dermal–epidermal junction and mild spongiosis with a few necrotic keratinocytes in the epidermis (Fig. 1a–c). In addition, similar lymphocytic infiltrates were observed around the nail matrix (Fig. 1d). Notably, the eccrine glands and ducts were also involved (Fig. 1e).
What is your diagnosis? See next page for answer.
Fig. 1. Clinical presentation: a longitudinal split of the right thumbnail with a skin-coloured papule on the proximal nail fold. (a) Dotted circle indicates the biopsy site on the papule of the proximal nail fold. Arrow represents the longitudinal section. Histopathology of the proximal nail fold and around the nail matrix. (b) The dense lymphocytic infiltration in the proximal nail fold (square) and around the nail matrix (dotted square) (haematoxylin and eosin staining, original magnification ×40). (c) Focal perivascular lymphocytic infiltrates and mild spongiosis with a few necrotic keratinocytes (original magnification ×200, corresponding to the square in Fig. 1b). (d) Lymphocytic infiltrates around the nail matrix (original magnification ×200, corresponding to the dotted square). (e) Eccrine gland involvement in another section (original magnification ×200).
Acta Derm Venereol 2017; XX: XX–XX.
Diagnosis: Nail lichen striatus
Nail changes are important indicators of various diseases and can sometimes be a diagnostic key (1). A nail split is caused by proximal nail matrix damage from trauma or physical pressure by tumours, such as glomus tumours (2, 3). Inflammation of the nail matrix can also result in a nail split (4).
Lichen striatus is an uncommon self-limited inflammatory dermatosis, which follows the Blaschko line (5). The lesions usually appear on the arms, legs and trunk, but the change may involve any site, such as the face. Nail involvement is rare. A study of 115 children with lichen striatus showed only 3 cases with nail changes (6). Although nail lichen striatus usually affects both nail and skin, 3 cases of lichen striatus limited to the nail have been reported (7). Nail abnormalities in lichen striatus are similar to those in lichen planus, presenting longitudinal ridging, splitting, onycholysis, nail pitting and/or shredding. Of these, a longitudinal nail split is the most common in nail lichen striatus (8). Whereas nail lichen planus damages the nails permanently (9), the nail changes of lichen striatus can resolve spontaneously (8).
The histopathological characteristics of nail lichen striatus resemble those of skin lichen striatus (7). In both, superficial and deep perivascular lymphocytic infiltrates, mild spongiosis with a few necrotic keratinocytes in the epidermis, hyperkeratosis and parakeratosis are diagnostic features (7, 8). In addition, eccrine extension of the infiltrates is a clue to diagnosis (10).
In the current case, a diagnosis of nail lichen striatus was made based on the clinical presentation of longitudinal nail split and the histopathological findings. The nail change has gradually improved with topical difluprednate ointment. In cases of longitudinal nail split, nail lichen striatus should be considered as a differential diagnosis.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize