


1Department of Dermatology, 3Department of Internal Medicine, 4Department of Gastroenterology and Alimentary Tract Surgery, Tampere University Hospital, 2Faculty of Medicine and Life Sciences, and 5Faculty of Social Sciences, University of Tampere, Tampere, Finland
Dermatitis herpetiformis (DH) is an extra-intestinal manifestation of coeliac disease. The highest currently reported prevalence of DH is in Finland, but knowledge of diagnostic delay is limited. This study investigated the duration of rash prior to diagnosis in 446 patients with DH, analysing the results in 3 periods of 15 years. The diagnosis was considered delayed when the duration of rash before diagnosis was 2 years or longer. Factors associated with delayed diagnosis were analysed. Within the 45 years, the median duration of rash before diagnosis decreased significantly, from 12.0 to 8.0 months (p = 0.002) and the occurrence of a delayed diagnosis decreased from 47% to 25% (p = 0.002). Female sex, the presence of villous atrophy, and a diagnosis of DH before the year 2000 were significantly associated with delayed diagnosis. In conclusion, the present study showed that one-quarter of patients currently have a diagnostic delay of 2 years or more, which is far from ideal.
Key words: dermatitis herpetiformis; coeliac disease; diagnostic delay; gluten-free diet; dapsone.
Accepted Oct 16, 2017; Epub ahead of print Oct 19, 2017
Acta Derm Venereol 2017; XX: XX–XX.
Corr: Kaisa Hervonen, Department of Dermatology, Tampere University Hospital, PO Box 2000, FIN-33521 Tampere, Finland. E-mail: kaisa.hervonen@staff.uta.fi
Dermatitis herpetiformis (DH) is a cutaneous manifestation of coeliac disease presenting as an itchy polymorphic blistering rash on the elbows, knees, buttocks and scalp (1). Diagnosis of DH is based on the presence of typical skin symptoms and the demonstration of IgA in the papillary dermis during direct immunofluorescence examination (2). Although 75% of patients with DH have small bowel mucosal villous atrophy at diagnosis, only a minority have marked gastro-intestinal symptoms (3, 4). The treatment of DH is a lifelong gluten-free diet (GFD), similar to treatment of coeliac disease (4, 5). A GFD results in healing of the enteropathy and the rash, but the rash alleviates slowly and additional treatment with dapsone (4,4’-diaminodiphenylsulfone) is frequently needed at the start of dietary treatment (6, 7).
DH is considered relatively uncommon, having the highest reported prevalence of 75.3 per 100,000 people in Finland and a lower prevalence in UK and the USA (8–10). In contrast to the established increase in the incidence of coeliac disease, the incidence of DH decreased in both Finland and UK during the 1990s (8, 9). DH constitutes a diagnostic challenge to general practitioners and other non-dermatologists, and can easily be misdiagnosed as other itchy or blistering skin diseases (11, 12). Early diagnosis is warranted in DH, since ongoing symptoms reduce quality of life, and undiagnosed DH predisposes to complications, such as lymphoma and low bone mineral density (13–15).
For coeliac disease, the median time from onset of gastro-intestinal symptoms to diagnosis in Finland is currently 3 years (16). Fortunately, diagnostic delay has decreased over the past decades in Finland, other European countries, and the USA (17–20). However, up-to-date knowledge about diagnostic delay in DH is lacking. The aim of this study was to investigate the changes in the diagnostic delay in DH and to analyse possible factors associated with delayed diagnosis. Our prospectively collected large DH cohort enabled us to perform delay analyses for 3 periods of 15 years.
All patients suspected of having DH in the Tampere region, Finland, are referred by private dermatologists and general practitioners working in healthcare centres to the Department of Dermatology, Tampere University Hospital, for confirmation of DH diagnosis. Clinical suspicion of DH is an adequate reason for referral regardless of coeliac autoantibody result, and the referral policy for DH has remained the same for the years of the present study. In Tampere University Hospital, diagnosis of DH is based on the detection of typical clinical symptoms and the presence of granular IgA deposits in the papillary dermis (2), and this diagnostic procedure has remained unchanged during the study period. All patients are treated at a special DH clinic, where they are advised to adhere to a lifelong GFD.
Our DH cohort consists of 512 patients who had been diagnosed and treated at the DH clinic between 1970 and 2014. A total of 446 patients were included for further analysis. Of the 66 patients excluded, 10 did not have IgA deposits in the skin, 21 had died over 20 years previously and their data was not available, and 35 had a previous diagnosis of coeliac disease. Data on the duration of the rash before diagnosis were collected from medical records held at Tampere University Hospital. The diagnosis was considered delayed when the duration of the rash before diagnosis was 2 years or more. The definition for delayed diagnosis was based on a previous study performed in our hospital district (21) and clinical experience. In December 2015, a special questionnaire that included questions about the duration of the rash, presence of gastrointestinal symptoms before the diagnosis and the occurrence of malignancies and fractures was sent to all 413 surviving patients with DH. A total of 237 (56%) patients responded, and 217 were included in the analysis of gastrointestinal symptoms. Self-reported bone fractures and malignancies were recorded from questionnaires. Excessive-trauma fractures (the trauma causing the fracture considered sufficient to cause a bone fracture for any person) and stress fractures were excluded from further bone fracture analyses, and non-melanoma skin cancers were excluded from further malignancy analyses.
The severity of the rash at DH diagnosis was collected from medical records and scored as mild, moderate, or severe according to the presence of a few, several, or many blisters; macular eruptions; and erosions on the knees, elbows, buttocks, scalp, or elsewhere on the body. Small bowel biopsy results at diagnosis collected from medical records were graded by experienced pa-thologists as subtotal villous atrophy (SVA), partial villous atrophy (PVA), or normal mucosa (22).
The results of reticulin and/or endomysium autoantibodies at diagnosis were collected from medical records and categorized as positive or negative.
The study protocol was approved by the Ethics Committee of Pirkanmaa Hospital District (R15143). Informed consent was obtained from each study participant responding to the questionnaire.
For the descriptive statistics and further analysis, the patients were grouped into three 15-year periods according to the year of their DH diagnosis: 1970−1984, 1985−1999, and 2000−2014. Diagnostic delay was expressed as the median with lower and upper quartiles (Q1−Q3), and also as mean, in order to be able to compare it with previous studies. The 2-sided χ2 test, Fisher’s exact test, and the Kruskal–Wallis test were used for verifying the relationship between the year of diagnosis of DH, diagnostic delay, severity of rash, and gastro-intestinal symptoms. The significance level was set at ≤ 0.05.
To identify factors associated with delayed diagnosis, binary logistic regression analysis was used. Univariate analysis was used at first for each associating factor, then multivariable analysis was used for detecting the independence of delay-associated parameters found in the univariate analysis. In the multivariable analysis, sex, age at diagnosis, calendar period of diagnosis, severity of rash, presence of gastrointestinal symptoms, and small bowel biopsy findings at diagnosis were all taken into consideration. Associations are expressed in terms of odds ratios (OR) with 95% confidence intervals. To determine whether the patients with delayed diagnosis developed more bone fractures or malignancies, Pearson χ2 test and Fisher’s 2-sided exact test were used. A p-value ≤ 0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics for Windows (Version 23.0. Armonk, NY: IBM Corp.).
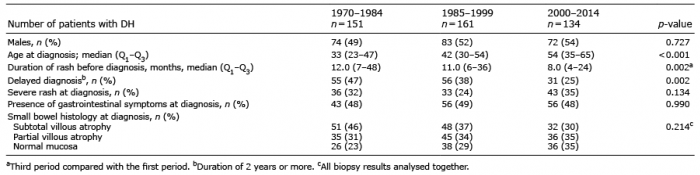
Of the 446 patients with DH, 229 (51%) were males. Mean age at diagnosis was 43 (range 3–83) years. The number of patients with DH diagnosed within the three 15-year periods was 151 in 1970−1984, 161 in 1985−1999, and 134 in 2000−2014 (Table I). As already reported in our previous study (8), the median age at diagnosis increased significantly (p < 0.001), from 33 years in the first study period to 54 years in the third study period.
Table I. Demography, duration of rash, delayed diagnosis, and small bowel biopsy findings in the three 15-year periods in 446 patients with dermatitis herpetiformis (DH)
During the entire study period, the median duration of the rash before diagnosis was 10 months and the mean was 3.1 years. The median duration of the rash decreased significantly from 12.0 to 11.0 and then to 8.0 months (p = 0.002) during the three 15-year periods, respectively (Fig. 1); statistical significance was found when the first and third period were compared (Table I). The corresponding mean values were 37 (range 0.1–240), 43 (0.1–528), and 34 (1–480) months, respectively.
Fig. 1. Duration of rash before diagnosis in patients with dermatitis herpetiformis (DH) in the three 15-year diagnostic periods. The lower and upper limits of the boxes indicate the 25% and 75% confidence intervals and the black bars indicate median values. The whiskers extend to 1.5 times the height of the box and the circles are outliers that exceeded the interquartile range ± 1.5 times, The asterisk is an extreme outlier that exceeded the interquartile range +3 times.
The rash was severe at diagnosis in 112 (29%) of the 386 patients, and 89 out of 217 (41%) reported having had gastrointestinal symptoms at diagnosis. There was no difference in the occurrence of severe rash or gastrointestinal symptoms at diagnosis during the 3 study periods (Table I). The small bowel biopsy result was available for 347 (78%) patients, of whom 131 (38%) had SVA, 116 (33%) PVA, and 100 (29%) normal mucosal morphology (Table I). Overall, there was no statistically significant change in the three 15-year periods; however, a decreasing trend was seen in the occurrence of SVA and there was a concomitant increasing trend in normal villous architecture.
Of the 446 patients in the study, 389 (87%) had sufficient information for the analysis of factors associated with the delayed diagnosis (Table II). Altogether, 142 (37%) patients had a delayed diagnosis, i.e. time from onset of rash to diagnosis was 2 years or more. The percentages in the 3 study periods were 47%, 38% and 25%, respectively (Table I).
Table II. Associations between clinical characteristics, time of diagnosis, and delayed diagnosisa in 389 patients with dermatitis herpetiformis
Female sex (OR 1.5) was significantly (p = 0.043) associated with delayed diagnosis in the univariate analysis, but not in multivariable analysis (p = 0.061, Table II). Age at diagnosis was not associated with the delay. DH diagnosis performed during the first study period was significantly associated with delayed diagnosis, both in the univariate (OR 2.62, p = 0.001) and multivariable (OR 2.32, p = 0.017) analyses (Table II). The severity of rash or presence of gastrointestinal symptoms at diagnosis was not connected with delayed diagnosis. By contrast, villous atrophy (subtotal or partial) at diagnosis was significantly associated with diagnostic delay, both in the univariate (OR 2.70, p = 0.001) and multivariable (OR 2.52, p = 0.003) analyses. Furthermore, the positivity of coeliac autoantibodies (reticulin and/or endomysium) was significantly associated with diagnostic delay in the univariate analysis (OR 2.63, p = 0.001) in the 250 patients with available autoantibody results.
The patients with delayed diagnosis did not develop more bone fractures (17.6%) than those without long delay in diagnosis (14.3%) (p = 0.523), nor did they develop more malignancies (7.4% vs. 6.0% respectively; p = 0.765).
This long-term study of DH patients diagnosed between 1970 and 2014 analysed time tendencies from the onset of the rash to diagnosis. In the three 15-year study periods, the median durations of rash before diagnosis were 12, 11 and 8 months, respectively. Importantly, the rash duration in the third and latest period was significantly shorter than in the first period. One reason for this seems to be better awareness of the disease due to nationwide guidelines for the diagnosis and treatment of coeliac disease in Finland, which were published in 1997 and are updated regularly (23). General practitioners and other physicians can access these guidelines online, and they also include DH, with clinical pictures of the rash and recommendations on how and where to diagnose patients.
Similarly to DH, the diagnostic delay for coeliac disease became shorter in Finland after the publication of the Current Care Guidelines (17). However, it is noteworthy that the diagnostic delay in coeliac disease is still much longer than in DH; in approximately one-third of Finnish patients with coeliac disease (17) and DH, there are delays of over 10 and 2 years, respectively.
The present DH cohort of 446 patients showed that the mean time from the first symptoms of rash to diagnosis was 3.1 years. Two previous DH studies with a smaller number of patients, one from Ireland (24) and another from Germany (25), documented a shorter (1.6 years) or similar (3.2 years) duration to diagnosis, respectively (Table III). By comparison, a recent Swiss study showed that, in bullous pemphigoid, the mean time from the first symptoms to diagnosis was much shorter (6.1 months) (26). It is clear that the blistering rash with accompanying intense itch in DH means that there is usually little delay before the patient contacts a physician. When DH is suspected, the patient is sent directly to our University Hospital for a final diagnosis. It is, however, noteworthy that the time needed for diagnosis can vary greatly among patients with DH. In the present study, the range was from 0.1 to 44 years, and in the 2 previous DH studies, the longest durations were 4 and 20 years, respectively (24, 25).
Table III. Time from the onset of symptoms to diagnosis in dermatitis herpetiformis (DH) and coeliac disease (CD) in the present and previous studies
In contrast to DH, the delay in diagnosis of coeliac disease has received much attention in recent years. The diagnostic delay for coeliac disease in hospital cohorts and questionnaire studies has been reported to be very long, from 3 to 11 years (Table III) (16, 19, 20, 27–29). Consuming a gluten-containing diet for such a long time may increase the risk of developing DH, which is the most common extra-intestinal manifestation of coeliac disease (1, 30). An important issue is how long the patients with DH have had preceding undiagnosed coeliac disease in the small bowel. The time period can be very long (up to 30 years), as shown by studies reporting a phenotype change from partially GFD-treated coeliac disease to DH (31, 32). Moreover, coeliac-type dental enamel defects observed in adults with DH suggest that undiagnosed coeliac disease had been present in childhood in many of the patients (33).
Small bowel mucosal damage in patients with DH ranges from severe, to partial villous atrophy, to normal villous structure with coeliac-type inflammatory changes (22). The present study analysed whether the small bowel damage could be linked to the delay in diagnosis of DH. It was found that the patients with villous atrophy significantly more often had a long diagnostic delay than those with normal villous mucosa. Villous atrophy can be a result rather than a cause of delayed diagnosis; after initial onset of gluten intolerance, it can take a long time before villous atrophy develops in coeliac disease (34, 35). Therefore, patients with DH who have undamaged villous morphology could be in the early stages of this process. Similarly, we found that the patients with positive coeliac autoantibodies significantly more often had a delayed diagnosis than those with negative autoantibodies, which probably reflects the same thing; since the diagnosis becomes delayed the autoantibody response has time to progress.
Several studies of coeliac disease have shown that females have a longer diagnostic delay than males (17, 20, 29). Similarly, in the univariate statistical analysis of the present DH study, females significantly more often had a delayed diagnosis than did males. Irritable bowel syndrome is common in females, and may mask the diagnosis of coeliac disease (20). Patients with DH rarely have obvious gastrointestinal symptoms, and the rash with intense itch is the reason for seeking medical advice. Therefore, the reasons why females seem to have delayed diagnosis in both coeliac disease and DH compared with males remain unknown.
Untreated DH has shown to decrease patients’ quality of life, which improves along with GFD treatment after diagnosis (13). The current study did not detect association with delayed diagnosis and development of bone fractures or malignancies, but the burden and complications related to delayed diagnosis of DH are yet to be fully elucidated.
The main strengths of the present study were the large patient cohort, collected from 1970 onwards at the single DH clinic. The diagnosis was invariably based on the presence of granular IgA deposits in the papillary dermis (2). Two experienced dermatologists have treated almost all of the present patients with DH, making notes on the presence of the rash at the time of diagnosis. In addition, small bowel biopsy results were available for the majority of patients, since endoscopy with small bowel biopsy has been performed routinely for all newly diagnosed patients with DH (22). The main limitations were the retrospective study design and a rather low response rate to the questionnaire. However, the data on the duration of the rash before the diagnosis was retrieved primarily from the patients’ medical records, and only the data on the presence of gastrointestinal symptoms was derived from the questionnaires. A further limitation is that the threshold of 2 years or more for delayed diagnosis is somewhat arbitrary; however, it is partially based on our previous study in which the median duration of rash before diagnosis was 9 months in patients with refractory DH and 12 months in control patients with DH (21). In addition, from a clinical point of view, we consider a diagnostic delay of 2 years or more with itchy rash to be far too long.
In conclusion, the present long-term study showed that one-third of patients had a diagnostic delay of at least 2 years. Female sex, villous atrophy at diagnosis, and a DH diagnosis before the year 2000 were significantly associated with delayed diagnosis. Even though the situation has improved over the past 45 years, the diagnostic delay is still unacceptably high for a country with such a high prevalence of the disorder.
The study was financially supported by the Finnish Coeliac Society, the Finnish Medical Foundation, the Competitive State Research Financing of the Expert Area of Tampere University Hospital (grants 9T018, 9T058, 9U019, 9T004), the Sigrid Juselius Foundation, and the Academy of Finland.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize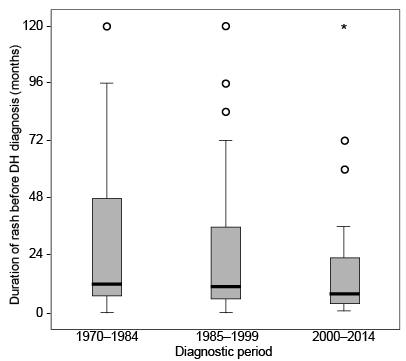 Click to show fullsize
Click to show fullsize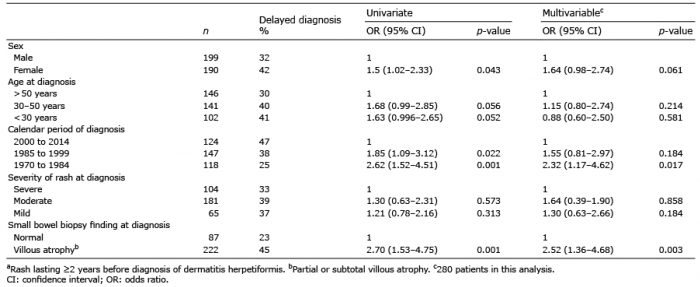 Click to show fullsize
Click to show fullsize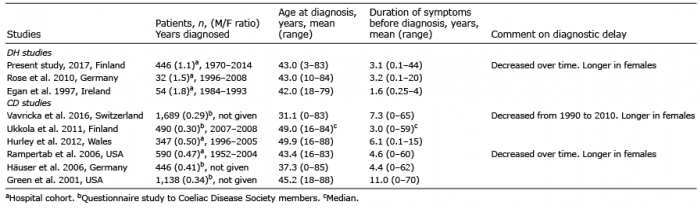 Click to show fullsize
Click to show fullsize