


1Department of Dermatology, Medical University of Vienna, and 2Department of Clinical Psychology, General Hospital of Vienna, Vienna, Austria
The Revised Illness Perception Questionnaire (IPQ-R) has been shown to assess illness perception reproducibly in primary cutaneous T-cell lymphomas (CTCL). Illness perception reflects patients’ individual concepts of understanding and interpretation of the disease, influencing illness behaviour and health-related quality of life (HRQOL). This study investigated the clinical relevance of the relationships between illness perception, illness behaviour, and HRQOL in CTCL and cutaneous B-cell lymphomas (CBCL). A total of 92 patients completed the IPQ-R, the Scale for the Assessment of Illness Behavior (SAIB), and a skin-specific HRQOL tool (Skindex-29). Data on illness behaviour were not evidently related to illness perception, whereas illness perception was significantly associated with HRQOL. Both, IPQ-R and HRQOL results correlated with disease entity, stage, and socio-demographics. Only IPQ-R results provided practical information on patients’ needs to train personal coping strategies. IPQ-R assessment in CTCL and CBCL might be a useful instrument to improve individual disease management.
Key words: illness perception; HRQOL; illness behaviour; individual disease management; coping strategies.
Accepted Oct 16, 2017; Epub ahead of print Oct 19, 2017
Acta Derm Venereol 2017; XX: XX–XX.
Corr: Constanze Jonak, Department of Dermatology, Medical University of Vienna, Waehringer Guertel 18–20, AT-1090 Vienna, Austria. E-mail: constanze.jonak@meduniwien.ac.at
Leventhal’s Common Sense Model of Illness Cognition proposes individual, mental concepts of perceiving and responding towards one’s illness. Herein, cognitive and emotional coping strategies are self-regulatory and based on patients’ illness perception (1–3). Thus, illness behaviour is the conceptual model for handling one’s state of health as a patient perceives, evaluates, and acts upon disease-related symptoms (4, 5).
Both illness perception and illness behaviour affect personal disease management and health-related quality of life (HRQOL) (6–8). In cancer patients, HRQOL is influenced by the way patients perceive and respond to their illness (9).
Consequently, we aimed to investigate the clinical value of the conceptual relationships between illness perception, illness behaviour, and HRQOL in primary cutaneous lymphomas (CLs). CLs are either of T-cell (CTCL) or B-cell (CBCL) origin and mostly follow an indolent course (e.g. CBCL or early-stage CTCL). However, prognosis is poor in advanced-stage CTCL mycosis fungoides (MF) and Sézary syndrome (SS) (10–13).
To date, HRQOL and illness perception, but not illness behaviour, have been assessed in CLs demonstrating mental burden due to this stigmatizing skin disorder (14–17). Within our questionnaire-based study the HRQOL tool Skindex-29, the revised Illness Perception Questionnaire (IPQ-R), and the Scale for the Assessment of Illness Behavior (SAIB) were jointly analysed. The aim of this study was to evaluate, compare, and link HRQOL and patients’ perception and response to their illness in either CTCL or CBCL with respect to socio-demographic factors. In addition, this project aimed to provide a basic step to raise dermatologists’ awareness of disease-specific psychological aspects and challenges in CL.
This monocentric, cross-sectional, observational study was performed at the Medical University of Vienna, Austria, following ethics approval (ECS: 2150/2013). The study was conducted according to the principles of the Declaration of Helsinki.
Patients, diagnosed with CTCL or CBCL according to the WHO–European Organization for Research and Treatment of Cancer (EORTC) classification (11), were invited to participate, either personally (n = 109) at the outpatient clinic of the Department of Dermatology or by a single postal mailing (n = 60) from 2014 until 2016. To create homogeneity within the CTCL study cohort, an additional subdivision was performed: (i) early-stage MF (stage IA–IIA), (ii) advanced-stage MF/SS (stage IIB-IVB) (12), and (iii) other than MF/SS (non-MF/SS), resulting in 4 groups, including (iv) CBCL. The non-MF/SS study group did not comprise aggressive variants. Participants aged 18 years and above, who were capable of completing questionnaires independently, were included. Socio-demographic information, stage and duration of the disease were recorded.
The validated German versions of the following questionnaires were used in this study: IPQ-R assesses illness perception in terms of one’s personal beliefs about the disease (18). It contains 9 subscales: 1: “identity” (occurrence of general symptoms and their relation to current disease), 2: “consequences” related to illness, 3: “coherence” (understanding of illness), 4: belief in “personal control”, 5: belief in “treatment control”, 6: “timeline acute/chronic” (expected duration of illness), 7: “timeline cyclical” (variability of symptoms), 8: “emotional representations” associated with disease, and 9: suspected disease “cause”. The “identity” scale is answered yes or no; all further items are assessed on a 5-point Likert-type scale, from “strongly disagree” to “strongly agree”.
High scores for “identity”, “consequences”, and “timeline acute/chronic” implicate attribution of general symptoms to the disease, belief in negative consequences, and chronic/cyclical nature of illness. High scores for “coherence” and “personal/treatment control” constitute patients’ positive beliefs in self-control and understanding of disease.
SAIB assesses illness behaviour as individual handling of one’s state of health (19). Items are rated on a 4-point Likert-type scale, from “I agree completely” to “I disagree completely” and are assigned to 5 parameters: 1: “verification of diagnosis” (demand for multiple diagnostic procedures), 2: patient’s individual “expression of symptoms”, 3: patient’s confidence in “medication and treatment”, 4: “consequences of illness”, and 5: “scanning” (scanning of body functions) (20). High scores indicate somatization and hypochondriasis, whereas low scores refer to denial of illness (21, 22).
Skindex-29 is a skin-specific HRQOL instrument for measuring patients’ experiences of illness and disease-related therapies (23–28). It assesses 3 domains describing symptoms, functioning, and emotions on a 5-point Likert-type scale, ranging from “never” to “all the time” (29). Higher scores indicate poorer quality of life (30).
Statistical analysis was conducted with IBM® SPSS® Statistics (version 22.0). Descriptive statistics were performed to analyse the frequency distribution of all variables of interest. Kolmogorov–Smirnov test was used to test for normal distribution. Differences between metric variables were calculated by Student’s t-test or Mann–Whitney U test. Statistical analyses were performed by means of Skindex-29, IPQ-R, and SAIB, and matched to subgroups by unpaired Student’s t-test or analysis of variance (ANOVA) with post hoc calculations for multiple comparisons. Pearson and Spearman correlation coefficients were applied to test for correlations. Internal consistency was evaluated by Cronbach’s α.
Statistical results are presented as mean ± standard deviation (SD) and range (minimum–maximum). p-values are 2-tailed and a p-value < 0.05 was regarded as statistically significant.
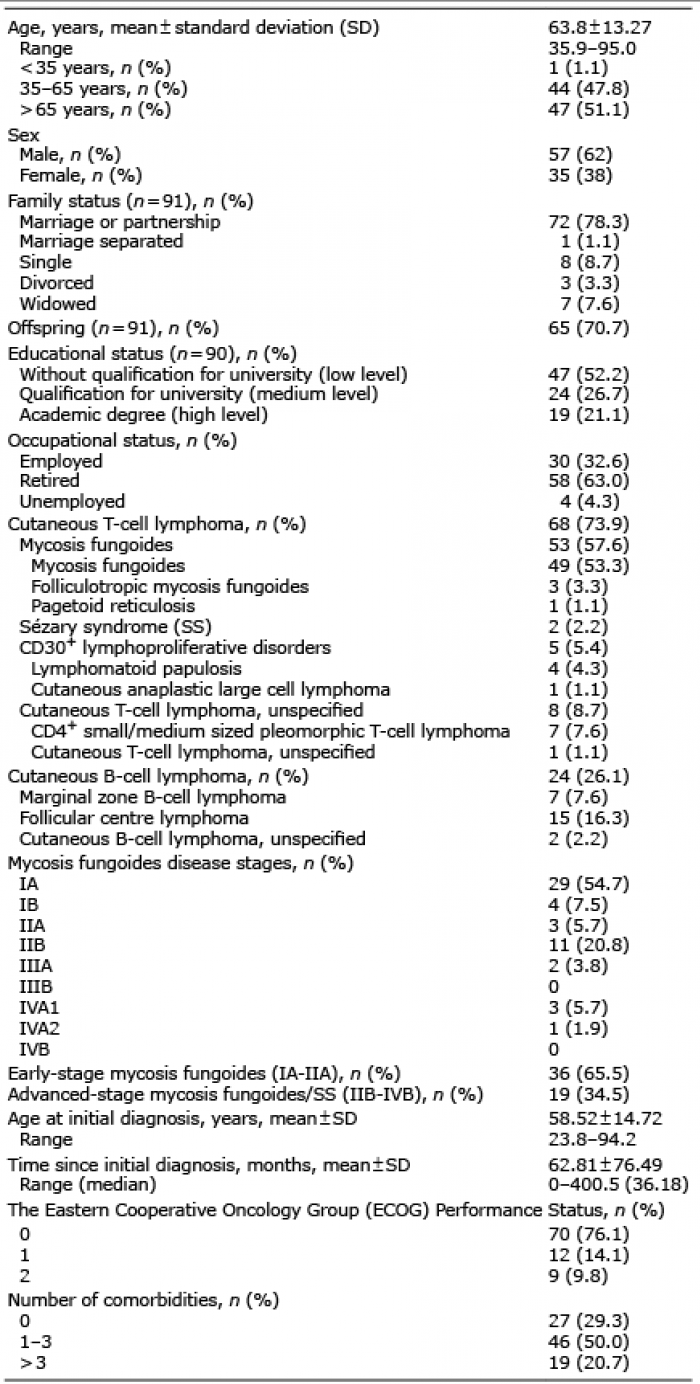
Participation rate in this study was 54% (n = 169). In total, 92 (55 CTCL, 37 CBCL; M:F = 1.6:1; mean age 63.8 years) patients participated in the survey, as summarized in Table I.
Table I. Demographics and disease characteristics of study population (n = 92)
Patients with advanced MF/SS associate more general symptoms with the disease and report fluctuation of their symptoms (highest scores in “identity” and “timeline cyclical”). They believe in a chronic disease course with negative consequences and experience emotional distress (highest scores in “timeline acute/chronic”, “consequences”, and “emotional representations”). They believe that the illness cannot be controlled either personally or therapeutically (lowest scores in “treatment control” and “personal control”) and have a vague understanding of the disease (lowest scores in “coherence”) (Table SI, Fig. 1). In contrast, patients with early-stage MF link less general symptoms to the disease and expect an acute disease course. CBCL and non-MF/SS patients also rate their disease as acute and trust in treatment control.
Fig. 1. Illness perception scores assessed by Revised Illness Perception Questionnaire (IPQ-R). Data were transformed to a linear scale from 0 to 100 to facilitate a visual comparison between the different questionnaires. Values represent mean aggregated scores of early mycosis fungoides (MF), advanced MF and Sézary syndrome (SS), non-MF/SS, and cutaneous B-cell lymphoma (CBCL).
Statistical significance was recorded in “timeline acute/chronic”, showing that patients with advanced MF/SS had significantly higher scores than patients with non-MF/SS (p = 0.008) or CBCL (p < 0.001). In “timeline cyclical” lower scores were recorded for CBCL in contrast to early-stage MF (p = 0.024) and advanced MF/SS (p = 0.005). In “treatment control” higher scores were documented in CBCL compared with advanced MF/SS (p = 0.004).
The suspected “cause” of the disease was attributed to chance/bad luck (33.3%), stress (15.5%), or environment (13.1%) (n = 84).
Highest scores in 4 out of 5 domains (“verification of diagnosis”, “medication and treatment”, “scanning”, and “expression of symptoms”) were recorded for advanced MF/SS (Table SII). This indicates that patients with advanced MF/SS consult several specialists and urge continuous availability of medication/treatment. They regularly scan their body for symptoms and over-communicate these symptoms. “Consequences of illness” showed lowest scores in advanced MF/SS and highest in CBCL, implicating that patients with advanced MF/SS rate their disease as being serious. Patients with non-MF/SS had lowest scores in “verification of diagnosis” and “medication and treatment”. In patients with CBCL, scores for “scanning” and “expression of symptoms” were lowest.
Results for illness behaviour were not statistically significant within the 4 evaluated CL entities.
Highest scores were found in patients with advanced MF/SS and lowest in CBCL (Table II; Fig. 2), which demonstrates that HRQOL is highly impaired in advanced MF/SS and barely influenced in CBCL. Statistically significant difference between early-stage MF and advanced MF/SS was present in Skindex-29 total (sum of the 3 scales) (p = 0.049) and “functioning” (p = 0.019), implicating that patients with advanced MF/SS are more compromised in their daily routines. Stage-dependent correlation in MF/SS was found for Skindex-29 total (r = 0.328, p = 0.014) and for the subcategories “symptoms” (r = 0.321, p = 0.017) and “functioning” (r = 0.350, p = 0.009). Early-stage MF (p = 0.010) and advanced MF/SS (p = 0.042) had significantly higher scores than non-MF/SS in “emotions” implying more emotional distress in the entity MF/SS.
Table II. Health-related quality of life (HRQOL), analysed by Skindex-29, for 92 patients with primary cutaneous lymphoma
Fig. 2. Bar chart of health-related quality of life scores assessed by Skindex-29. According to the originators, data were transformed to a linear scale, varying from 0 to 100 (30). Values represent mean aggregated scores of early mycosis fungoides (MF), advanced MF and Sézary syndrome (SS), non-MF/SS, and cutaneous B-cell lymphoma (CBCL).
Data of illness perception were not evidently associated with illness behaviour, whereas illness perception correlated with HRQOL in CTCL and CBCL (Fig. 3).
Fig. 3. Radar plot. (a) Revised Illness Perception Questionnaire (IPQ-R) scores across 7 dimensions, and (b) health-related quality of life (HRQOL) tool Skindex-29 scores across 3 dimensions. Data were transformed to a linear scale from 0 to 100 to facilitate a visual comparison between the different questionnaires. Values represent mean aggregated scores of early mycosis fungoides (red: early MF), advanced mycosis fungoides and Sézary syndrome (purple: advanced MF/SS), non-mycosis fungoides and Sézary syndrome (orange: non-MF/SS), and cutaneous B-cell lymphoma (dark red: CBCL).
Disease duration. Scores of illness perception “timeline acute/chronic” (p = 0.011), “timeline cyclical” (p=0.022) and “treatment control” (p = 0.010) were significantly higher in patients with prolonged disease duration (> 3 years). Disease duration had no statistically significant impact on HRQOL and illness behaviour.
Age groups. Age groups were analysed according to working life (35–64 years, n = 45) and retirement (> 65 years, n = 48). Patients > 65 years of age had higher HRQOL scores, significantly higher (p = 0.011) in the domain “emotions”. Illness perception and behaviour were not affected by age.
Educational level. Patients were grouped by educational level: low (without qualification for university, n = 47), medium (qualification for university, n = 24), and high (academic degree, n = 19). IPQ-R scores were highest in low educated in “timeline acute/chronic” (p = 0.020) compared with high educated. Elevated scores were observed in high education in “personal control” (p = 0.052) compared with low education. Significant difference was observed in Skindex-29 item “emotions” in low vs. high education (p = 0.043). SAIB results did not significantly differ by education.
Sex differences. Skindex-29, IPQ-R, and SAIB items were not affected by sex.
CLs are a heterogeneous group of lymphoproliferative disorders with enormous variety in clinical appearance and prognosis (11, 13, 31). The feasibility and reproducibility of assessing illness perception with the IPQ-R has been shown only in a mixed panel of patients with CTCL (17). Our study documents that patients’ illness perception diverges depending on the respective CL entity. The IPQ-R results showed that CBCL and non-MF/SS patients rely on personal and therapeutic control, whereas patients with advanced MF/SS experience a chronic and variable disease course with expectation of negative consequences. Also, poor beliefs in personal/treatment control, vague understanding of the disease, and high emotional distress are associated with advanced MF/SS. In contrast, patients with early-stage MF have positive beliefs in personal/treatment control and disease understanding. These subjective beliefs about chronicity, treatment control (common treatment failure in CTCL), and consequences of the disease (32) are true and thus objectified by the IPQ-R. These realistic perceptions might result from the fact that this cohort was informed by experts in the field of CL. Nevertheless, one cannot assume that all patients with CL will rate their disease realistically. Knowledge of patients’ illness perceptions allows documentation of how medical staff and patients differ in their views of the same condition. This information is critical in order to address issues of misunderstanding and miscommunication in healthcare (33). Notably, illness perception in our study is not evidently associated with illness behaviour, and assignment of a specific pattern of illness behaviour to a distinct CL entity is not possible. The assessment of illness behaviour by the SAIB revealed that patients with advanced MF/SS experience a high need to communicate about the disease, demand constant availability of medication, and frequently consult specialists, which is reasonable in cancer. The fact that “illness behaviour” itself is governed by social norms, cultural models, and even the healthcare system (34) might explain that illness behaviour is more dependent on the individual than on the disease.
However, patients with CTCL have long periods with highly visible, itchy, and painful lesions and/or tumours, causing embarrassment and isolation (12). Previous studies have reported impaired HRQOL due to stigmatizing dermatoses, including CTCL (15, 35–38). In this study, HRQOL in MF/SS was more affected than reported previously (14, 16, 39), which might be explained by different socioeconomic factors and lifestyle changes (40, 41). Easy access to web-based information increases awareness of the disease, which might be reflected by worries about disease seriousness and progression in 80% of our patients. Approximately 50% reported disease-induced sleeping disorders, difficulties at work or leisure, and in social life. Our data basically correlate with published literature (15, 16). Interestingly, we found no sex-specific differences, which might be caused by the male predominance within this cohort (42). However, in CBCL and non-MF/SS, HRQOL is barely influenced, which can be explained by the indolent disease course (11). It should be mentioned that a non-MF/SS cohort comprising clinical aggressive variants of CTCL might show a deviating result. HRQOL was closely linked to illness perception and socio-demographics, which is in line with the literature (5, 43, 44). Our data reflect that advanced age and low educational level negatively affect HRQOL. Accordingly, younger age and high educational level correlate positively with personal control and disease understanding, while prolonged disease duration negatively influences illness perception (“timeline acute/chronic”, “timeline cyclical”, “treatment control”).
In conclusion, this study strongly suggests that in CL patients with advanced MF/SS, age > 65 years, prolonged disease duration (> 3 years), and low educational level are related to impaired personal disease management (visualized either by Skindex-29 or IPQ-R).
Patients’ illness perceptions have also been proven to be predictive for coping in cancer. In concrete terms, how cancer patients perceive their illness promotes personal coping strategies either adaptive or maladaptive (acceptance or denial of the illness). Perceptions of treatment/personal control are not related to specific ways of coping (45), but beliefs in personal control (over the disease) are associated with better adherence to therapeutic regimens in patients with hypertension (46). Therefore, the recognition of illness perception might help to identify patients with maladaptive coping (44) and might enable improved adherence to treatment by supporting patients’ self-control (17), e.g. in terms of psychological interventions. Professional patient-education is validated to improve symptom control and health outcomes by training patients’ coping strategies (47).
The information provided by physicians to patients should reflect the actual severity and prognosis of the disease, but should not be demoralizing, because supporting patients’ self-control is known to have a positive impact on the disease course. This dual role of managing and supporting patients once more shows the necessity of interdisciplinary team-work, e.g. cooperation with clinical psychologists to strengthen patients’ positive perceptions of illness. Professional psychological support, e.g. in terms of psycho-education, helps patients to train emotional and cognitive coping strategies to improve symptom control and health outcomes (47, 48). From this perspective, it could be beneficial to train dermatologists in psycho-education.
Moreover, patients’ illness perceptions change rapidly in response to diagnostic results (33) thus providing the possibility of using illness perception as a tool to monitor therapeutic success. For this purpose, the assessment of HRQOL is mandatory in clinical trials (49). Our study emphasizes that, in CL patients, illness perception is closely linked to HRQOL and, above all, IPQ-R results provide applicable information on patients’ individual perception of the disease and the risk of coping poorly. In contrast, the Skindex-29 captures individual disease-related quality of life, which only shows whether HRQOL is impaired. We conclude that the IPQ-R is a useful instrument to identify and monitor patients’ personal beliefs about their disease and personal disease management. Moreover, this cost-effective tool is easy to access and to apply.
Nevertheless, additional studies on the clinical impact of patients’ illness perception facilitating individual disease management in CL are needed. In particular, repetitive evaluation of IPQ-R after patient-education is necessary to investigate whether strengthened perceptions towards one’s illness are crucial in the management of patients with CL. The assessment of patients’ illness perceptions in CL might improve patient care and health outcomes in the face of poor prognosis and the fact that therapeutic options in advanced MF/SS are still limited.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize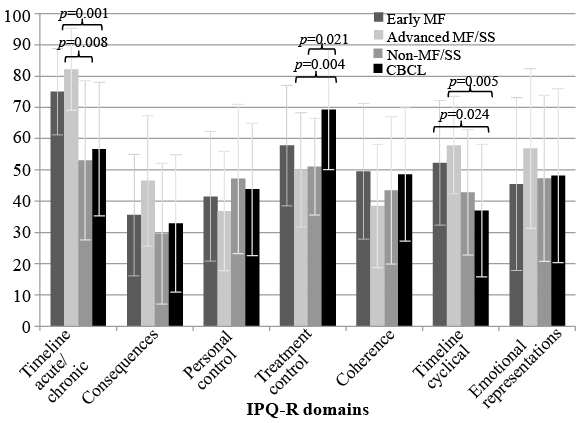 Click to show fullsize
Click to show fullsize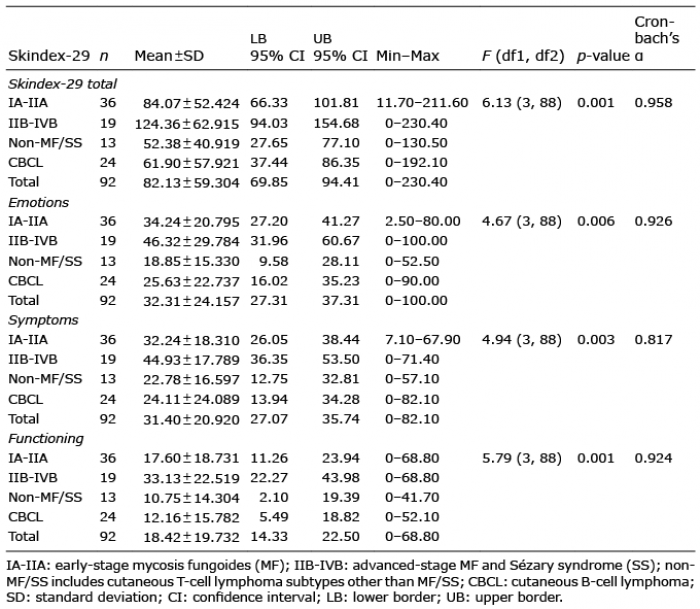 Click to show fullsize
Click to show fullsize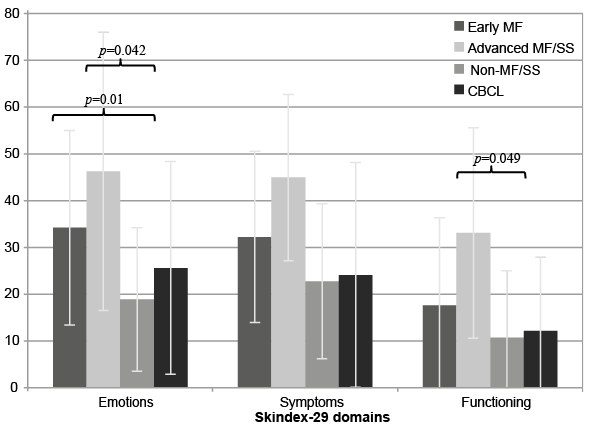 Click to show fullsize
Click to show fullsize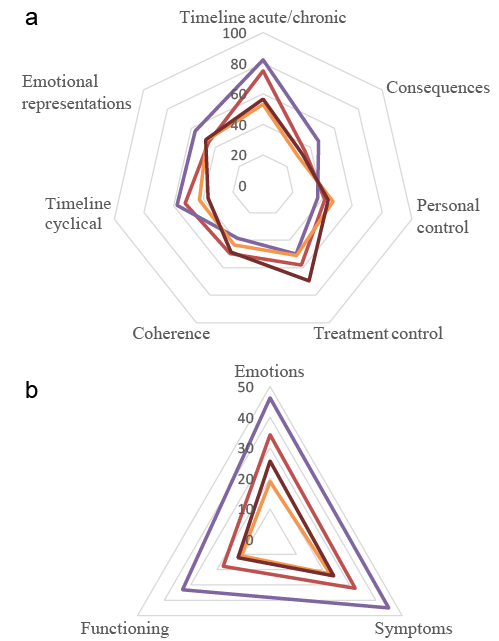 Click to show fullsize
Click to show fullsize