


1Dermatology Unit, Department of Experimental, Diagnostic and Specialty Medicine, University of Bologna, Via Massarenti 1, IT-40138, Bologna, 2Dermatology Section, and 3Anatomic Pathology Unit, Department of Surgery and Translational Medicine, Division Dermatology, University of Florence, Florence, Italy. E-mail: alessandropileri@hotmail.it
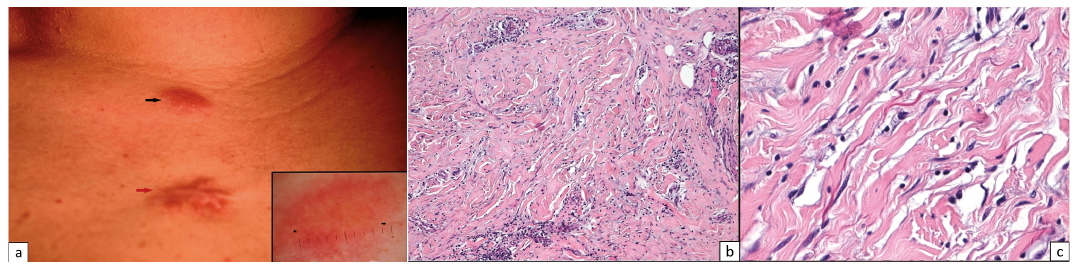
A 38-year-old woman presented with a 2-month history of an asymptomatic erythematous plaque on the jugular notch area (Fig. 1). Dermoscopy revealed erythema at the border of the lesion, while milky-red areas and linear-irregular vessels were seen in the inner part of the lesion. No radial streaming, pseudopods, peppering, or atypical pigmented structures were found. The lesion was surgically removed and histology showed the presence of spindle cells, some with atypical characteristics, randomly aligned and dispersed within an abundant fibrous tissue (Fig. 1b, c). Furthermore, an inflammatory infiltrate within the spindle-cell proliferation was observed. The patient had had a stage IIB bulky Hodgkin’s lymphoma (HL), and had been in complete remission for 5 years after 6 courses of multi-agent chemotherapy, followed by radiotherapy of the mediastinal area. Six months previously, below the suspicious plaque, the patient had had a hypertrophic scar on the site of the peripherally inserted central catheter (Fig. 1, red arrow).
What is your diagnosis? See next page for answer.
Fig. 1. (a) Erythematous plaque on the jugular notch (black arrow) above a previously treated hypertrophic scar (red arrow). Inset: Dermoscopic characteristics of the lesion (from the border to the inner part): erythematous border, milky-red areas with linear-irregular vessels. (b) The presence of spindle cells, randomly aligned and dispersed within an abundant fibrous tissue, with a co-existing inflammatory infiltrate within the spindle-elements (haematoxylin and eosin (H&E) ×10). (c) Some cells showed atypical characteristics (H&E ×40).
Acta Derm Venereol 2018; 98: XX–XX.
Diagnosis: Desmoplastic melanoma
On histopathology neither neurotropism nor nerve invasion were detected. On immunohistochemistry, the spindle-shaped cells were MART-1 and Melan-A negative, while expressed S-100 molecule (Fig. 2a). The desmoplastic melanoma (DM) diagnosis (Breslow thickness 0.6 mm, 0 mitosis, no ulceration) was further supported by the strong positivity of SOX-10 marker (Fig. 2b). Re-excision of 1-cm margins did not show any residual neoplastic cells. No disease recurrence was observed after one year of follow-up.
DM is a rare melanoma variant with non-specific clinical characteristics, thus it is difficult to reach the correct diagnosis (1–5). Based on the presence/absence of a desmoplastic component, Busam et al. (6) have suggested 2 categories: the pure and the mixed (pDM and mDM, respectively). At immunohistochemistry, the disease usually shows positivity for S-100 molecule, while Melan-A and HMB-45 staining is negative. Local recurrence is more common (from 11% to 40% of reported cases) than lymph node involvement (0–18%) (1). At dermoscopy, DM can show the presence of dermoscopic criteria for melanocytic tumours (i.e. atypical pigmented network, radial streaming, pseudopods, dots or globules) in cases associated with non-DM subtype. How-ever, none of the above-mentioned characteristics were observed in our patient. In accordance with Debarbieux et al. (4), the analysis of the vascular pattern, consisting of the presence of linear-irregular vessels and milky-red areas, was helpful to suspect a melanoma. Differential diagnosis should encompass HL dissemination to the skin, spontaneous keloid scar on a chronic radiodermatitis area, and myoepithelial tumour. HL skin-involvement is considered a worse prognostic factor, while clinical presentation varies from disseminated papules to nodules or plaques (7). However, histology ruled out such a disease. Keloid scar diagnosis was more difficult to exclude, due to the presence at dermoscopy of linear irregular vessels, which can be observed in such a lesion (8) and the prior diagnosis of a hypertrophic scar in the same area. Nonetheless, the most common vascular pattern in keloid is the presence of arborizing vessels (8) while milky-red areas are usually absent. The presence of scarce fusiform S-100 positive cells within abundant fibrous tissue could be in favour of a keloid scar, in addition to negativity for MART-1 and Melan-A molecules. Indeed, the S-100 molecule can stain dendritic cells in many types of dermal tumours (9). In such a situation, the strong positivity for SOX-10 (Fig. 2b) was crucial to reach a diagnosis of DM. SOX-10 has recently been suggested to be one of the most sensitive markers for melanocytic tumours and especially for DM (78–100% of series in the literature) (9–12). However, Jacket et al. (13) observed that SOX-10 can also be expressed in scars. Unlike DM, SOX-10 positive elements are scattered within the specimen. In our case the presence of atypical spindle-shaped elements, some of them showing nuclear pleomorphism, as well as the strong SOX-10 expression supported a diagnosis of DM. Moreover, soft tissue myoepithelial/mixed tumours can strongly express SOX-10 molecule. In contrast to DM, these tumours co-express myoepithelial markers, such as keratins AE1/AE3, GFAP and p63 (14). The patient’s age, younger than normal incidence of DM (37 vs. 66 years) is another peculiarity of our case and warrants a comment. It can be speculated that HL itself or the related therapies may have triggered the disease, determining some genetic mutation.
Fig. 2. The malignant cells (arrow) expressed: (a) S-100 and (b) SOX-10 molecules, at the nuclear and cytoplasmic level and nuclear level, respectively (immunoalkaline phosphatase, Gill’s haematoxylin nuclear counterstaining, both ×40).


 Click to show fullsize
Click to show fullsize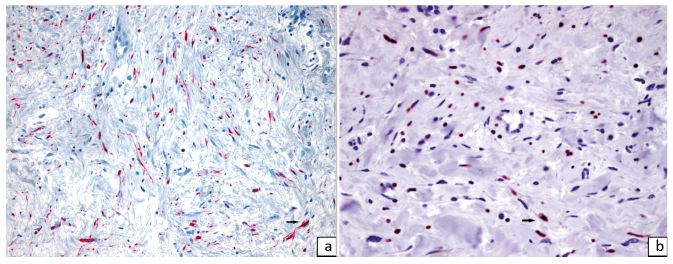 Click to show fullsize
Click to show fullsize