


1Laboratory of Neurosciences of Brest (EA4685), Faculty of Medicine, University of Brest, FR-29200 Brest, Departments of 2Plastic Surgery and 3Dermatology and 4INSERM CIC 1412, University Hospital of Brest, Brest, 5CNRS UMR 7338, Biomechanics and Bioengineering, Technological University of Compiègne, Compiègne, and 6Myelin maintenance and peripheral neuropathies (EA6309), University of Limoges, Limoges, France. *E-mail: laurent.misery@chu-brest.fr
Accepted Oct 19, 2017; Epub ahead of print Oct 23, 2017
Deep burn injuries alter the integrity of skin innervation and have a significant impact on patient’s quality of life by compromising perceptions of touch, temperature and pain. Moreover, patients can develop long-term disabilities, ranging from loss of cutaneous sensibility to chronic pain, itch and other paraesthesia and dysaesthesia (1, 2).
The mechanisms involved in skin reinnervation following burns remain unclear. Depending on the depth of the burn, nerve sprouting can occur from the wound bed or surrounding healthy tissue, but this process fails to provide correct re-innervation of the wound during scarring (1). Although nerve fibres may regenerate after spontaneous wound healing and/or skin grafting, abnormal nerve fibre density is often encountered, resulting in altered skin sensation (3). More precisely, a significant reduction in the axonal regrowth of small fibres within the wound occurs (4).
This pilot study compared the expression of genes involved in the regulation of innervation in healthy skin and in post-burn scars from the same patients. In addition, the intra-epidermal density of nerve endings was measured in these samples.
The study was approved by an ethics committee (CPP Ouest II n°2014-37) and registered on clinicaltrials.gov (NCT02356354). Patients evaluated pain and/or pruritus with the help of a visual analogue scale (VAS) then answered the Douleur Neuropathique-4 (DN4) questionnaire (5) and the Hospital Anxiety and Depression Scale (HADS) (6) to measure the levels of anxiety and depression. The quality of the scar tissue was assessed with the help of the Patient and Observer Scar Assessment Scale (POSAS) (7).
Patients underwent 4-mm diameter skin biopsies in the post-burn scar and in the contralateral healthy skin. Each skin sample was identified by a code number to allow blinded analyses and cut into 2 half-biopsies; one was fixed overnight in a 4% paraformaldehyde bath and then preserved in a phosphate-buffered saline (PBS) – 10% sucrose bath for an additional 24 h prior to being frozen and stored at –80°C. The biopsies were cut into 7-μm or 30-μm-thick sections, spaced at least at 98 μm apart.
Determination of nerve fibre density was performed as described previously (8, 9). The other half-biopsy was preserved at –80°C in RNAlater (Thermo Fisher, Carlsbad, CA). RNA was later extracted with a Purelink RNA Micro kit (Invitrogen, Carlsbad, CA) after lysis with a rotor stator in lysis buffer. RT-PCR was performed using the High-capacity cDNA reverse transcription Kit (AB Applied, Foster City, CA). The expression of genes that can regulate neuronal regeneration was studied with TaqMan technology and the kit TaqMan Fast Universal PCR Master Mix (AB Applied) associated with a couple of specific gene assays. Actin B was used as a housekeeping gene standard. For each half-biopsy, the expression of each gene was first normalized to the expression of actin B, which was stable (ΔCt). The levels of expression were normalized in scars and then compared with those in healthy skin (ΔΔCt) for all patients. The final results were expressed according to the multiplication factor of each gene in scars by comparison with contralateral healthy skin (calculation of “×-fold change” according to 2-ΔΔCt).
Although this is a pilot study, statistical analysis was performed.
Six patients were included in the study (3 men and 3 women, ranging from 22–66 years old). The burn was chemical in one case and thermal in 5 cases. The total body surface area of burns (TBSA) was higher than 40% in one patient, but lower than 15% in the 5 others. The age of the burns ranged from 1 to 4 years. Using POSAS (thickness ≥ 6/10), 3 patients had hypertrophic scars (patients 3, 5 and 6). The mean intensity of pain was 5.2/10 (from 2 to 9) and that of itch was 5/10 (from 4 to 8). All patients could be considered to present with neuropathic pain, with a mean DN4 score of 6.2 (from 4 to 8; score > 4 for the diagnosis). Patients did not show pathological scores on the HADS depression subscale (scoreHADS < 7), but 3 patients had a pathological score of anxiety (score > 7).
The profiles of expression of the studied genes (artemin, BDNF, FGF-2, GDNF, HSP27, IL6, NGF, neurturin, NT-3, NT-4, Netrin 1, semaphorin 3A, persephin and VEGF) were variable in each patient. Overexpression was assessed by a level of expression that was increased 2-fold or more. Nine genes were overexpressed according to this rule: artemin (ARTn), BDNF, IL6, neurturin (NRTN), NT3, NT4, semaphorin 3A (SEMA3A) and persephin (PSPN). Among them, IL6 and SEMA3A were highly overexpressed in the scars of 2 patients. There was no significant difference between patients with hypertrophic and non-hypertrophic scars.
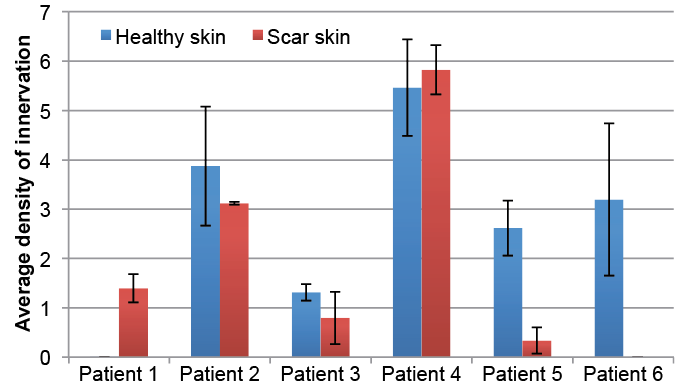
The results were also heterogeneous. Two patients had notably higher densities of intra-epidermal fibres in scars than in healthy skin. By contrast, the densities were decreased in the other patients, especially those who had hypertrophic scars (Fig. 1). No significant differences were found.
Fig. 1. Density of intra-epidermal nerve endings. Post-burn scars (red) by comparison with contralateral healthy skin (blue) in the same area. Patients 3, 5 and 6 had hypertrophic scars.
This pilot study of 6 patients was performed with a rigorous methodology and provided interesting results on the expression of genes that are involved in neuronal growth and the density of intra-epidermal nerve fibres. Due to the low number of patients, no significant differences could be determined, but the heterogeneity of the results was impressive and suggests that a study with a large number of patients should be performed.
All patients reported painful and itchy sensations in their scars, which revealed a quantitative and/or qualitative disorder of skin innervation. The density of intra-epidermal nerve fibres showed a number of variations that were not clearly associated with the presence of a scar, in comparison with the contralateral side. None-theless, we found that the 3 patients with hypertrophic scars presented with a dramatic decrease in the density of innervation, as reported previously (10). A previous study suggested that the PGP9.5 immunoreactive fibre count was lower in burn-graft than control skin and that the substance P immunofluorescent fibre count was significantly increased (11), but no data were available regarding the age of the burns and the characteristics of the scars. A study comparing skin innervation in healthy skin and scars from patients with painful post-burn scars did not find any difference in the density of nerve fibres, but calcitonin-gene related peptide (CGRP) immunostaining was significantly elevated in both uninjured and scar sites of patients with chronic pain compared with the control group (12).
The expression of genes that could be implied in the regulation of skin innervation was also variable. Nonetheless, 9 genes were of interest due to their higher expression in scars than in healthy skin. Another observation is that IL6 and SEMA3A were overexpressed in hypertrophic scars that were also poorly innervated. IL6 is known to be elevated in inflammation and is involved in neuronal growth and hyperexcitability (13). SEMA3A regulates neuronal growth by repelling the growth of dendrites (14).
In conclusion, this pilot study, which is also a feasibility study, shows a wide heterogeneity of results between healthy skin and post-burn scars, but suggests that a further study with a larger patient population is required to better understand the alterations in skin innervation after burns, especially in hypertrophic scars. Only genes IL6 and SEMA3A are discussed in this Short Communication due to space constraints.
This work was supported by the French Armaments Procurement Agency (DGA N°2013 94 0903).


 Click to show fullsize
Click to show fullsize