


University of Groningen, University Medical Center Groningen, Center for Blistering Diseases, Department of Dermatology, Groningen, The Netherlands
Pain is one of the most debilitating symptoms in epidermolysis bullosa (EB) leading to reduced quality of life. Pain in EB comprises both neuropathic and non-neuropathic qualities. An assessment of pain qualities has not formerly been completed in EB. The Pain Quality Assessment Scale (PQAS) is an adjusted version of the validated Neuropathic Pain Scale and includes 20 pain qualities and descriptors. Patients with EB (n = 43) rated the pain qualities in the PQAS on 20 numerical scales and 1 multiple choice question. Pain was experienced by 39 patients (91%). In general, patients with EB experience intense and unpleasant pain on the surface of the skin; the hands and feet are most commonly affected. The subtypes, recessive dystrophic EB and junctional EB reported pain qualities pathognomonic of neuropathic pain. The PQAS adds value to the current practice of global pain intensity scoring in EB.
Key words: epidermolysis bullosa; pain; survey.
Accepted Oct 19, 2017; Epub ahead of print Oct 23, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Marcel F. Jonkman, Department of Dermatology, University Medical Center Groningen, Hanzeplein 1, NL-9700 RB Groningen, The Netherlands. E-mail: m.f.jonkman@derm.azg.nl
Epidermolysis bullosa (EB) is a group of inherited mucocutaneous blistering disorders that lead to painful erosions, strictures and contractures. The incidence of EB is 1:22,000 births and the prevalence is 2.4:100,000 (1); a total of 587 patients are currently registered in the Netherlands (population approximately 17 million). The disease is caused by mutations in structural proteins maintaining the integrity of stratified squamous epithelia. The splitting of skin and mucous membranes and subsequent blistering lead to a cascade of secondary effects that require comprehensive multidisciplinary clinical care, in which pain has been identified as one of the most significant and unbearable aspects (2).
The most important issues in EB include the symptoms experienced by patients on a daily basis. One of the greatest challenges reported by patients is controlling pain during dressing changes (3). Therefore, new research on effective pain alleviation, improving best-practice guidelines, will have an immediate and far-reaching effect on clinical practice.
EB research encompassing pain has been limited by a tendency to highlight global pain intensity rather than measure individual qualities of pain (4). This is in contrast to current consensus that pain qualities or descriptors can aid the clinical classification of the nature of pain (e.g. neuropathic) and give direction to appropriate treatments (5). Not identifying the qualities of pain limits the ability to tailor treatment regimens for individual patients, as pharmacological treatments of neuropathic and non-neuropathic pain differ, and exposes patients to unnecessary health risks and healthcare costs for analgesic medicines (6).
Pain in EB is highly associated with wound presentation, is extremely debilitating, and correlates strongly with a reduction in patients’ quality of life (QoL) (3).
The general consensus is that pain in EB is caused by neuropathic and non-neuropathic mechanisms, probably exacerbated by central nervous system sensitization and psychological conditioning. Pain associated with extensive wounds has neuropathic qualities as it has a “burning” sensation. A recent study confirmed a source of neuropathic pain as they showed a decreased intraepidermal nerve fibre density in patients with recessive dystrophic EB (RDEB), caused by injury (probably due to trauma, metabolic-toxins, infections and nutritional deficits, amongst others) to the distal terminals of small fibres (7).
The most updated set of evidence-based best-practice EB guidelines addresses the many painful scenarios or events, including pain from surgery, chronic wounds, dressing changes, baths, ulcerative lesions, gastrointestinal tract, bones, corneal abrasions and end-of-life scenarios (3). In the daily life of patients with EB, analgesia is key to coping with painful symptoms of multisystem disease. The use of allopathic drugs for every cause of pain may lead to a level of sedation that will hinder normal productivity and the ability to perform other daily activities. This poses a problem, as there is not one form of adequate pain therapy for these patients (3).
The complex pathophysiology of EB means that the causes of pain cannot always be identified and treated appropriately. The aim of this study is to harness the clinical descriptors of pain qualities in EB by applying the Pain Quality Assessment Scale (PQAS), which will enable more accurate assessment of treatment and intervention outcomes through patient-reported pain qualities.
This study is a cross-sectional survey for patients diagnosed with any subtype of EB, registered at the Center for Blistering Diseases at the Department of Dermatology, University Medical Center Groningen (UMCG).
The translated Dutch PQAS questionnaire describes the levels and qualities of pain experienced by participants in the last week (8). The PQAS is an adapted version of the clinically validated Neuropathic Pain Scale (NPS) (9), containing 10 additional pain descriptors. We selected the PQAS for this study because of its broad inclusion of neuropathic and non-neuropathic pain qualities. All participants completed the PQAS once and were asked to rate the severity of each of the 20 pain qualities using a numerical rating scale (0 = no pain/sensation; 10 = the most pain/sensation imaginable) and 1 multiple-choice question on the temporal quality of pain (Table I).
Table I. Definitions of time qualities of pain as described to patients completing the Pain Quality Assessment Scale (PQAS) survey
Means and standard deviations were calculated for all pain qualities. The diagnosis EB was divided into 4 genetic subtypes, EB simplex (EBS), junctional EB (JEB), RDEB, and dominant dystrophic EB (DDEB). Statistical differences were calculated using independent samples t-testing, with a significance of p < 0.05 on IBM’s SPSS software.
Ethical approval to complete this study was obtained from the ethics board of the UMCG.
The PQAS was sent to 134 patients and was completed by 43 patients (response rate 32%). Thirty-nine patients (91%) experienced pain by scoring higher than zero for at least 1 parameter of pain (RDEB = 5; DDEB = 9; EBS = 19; JEB = 6).
The general trend in the entire study portrayed patients with EB as experiencing intense and unpleasant pain located on the surface of the skin (Fig. 1). The feet and hands were the most commonly affected anatomical locations, followed by arms and legs, as shown in Fig. 2. The global measurement of pain (intense) showed that JEB and RDEB scored the highest, with means of 5.5 and 5.4, out of 10, respectively, significantly higher than patients with EBS who scored a mean of 2.4. The unpleasant experience of pain (described by the words annoying, bothersome, miserable and intolerable was given the highest score of the 20 qualities, in 3 of the 4 subtypes (RDEB = 6.4; EBS = 3.5; JEB = 5.7). Patients with DDEB attributed the highest score to pain with an itchy sensation (5.7). High mean scores for a sharp pain were reported in patients with RDEB (5.8) and JEB (5.3), whereas patients with EBS attributed higher mean scores to sensitive (2.7) and tender (2.8) pain qualities.
Fig. 1. Radar diagram portraying mean scores (0–10) of pain qualities from the Pain Quality Assessment Scale (PQAS) for each subtype of epidermolysis bullosa (EB). JEB: junctional EB; EBS: EB simplex; DDEB: dominant dystrophic EB; RDEB: recessive dystrophic EB.
Fig. 2. Frequency of anatomical locations of pain in epidermolysis bullosa (EB) (n = 35). Multiple locations may be recorded on one patient.
The results show a trend that patients with JEB, DDEB and RDEB scored higher means than those with EBS on 18 of 20 parameters (Table II). As well as experiencing significantly more intense pain, patients with RDEB and DDEB reported significantly higher means for itchy pain compared with those with EBS. Patients with RDEB also scored significantly higher means for sharp, shooting, unpleasant and surface pain compared with those with EBS.
Table II. Pain Quality Assessment Scale scores of patients with epidermolysis bullosa (EB), and stratified by EB subtype
A cold-type pain sensation was experienced least by all respondents and was reported as the lowest score in patients with RDEB (2.0), DDEB (0.1) and EBS (0.5). Patients with JEB scored similarly low (1.8), however, they reported a cramping type pain with the lowest score (1.2).
The time qualities for pain were selected from 3 items by multiple choice (Table I). The most common time quality for pain was intermittent pain (n = 20; 74%).Variable pain was reported in each (sub)type (n = 5; 19%). Stable pain was reported only in EBS and RDEB (n = 2; 7%) (Fig. 3).
Fig. 3. Time quality of pain per epidermolysis bullosa (EB) subtype of respondents, shown as percentages. EBS: EB simplex; JEB: junctional EB; DDEB: dominant dystrophic EB; RDEB: recessive dystrophic EB.
The PQAS was developed to identify and score qualities of pain that cover both neuropathic and non-neuropathic types of pain. This is the first study to determine qualities of pain in EB.
Overall, the general description in EB was of intense pain, which was experienced as unpleasant. Patients with RDEB reported pain with tender and sharp qualities; DDEB is characterized by pain with deep and itchy qualities; EBS with sensitive and aching qualities; and JEB with surface and sharp qualities.
Recently RDEB was described to include neuropathic pain qualities, further quantified by intraepidermal nerve fibre density (IENFD) testing (7). In our study, RDEB and JEB reported similar mean scores for pathognomonic terms, indicating neuropathic pain (hot, shooting, tingling, electrical and cold). This indicates a comparable neuropathic pain mechanism in JEB, which should be quantified in order to optimize treatment of JEB pain.
With regard to pain in EB largely originating from wounds, the surface is a fitting description of pain qualities. The high intensity of pain was also seen when EB was compared with several other severe dermatological conditions using the Dermatology Life Quality Index (DLQI) survey. The unpleasant pain sensation was also described using the words annoying, bothersome, miserable and intolerable and is an attitude or response to pain. Pain in EB is not well understood, as the qualities of pain have never been described thoroughly. This may be the reason for the current lack of effective treatment guidelines. This is also the reason to support the reported high score attributed to unpleasant pain sensations in our study.
Patients with EBS reported the least severe pain profile, as can be seen clearly for virtually all pain qualities in the radar diagram (Fig. 1). The significant differences between EBS and DDEB, and EBS and RDEB highlight expected differences in pain between subtypes, as was reported in another Dutch study that referred to bodily pain as a parameter of the Health-Related Quality of Life (HRQoL) assessment; patients with EBS reported the least-severe score, followed closely by patients with DDEB (4).
Interestingly, in our study patients with DDEB attributed their highest score to an itchy pain sensation. Patients with RDEB and JEB attributed their highest scores to a sharp sensation, resembling that of a knife, spike or piercing. As well as presenting clinically with a higher prevalence of open wounds than EBS and DDEB, the results suggest that JEB and RDEB pain qualities are similar.
One fascinating result seen across all EB subtypes was that a cold-type pain scored the lowest. A recent study described cold hypersensitivity as a result of deleting the nerve circuit that codes for heat. Similar to the concept that removing heat from a room induces a cold sensation, an ablation or removal of the associated receptors (TRPV 1) can lead to heightened cold sensations (10). In our results the cold-type pain not seen as significant in EB, can either suggest an overcompensating heat sensory circuit, or a limited or disrupted cold sensory circuit.
As the subtypes of EB are more clearly defined (7), it is important to maintain consistent assessments of symptoms in EB through the subdivision and independent analysis of symptoms in each EB subtype. The most updated recommendations on pain management in EB successfully recognized the most effective treatment options for different painful events or circumstances; however, the recommendations were not able to acknowledge the potential for different pain qualities to predominate each EB subtype, as was seen in our study (3).
An additional question as a part of the pain survey (not conventionally included in the PQAS) allowed us to visualize the prevalence of pain per anatomical region in EB. Our findings suggest that most pain in EB is experienced in the feet, followed by the hands. An assessment of the locations of pain in EB had not previously been completed in this manner. This question was accompanied by two 2-dimensional diagrams of the human body (front and rear); however, pain symptoms in EB originating from visceral organs, bones and mucous membranes could not be reported. For future research, an EB-specific pain survey should include pain qualities and accurate anatomical localizations.
The most updated grading system for neuropathic pain research and clinical practice, maintains the importance of incorporating pain qualities into the decision-making pain classification tract (5). These provide clinical reference points for prescription of analgesic medicines, such as gabapentin for neuropathic pain, and allow for patient-specific pain treatments.
In conclusion, the PQAS is an important tool for clinical and research assessment of pain in EB. Determining the qualities of pain, such as those that are pathognomonic for neuropathic pain, will be helpful to measure pharmacological treatment effectiveness through the deep phenotyping of pain, thus avoiding unnecessary exposure to pharmacological treatments.
The authors would like to thank all the persons with EB who volunteered to take part in this study, many of whom shared their personal experiences of pain, one of the most difficult symptoms today. The authors also thank Dr José C. Duipmans, the principal point of contact for patients with EB in the Netherlands, who helped us to make this project logistically possible.


 Click to show fullsize
Click to show fullsize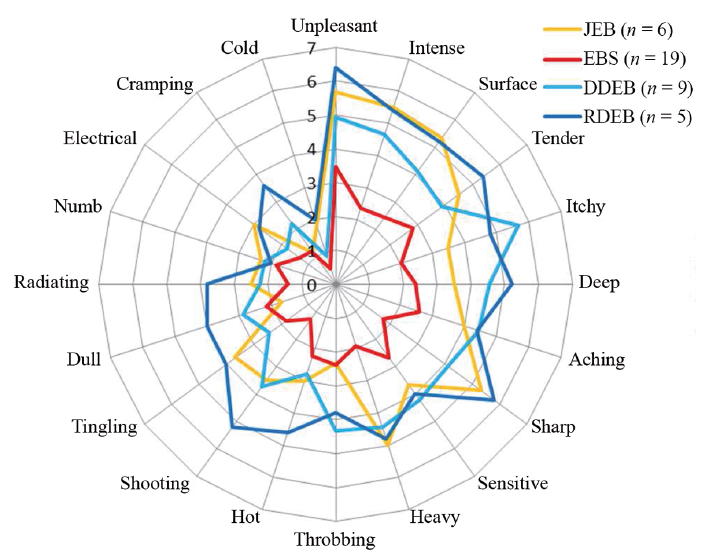 Click to show fullsize
Click to show fullsize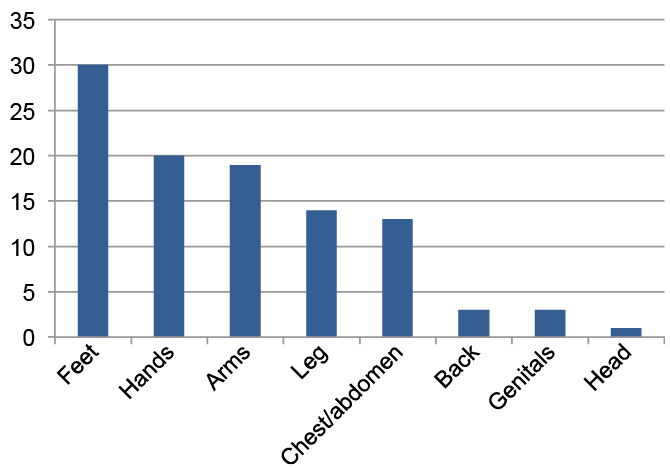 Click to show fullsize
Click to show fullsize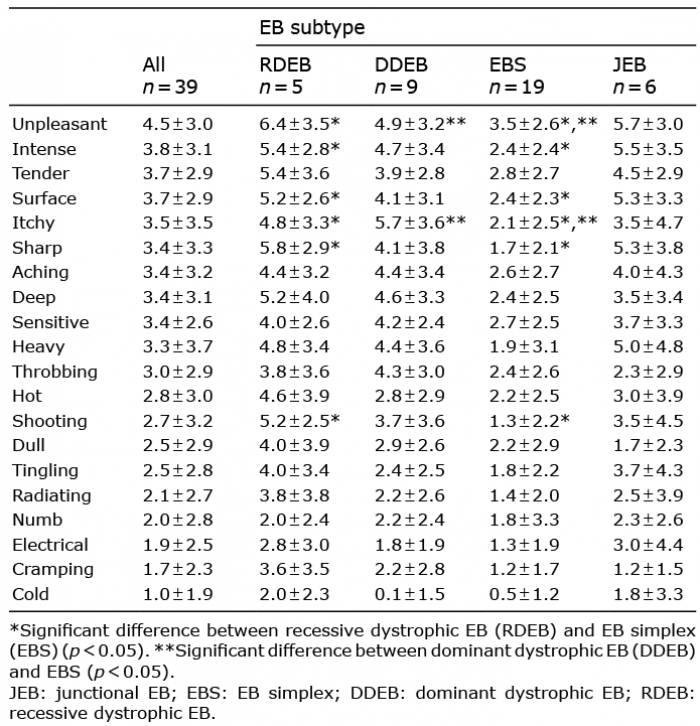 Click to show fullsize
Click to show fullsize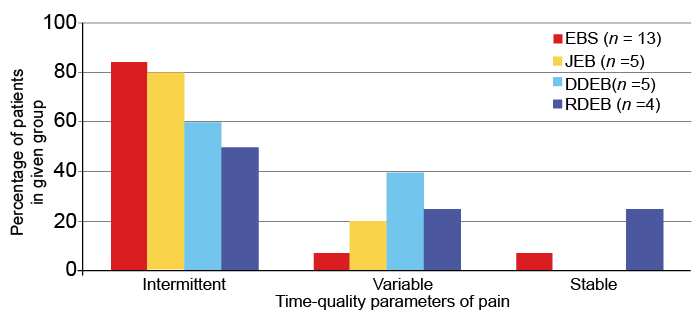 Click to show fullsize
Click to show fullsize