


Unit of Dermatology, Department of Pathophysiology and Transplantation, Ca’ Granda Foundation and Institute for Research and Care, Maggiore Polyclinic Hospital, University of Milan, Milan, Italy. E-mail: m.cusini@policlinico.mi.it
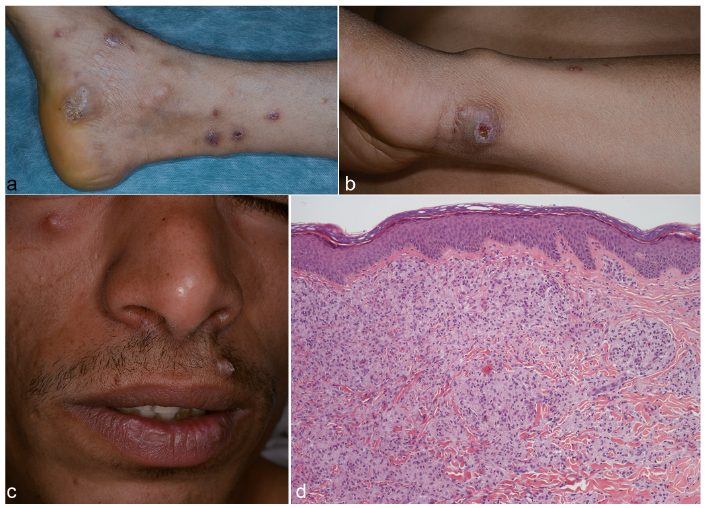
A 29-year-old Egyptian man presented with a 6-month history of multiple papular nodular lesions on his limbs. Prior to admission to our department he had been treated with topical antibiotics and corticosteroids by other specialists, but with no resolution. On admission, he had multiple brownish papular nodular lesions, some with erosions and other with crusts, on his legs (Fig. 1a), and an erythematous ulcerated plaque on his left wrist (Fig. 1b). In addition, some slightly erythematous firm nodules were present on his face (Fig. 1c). The patient’s general condition was non-compromised, he only reported mild itching. He worked as a warehouseman at the vegetable market in Milan and had been in Italy permanently for 2 years. Serology for HIV and syphilis were negative. Neurological examination documented a loss of sensation in the lesions on the lower limbs, with no palpable nerve enlargement. Biopsy specimens from the plaque on the left wrist were submitted for histology (Fig. 1d).
What is your diagnosis? See next page for answer.
Fig. 1. Clinical presentation. (a) Multiple papular nodular crusted brownish lesions on the legs. (b) Ulcerated plaque on the left wrist. (c) Flesh-coloured firm non-tender nodules on the face. (d) Histopathology: section of diseased skin demonstrating thinned out epidermis with a grenz zone and underlying dermis demonstrating vacuolated and foamy interlacing histiocytes (haematoxylin and eosin (H&E) ×20).
Acta Derm Venereol 2018; 98: XX–XX.
Diagnosis: Lepromatous leprosy
On admission to our clinic, we hypothesized a granulomatous disease, particularly a non-tuberculous mycobacterial infection (1). Since histopathological examination of the plaque on the patient’s wrist revealed an atrophic epidermis with an underlying grenz zone separating the dermal pathology from the epidermis and the dermis demonstrated numerous interlacing vacuolated and foamy histiocytes, we performed additional stainings. Fite’s stain helped in substantiating the diagnosis, showing innumerable acid-fast, red-staining bacilli, in bundles, like packs of cigars, and in globi (Fig. 2). With these findings, a diagnosis of lepromatous leprosy was made. The patient was hospitalized in a leprosy reference centre and was started on multibacillary multi-drug therapy. Leprosy is a great mimicker of other diseases, and in this case the patient was treated for a long time by other specialists under suspicion of prurigo nodularis. Hansen’s disease (leprosy) was not considered, probably because it is rare in the western countries. Despite this, it is not unusual to find leprosy still existent, and many times the presentation is characterized by unconventional phenotypes that could further confuse the diagnosing clinician (2, 3). A diagnosis of leprosy should be considered in migrants with skin lesions and neurological symptoms coming from a leprosy endemic country, considering furthermore the long incubation period (4, 5). It would therefore be prudent to perform a complete work-up for Hansen’s disease whenever there is even the remotest suspicion, so that treatment can be started promptly.
Fig. 2. Section of diseased skin stained with Fite’s stain (×40) revealing numerous acid-fast bacilli within the vacuolated histiocytes.


 Click to show fullsize
Click to show fullsize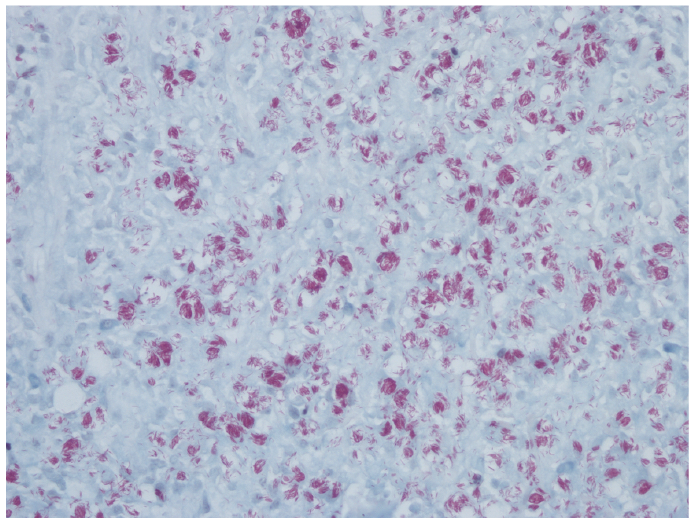 Click to show fullsize
Click to show fullsize