


1Department of Cardiologic, Vascular, and Thoracic Sciences and Public Health, 2Statistics Department, 3”Marco Fanno” Department of Economics and Management, 4Department of Oncology and 5Department of Pharmacy, Veneto Institute of Oncology, and 6Department of Surgery, Oncology and Gastroenterology, University of Padua, Padua, Italy
Cutaneous melanoma is a major concern in terms of healthcare systems and economics. The aim of this study was to estimate the direct costs of melanoma by disease stage, phase of diagnosis, and treatment according to the pre-set clinical guidelines drafted by the AIOM (Italian Medical Oncological Association). Based on the AIOM guidelines for malignant cutaneous melanoma, a highly detailed decision-making model was developed describing the patient’s pathway from diagnosis through the subsequent phases of disease staging, surgical and medical treatment, and follow-up. The model associates each phase potentially involving medical procedures with a likelihood measure and a cost, thus enabling an estimation of the expected costs by disease stage and clinical phase of melanoma diagnosis and treatment according to the clinical guidelines. The mean per-patient cost of the whole melanoma pathway (including one year of follow-up) ranged from €149 for stage 0 disease to €66,950 for stage IV disease. The costs relating to each phase of the disease’s diagnosis and treatment depended on disease stage. It is essential to calculate the direct costs of managing malignant cutaneous melanoma according to clinical guidelines in order to estimate the economic burden of this disease and to enable policy-makers to allocate appropriate resources.
Key words: melanoma; direct cost estimation; clinical guidelines; whole disease model.
Accepted Oct 31, 2017; Epub ahead of print Nov 7, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Alessandra Buja, Laboratory of Health Care Services and Health Promotion Evaluation, Unit of Hygiene and Public Health, Department of Cardiologic, Vascular, and Thoracic Sciences and Public Health, University of Padova, Via Loredan, 18, IT-35131 Padua, Italy. E-mail: alessandra.buja@unipd.it
The economic burden of cancer is increasing, due not only to rising incidence and survival rates, but also to the increasing costs of patient care (1, 2). The incidence rates of cutaneous malignant melanoma among Caucasian populations have risen steadily over recent decades (3). In Italy, the incidence rate is increasing for both men (from 1.6/100,000 in 1970 to 21/100,000 in 2015) and women (from 2/100,000 in 1970 to 17/100,000 in 2015) (4). Recent evidence suggests that this trend is due largely to a higher incidence of thinner melanomas (which have become easier to identify with improvements in early diagnostics) and to changes in lifestyle (e.g. higher recreational exposure to sunlight) (5–7). Thus, malignant cutaneous melanoma represents not only an important public health issue, but also an economic concern, and the financial pressure on healthcare systems is inducing policy-makers to focus more on the appropriate allocation of existing resources. It has been demonstrated, moreover, that melanoma is associated with a significant number of years of potential life lost (YPLL) and with the indirect costs of premature mortality and morbidity, given its high incidence rates among young adults and the large number of melanoma-related deaths (8).
It is of the utmost importance to devise cost-effective clinical pathways for melanoma, allocating the necessary resources appropriately so as to achieve the best possible patient outcomes, while also ensuring healthcare system sustainability. Standardized guidelines have been developed worldwide to provide recommendations, and to describe the processes and time-frames for managing specific medical conditions or interventions. Clinical pathways should not only improve efficiency and have the advantage of reducing inequalities and unwarranted variability in patient management, but also improve the sustainability of care (9). A standard clinical pathway to cover the practical dimension of affordability and feasibility, however, should also include an economic impact assessment, providing a complete and detailed breakdown of the resources required.
The costs associated with cutaneous melanoma have been extensively discussed and reviewed in the literature (10), but few studies have provided details of the costs by disease stage and by melanoma management phase, as established by the National Comprehensive Cancer Network (NCCN), including its diagnosis, treatment and follow-up (11). In addition, rapid changes in the way melanoma is treated (especially in the advanced stages of the disease) make previously published estimates out of date, and differences in how health systems operate (e.g. in the USA and the EU) can undermine the transferability of any economic assessments.
The main purposes of the present study were: to develop a “whole-disease” model (12) of melanoma care encompassing all relevant aspects of the disease’s staging and treatment, from pre-clinical conditions through a first year of follow-up; and to identify the patient outcomes and expected direct costs of melanoma by stage at diagnosis and phase of its management.
Consistent with other international guidelines (13), the Italian Medical Oncological Association (AIOM) developed clinical guidelines for malignant cutaneous melanoma to cover its management from diagnosis to all subsequent staging, treatment and follow-up actions (14). Like some other Italian regions, the Veneto Region adapted these national guidelines to its regional context and defined a diagnostic and therapeutic patient care pathway.
Based on the Italian guidelines for melanoma, we developed a very detailed decision-making model that describes the probabilities of a series of potentially necessary diagnostic or therapeutic actions, the associated costs, and the outcomes expected on a 1-year time horizon. This model enables an estimation of the cost of each stage and phase of the disease as the sum of the costs involved weighted by the probability of the action being needed for each patient, and then calculates the total costs incurred by the public healthcare system (15).
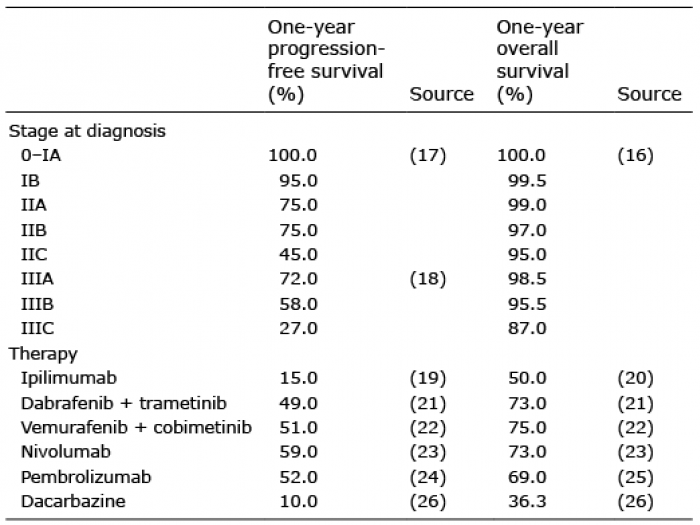
The probability of patients taking each step was divided into 2 categories, defined as clinical and process probabilities. Clinical probabilities were estimated mostly from the literature. Overall and progression-free survival rates by disease stage at diagnosis (for stages 0–III), and by therapy (for inoperable patients with stage IV or III) were drawn from the literature (Table I; 16–26).
Table I. One-year progression-free and overall survival rates by stage at diagnosis and treatment (for patients with inoperable stage III or stage IV melanoma)
Process probabilities are related to the likelihood of a process/procedure being undertaken on a patient with a given clinical condition. Most procedures are bound to be included because they are specified in the guidelines (14) for clinical events for which all patients with a given clinical condition follow a pre-set path (e.g. all patients diagnosed with stage IV melanoma undergo a multidisciplinary examination). However, the guidelines leave some decisions regarding particular diagnostic or therapeutic procedures to the physician’s discretion; therefore, in some cases we had to refer to other guidelines, such as those of the NCCN (13). If the other international guidelines consulted were also insufficiently explanatory, several melanoma experts were asked to judge what proportions of patients underwent certain procedures (based on their professional experience) to enable us to establish estimates that would be as accurate as possible. A survey was designed using the Delphi technique (27) to obtain a consensus among the experts consulted by means of a series of call-recall questionnaires that contained both aggregate information and any open suggestions made by the experts. The final version of the questionnaire, consisting of 16 questions divided into 5 sections, was administered to various experts at the main Italian melanoma treatment centres. Those who responded included 4 oncologists specializing in the medical treatment of melanoma, and 13 surgeons and dermatologists. All the participating experts work at departments with teams specializing in the treatment of melanoma. The survey was conducted using a Computer-Assisted Web-based Interviewing (CAWI) method, and the questionnaire was sent by email. The 17 experts completed 2 successive questionnaires and contributed to the achievement of good results in terms of convergence. The process probabilities adopted in the model were estimated from the medians of the proportions indicated by the experts. All the process probabilities estimated with the Delphi survey, by disease stage and phase of diagnosis and treatment, are described in Tables II and III. For each proportion assessed by means of the Delphi survey, Table IV shows the median, interquartile range, and coefficient of variation associated with the 2 successive detection steps.
Table II. Process probability estimates by primary tumour category related to disease staging and by disease stage related to surgical and medical treatment phases (Delphi Survey)
Table III. Medical treatment scheme according to the clinical pathway 2015, and with new therapies approved in 2016 by the Italian Pharmaceutical Agency for inoperable stage III and stage IV patients
Table IV. Median and interquartile range obtained at the final interview with melanoma experts and coefficients of variation (CV) associated with the 2 successive calls for an assessment of the proportions of patients involved in actions envisaged in the clinical pathway using the Delphi procedure
The study was conducted from the perspective of Italy’s National Health Service, considering only the direct costs sustained by the public health authorities. The model was completed using cost data drawn from official reimbursement tariffs in effect in 2016. The cost assessment concerned all the phases considered in the clinical guidelines, starting from the initial diagnostic and staging procedures through all the surgical and medical treatments. We also considered the costs associated with the first year of follow-up, and any relapses occurring during said time, and the costs of supportive care. The unit costs used in the model are given in Table V.
Table V. Unit costs for each single procedure according to the regional tariffs, and for inpatient care according to the reimbursement for each diagnosis-related group
To assess the costs of medical therapy, we estimated a monthly cost for each drug package, which included the cost of the drug, the cost of drug delivery, and the cost of routine laboratory tests (Table VI). The costs of monitoring the courses of therapy were included in the follow-up costs.
Table VI. Monthly costs of medical therapy in Euros (€)
The costs of relapses were calculated separately, depending on whether the relapse was local, in transit, lymph nodal, or involving distant metastases; these costs were referred to the patients’ stage of disease at diagnosis, not at relapse.
Based on indicators of good melanoma management, we assumed that medical therapy would be stopped in the last 3 months of life for patients who were not expected to survive any longer; and the costs of supportive care were applied to these patients (29).
We estimated the mean per-patient costs by disease stage and phase of management (diagnosis and staging, surgical and medical treatments, follow-up, relapse, and supportive care). The mean per-patient costs were obtained from the total costs related to a particular disease stage and management phase divided by the total number of patients in the same stage. Computing the mean costs by disease stage and management phase enabled our results to be applied even in the event of changes in the patients’ distribution by stage.
The model was tested by its developers (AB, GS, MS), and reviewed by another author who was not involved in developing the model (VR). Then it was submitted for external peer review by clinical experts (CRR, VC and AP) and a methodologist (MB). Finally, check model input values were run against the source material.
The study was approved by the ethics committee of the Veneto Institute of Oncology.
Table VII shows the mean per-patient for the whole melanoma pathway (including one year of follow-up) costs by disease stage and patient management phase: considering all stages, this was €5,332 (ranging from €149 to €66,950 depending on the stage). The costs relating to each management phase varied considerably by disease stage, especially for the medical therapy. From stage 0 to IA, the costs started to increase dramatically, due largely to wide-margin excisions of skin melanomas performed in hospital. The costs of stage IB continued to grow slightly due to the following factors: instrumental tests not required for patients with IA or in situ disease; a different follow-up pattern; and the presence of recurrent cases. For stages IIA, IIB and IIC, the mean per-patient cost continued to increase, though not steeply, associated with the need for computed tomography (CT) scanning for staging purposes, and with the recommendation of interferon therapy. Stage IIB is the first stage of disease for which the mean per-patient cost is higher (112%) than the mean per-patient cost calculated for all stages. The costs more than doubled for stage III patients, the main cost items being hospitalizations for lymphadenectomies, interferon therapy (used more often than for stage II), and new therapies for inoperable patients. Patients in stage III with in-transit metastases were considered as a separate category because their management (and the consequent costs) is substantially different: the costs of in-transit metastases requiring hospital procedures, such as limb perfusion or electro-chemotherapy, and new therapies in a higher proportion of cases, are almost twice as high as for stage III patients with nodal involvement alone. Finally, the mean per-patient cost peaks (at €66,950) for patients with distant metastases (stage IV).
Table VII. Mean per-patient cost by disease stage and phase of treatment in Euros (€) and proportion of each diagnostic-treatment phase cost on total stage cost of the whole pathway (including one year of follow-up)
The main outcome of this study is the development of a model that enables estimation of the direct costs and outcomes for patients with precancerous lesions and cutaneous melanoma throughout a clinical course defined by national and international guidelines (from diagnosis and treatment through the first year of follow-up), and thus of the economic burden of melanoma by disease stage at diagnosis and by phase of patient management.
As expected, also in the light of previous studies on this topic (11, 30–32), the costs associated with melanoma increase for higher-stage disease. The distribution of the costs between the different stages, however, has changed considerably over time, with the per-patient costs of stage IV disease increasing more compared with those of early-stage (0–IIC) disease. In fact, the per-patient cost ratios for stage V and stage VI melanoma have increased dramatically since studies performed in 2008 to 2009 (11, 31). A Swedish study based on a data warehouse recording the costs associated with all patients’ contacts with the healthcare system during the years 2005 to 2012 found a cost ratio between stages IV and I of 10.97 in the first year after a melanoma was diagnosed (32), whereas our study identified a cost ratio between the same stages of 31.27. A study conducted in 2008, before new targeted therapies were introduced, found that chemotherapy accounted for only 17% of the total direct costs of melanoma (33), whereas our data indicate that medical therapy now accounts for 39.2% of the total direct costs. In 2012 Styperek et al. (31) found little difference between the costs associated with stage III as opposed to stage IV, while we calculated that the cost of a stage IV patient is more than 3 times as high as that of a patient with stage III (without in-transit metastases), and more than 1.5 times the cost of a stage III patient with in-transit metastases.
Efforts to estimate the direct costs of treating melanoma in its earlier and later stages would be useful for the purpose of assessing the potential economic value of screening to diagnose the disease early on. In fact, our findings should already suffice to encourage healthcare systems to develop strategies to identify melanoma patients in the early stages of the disease. Patients in clinical stage I have little risk of metastasis or death, and, after the initial outlay for outpatient surgery and follow-up, they cost no more than the general population considered at risk and undergoing routine annual check-ups. This should also reinforce the conviction that a screening campaign to identify in situ and stage IA melanomas might be cost-effective (34), although new studies and new estimates of the costs of treatment are needed for a precise cost-effectiveness analysis of screening programmes. Primary prevention (limiting exposure to sunlight and other ultraviolet light sources; actively promoting the routine use of sunscreen (35), or campaigning to increase awareness and understanding of the potentially negative health effects of exposure to UV radiation, especially during childhood, through various channels such as television, radio, and weather forecasting websites, and in schools) is also important in helping to contain the incidence of melanoma and the related deaths, productivity losses, and treatment costs (8). For example, Euro-melanoma is a pan-European campaign for skin cancer prevention that combines screening with an intensive public education initiative in the mass media. Despite the relatively young population, the suspected melanoma detection rate was 3% (36). The efficacy and cost-effectiveness of this approach would be higher if only middle-aged or older adults were included (37).
The allocation of resources should ideally be based on evidence emerging from clinical research, and affordable care organizations offer unique opportunities to test the cost-effectiveness of competing melanoma detection strategies (38). The combined efforts of all healthcare services and dermatologists are needed to pursue 3 aims simultaneously: to improve the individual patient’s experience of care; to improve the population’s health; and to reduce per capita healthcare costs (39). The task of resource allocation is further complicated by rapidly-rising treatment costs, as in the case of melanoma treatments in recent years. Cancer care services and systems should be constantly evolving to drive better value for patients and the community (40). While many evidence-based pathways, guidelines and frameworks have been introduced to drive quality improvements in cancer care, most of them disregard affordability (41), whereas clinical and cost data should be pooled to provide the knowledge base needed to devise value-based decision-making tools. Policy-makers are often rightly concerned about the affordability of health services, and interested in the health and economic impacts of implementing new strategies (such as the adoption of a novel clinical pathway) in a local epidemiological and demographic context. As Mauskopf et al. (42) said, assessing economic impact should include classifying the policy-makers’ information needs, and producing a full and detailed breakdown of resource use and costs, and a list of expected health outcomes.
A strength of the present study is that the whole clinical pathway was modelled up to a high level of detail, which can provide a broad and consistent disease-level framework for use in conducting economic assessments. This sets it apart from conventional piecemeal approaches, giving it the structural capability needed to compare alternative interventions across the clinical pathway from diagnosis to follow-up. Further research activities could be designed, adopting a whole-disease model based on EU-shared clinical pathways, and including costs by country for each procedure or treatment in the model in order to enable an estimation of the local average costs of melanoma patients by disease stage. In fact, it has been demonstrated that there is still some discrepancy between the costs of cancer patient management in different countries, despite a consensus on the related clinical practice guidelines (43).
This study also has several limitations. Firstly, the estimated costs based on the clinical pathway considered here would apply to cases managed according to best practices, but do not necessarily reflect what actually happens in real-world health services, since physicians do not always follow such standardized pathways, and patients are not always compliant. It would therefore be interesting to conduct a further study to measure actual costs and the gap between these and the expected costs. Secondly, the present study does not consider indirect costs, although they are known to be high for this kind of tumour, especially in its advanced stages (9, 44). A further limitation of our model concerns the costs of new therapies, since it does not take into account that some patients may be enrolled in clinical trials for profit, so the costs of their treatments are not covered by the healthcare system. The model also ignores any toxicity-related healthcare costs because the available data on the toxicity of new therapies are still too recent and often controversial. A further limitation of this study is that it only covers the first year of follow-up, and fails to consider a lifespan time horizon (although the long-term efficacy of the new therapies remains to be determined).
Modelling whole guideline-based pathways enables the main sources of spending to be examined and can thus help policy-makers to plan the most appropriate allocation of future resources. Being able to simulate the scenarios of interest also allows for considerations of future costs vis-à-vis present costs (budget impact analyses), such as the impact of introducing innovative therapeutic or diagnostic technologies.
The authors would like to thank all the experts at the Italian National Melanoma Centers who participated in the Delphi Survey: Paolo Ascierto, Lorenzo Borgognoni, Corrado Caracò, Vincenzo De Giorgi, Maurizio Governa, Marco Lorenzini, Mario Mandalà. Nicola Mozzillo, Pietro Quaglino, Carlo Riccardo Rossi, Mario Santinami, Vanna Chiarion Sileni, Antonio Sommariva, Ignazio Stanganelli, Pierosandro Tagliaferri, Alessandro Testori and Antonella Vecchiato.
Conflicts of interest: Funding for this study was provided by Bristol-Myers Squibb Srl. The company had no role in the design of the study, the collection, analysis, or interpretation of the data, the writing of the manuscript, or the decision to submit the paper for publication.


 Click to show fullsize
Click to show fullsize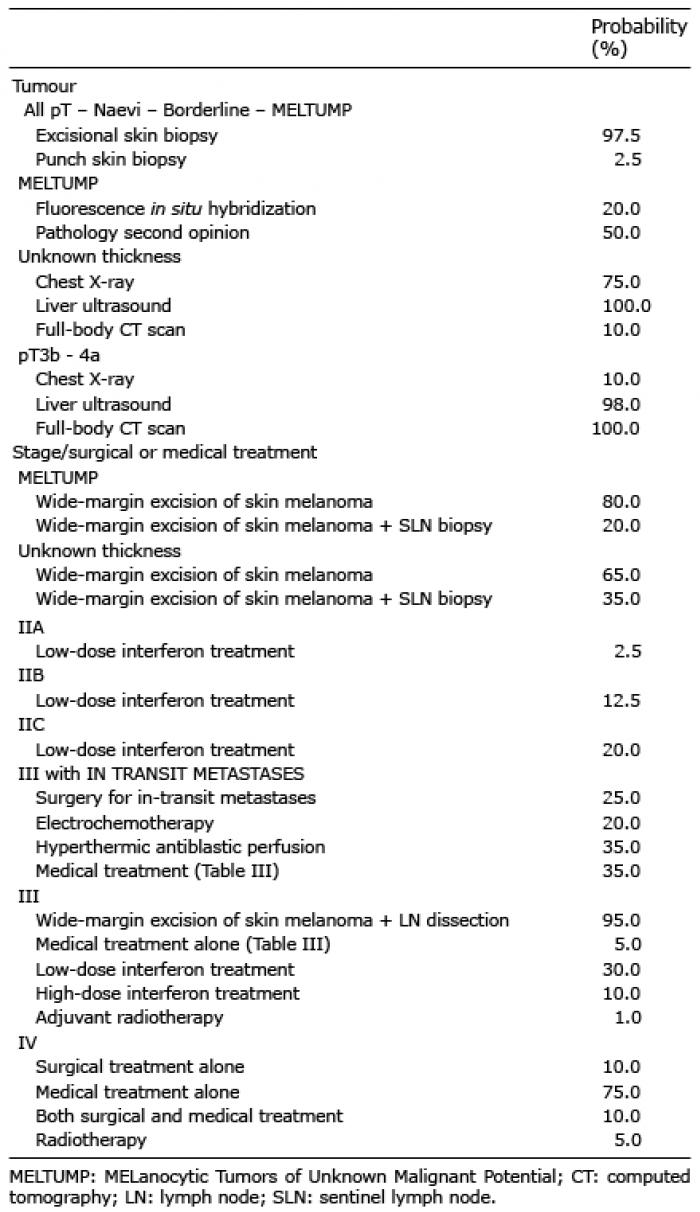 Click to show fullsize
Click to show fullsize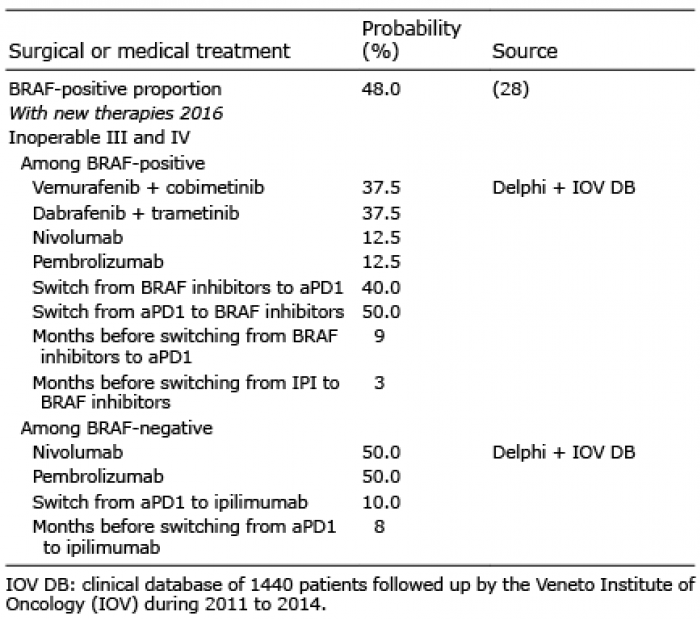 Click to show fullsize
Click to show fullsize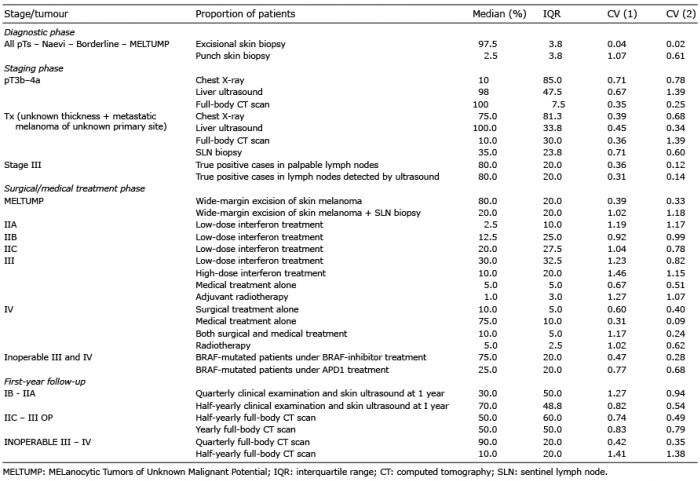 Click to show fullsize
Click to show fullsize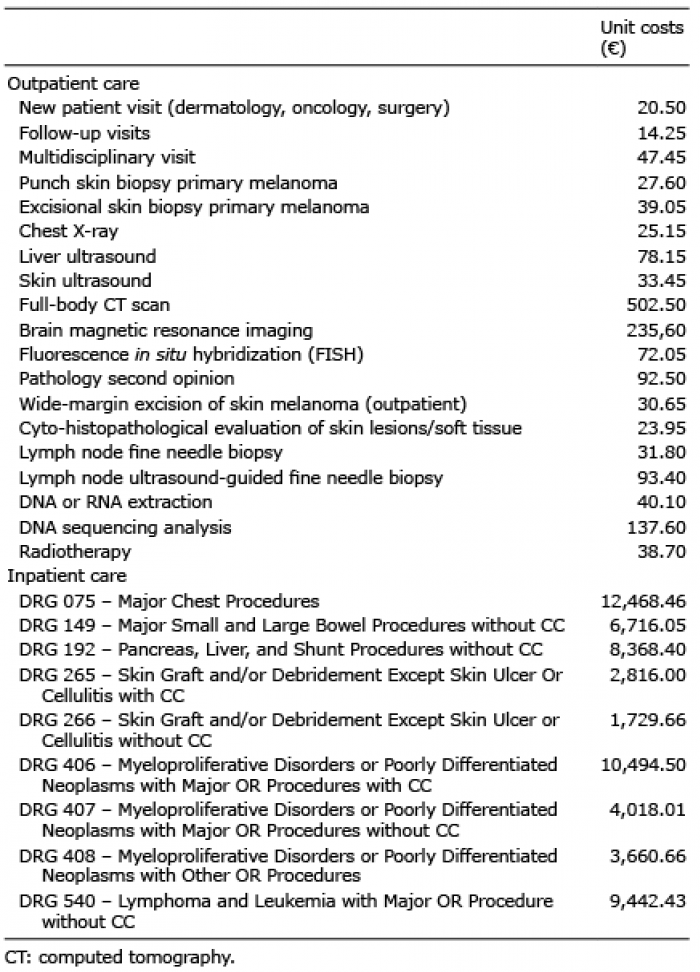 Click to show fullsize
Click to show fullsize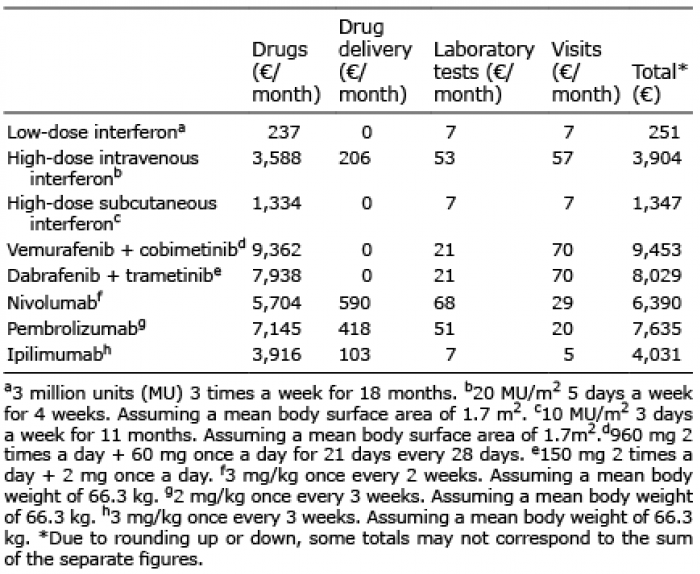 Click to show fullsize
Click to show fullsize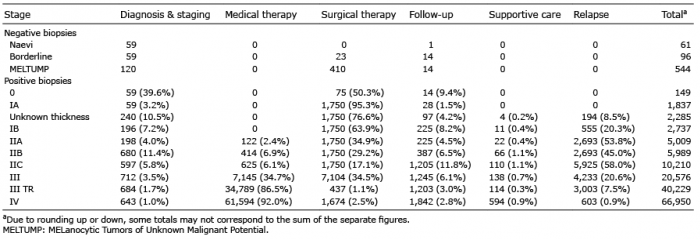 Click to show fullsize
Click to show fullsize