


1Department of Dermatology, Allergology and Venereal Diseases, University of Helsinki and Center of Inflammation, Helsinki University Central Hospital, 2Department of Virology, and 3Department of Bacteriology and Immunology, University of Helsinki, Helsinki, Finland
#These authors contributed equally to this paper.
A retrospective study of 109 skin biopsies with granuloma annulare (GA) or morphea histology from patients with suspected tick bite was performed. Biopsies were tested for cutaneous Borrelia burgdorferi DNA using PCR. The same biopsies were analysed for tick-borne novel agents, Chlamydia-related bacteria (members of the Chlamydiales order), using a PCR-based method. Borrelia DNA was detected in 7/73 (9.6%) biopsies with GA and in 1/36 (2.8 %) biopsies with morphea, while Chlamydiales DNA was found in 53/73 (72.6%) biopsies with GA and 25/34 (73.4%) biopsies with morphea. All Borrelia DNA-positive GA samples were also positive for Chlamydiales DNA. The Chlamydiales sequences detected in GA were heterogeneous and contained Waddliaceae and Rhabdochlamydiaceae bacteria, which are also present in Ixodes ricinus ticks, while the Chlamydiales sequences detected in morphea closely resembled those found in healthy skin. In conclusion, tick-mediated infections can trigger GA in some cases, while correlation of either Borrelia or Chlamydiales with morphea is unlikely.
Key words: granuloma annulare; morphea; Borrelia burgdorferi; chlamydia-related bacteria.
Accepted Oct 31, 2017; Epub ahead of print Nov 7, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Lauri Tolkki, Center of Inflammation, Department of Dermatology, Allergology and Venereal Diseases, Helsinki University Central Hospital, PO Box 160, FIN-00029 Helsinki, Finland. E-mail: Lauri.Tolkki@hus.fi
Granuloma annulare (GA) and morphea (localized scleroderma) are skin reactions with unknown aetiology (1–5). One of the possible causative agents is Borrelia burgdorferi sensu lato, a spirochete transmitted to humans via tick bites. Although the causal connections between B. burgdorferi and GA and morphea have been explored in several studies using various methods, including indirect serological methods and direct detection by PCR, there is no firm evidence of a causative role (6–11).
In addition to B. burgdorferi sensu lato, ticks are known to serve as vectors for a number of other animal and human pathogens, such as Babesia microti, which causes babesiosis, Anaplasma phagocytophilum, which causes human granulocytic anaplasmosis, species of the spotted fever group of Rickettsiae, and Flavivirus, which causes tick-borne encephalitis (TBE) (12–15).
Recently, Ixodes ricinus ticks have also been shown to carry another group of potential human pathogens, Chlamydia-related bacteria (16–19). They share the characteristic features of the order Chlamydiales: strict intracellular lifestyle, biphasic developmental cycle and a large core-set of genes. The traditional members of the order are the established human pathogens Chlamydia trachomatis and Chlamydia pneumoniae (genus Chlamydia, family Chlamydiaceae). During the last 20 years, an increasing number of novel chlamydial species have been described and, currently, 8 additional families are recognized as belonging to the Chlamydiales order. These new families: Parachlamydiaceae, Waddliaceae, Simkaniaceae, Rhabdochlamydiaceae, Criblamydiaceae, Piscichlamydiaceae, Clavichlamydiaceae and Parilichlamydiaceae are collectively called Chlamydia-related bacteria. They were originally detected in various types of environmental samples (e.g. soil and water from various sources), but subsequently also in animals, including arthropods, and humans. Many of them have pathogenic potential (20, 21), and their reservoirs, vectors and transmission routes have been widely investigated, but have mainly remained obscure.
In this study, 109 patient skin biopsies with histologically confirmed GA and localized scleroderma (morphea) were analysed retrospectively. The samples had been studied for the presence of B. burgdorferi, either because of a clinical suspicion of borreliosis or because of abundant plasma cells in the biopsy. In order to determine whether certain types of Chlamydia-related bacteria could play a role in the pathogenesis of these conditions, the occurrence and type(s) of Chlamydiales in the biopsies was examined, and the results compared with our previously published data on healthy skin and ticks (17). We recently reported the occurrence of Chlamydiales in up to 40% of Finnish ticks and, furthermore, in human skin biopsies. Chlamydiales DNA was found in human skin samples, with a prevalence of 49% in healthy skin (19/39, 49%) and 85% in skin samples from subjects positive for B. burgdorferii PCR. This suggests that ticks could indeed serve as vectors for transmission of Chlamydia-related bacteria.
Data for all patients whose skin biopsies had a histology of GA or morphea and were submitted to B. burgdorferi DNA analysis at the Department of Dermatology, Helsinki University Central Hospital from 2010 to 2015 were reviewed. The samples were studied for the presence of B. burgdorferi due to clinical suspicion of borreliosis, history of tick bites, or the dermatopathologist’s recommendation based on histological features. The study included 109 skin biopsies from 73 patients with GA and 36 with morphea. Clinical and serological data were retrieved from patient files retrospectively.
Histopathological analysis was performed as routine investigation in the Laboratory of Dermatopathology, Skin and Allergy Hospital, Helsinki University Central Hospital by an experienced dermatopathologist. Histological slides were available for re-examination by one of the authors (LT) in 71 cases of GA and 34 cases of morphea.
GA has 2 predominant histological variants, palisading and interstitial, both of which are characterized by mucin and dermal inflammation (2). The histopathology of morphea is indistinguishable from the skin lesion of systemic sclerosis (3). The histopathological findings in the samples of our patients with GA and morphea were classic and identical to the description in standard textbooks.
B. burgdorferi sensu lato DNA detection was performed as a part of routine diagnostics by PCR amplification and hybridization with 16S rRNA- and OspA-specific primers and probes, as described earlier (6, 22). Real-time PCR with LightCycler® (Roche, Basel, Switzerland) was also performed. Briefly, PCR reactions contained 10 µl 2×MasterMix of the DyNAmo Flash Probe qPCR Kit (ThermoFisher Scientific, Waltham, MA, USA), 1 µl 10 µM the corresponding forward and reverse primers, 0.5 µl 10 µM probe, and 100 ng template DNA in a total reaction volume of 20 µl. PCR cycling (60 cycles of 95°C 15 s, 60°C 1 min) was performed with a LightCycler instrument (Roche).
Anti-borrelia IgG and IgM antibodies were determined by 2 immunoassays. If the screening test (Genzyme Virotech GmbH, Russelsheim, Germany) was positive, a confirmatory chemiluminescence immunoassay (Liaison®) was performed as a routine procedure (Diasorin, Saluggia, Italy) by HUSLAB (23). The results were interpreted as described earlier (22).
Chlamydiales DNA was detected with a pan-Chlamydiales real-time TaqMan-PCR method, as described earlier (17, 24). Extreme precautions were taken to avoid cross-contamination, and no-template (water) controls were included in each PCR run. The resulting DNA amplicons (approximately 200 bp of the 16S rRNA gene region) were puri?ed by Illustra ExoProStar 1-Step (GE Healthcare, Buckinghamshire, UK) according to the manufacturer’s instructions. Sequencing was then performed at the sequencing unit of the Institute for Molecular Medicine Finland.
BLAST analysis was performed in order to compare the obtained Chlamydiales sequences to the known sequences in the National Center for Biotechnology Information (NCBI) database, especially the Chlamydiales sequences from biopsies of healthy skin and from Finnish Ixodes ricinus ticks. For family-level classification, the first established Chlamydiales strain of the BLAST hit list was determined, and if the sequence identity was ≥ 90%, the 2 sequences were considered as members of the same Chlamydiales family (17, 25, 26).
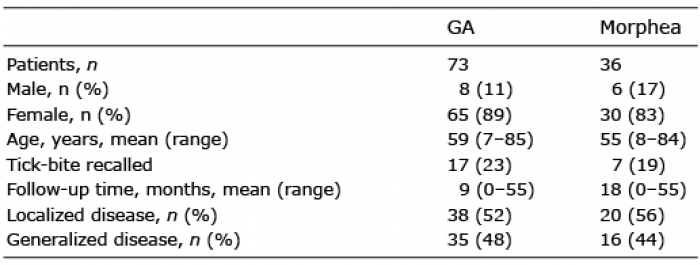
Clinical characteristics of the patients are summarized in Table I. Most patients were female. The mean age of patients with GA was 59 years (range 7–85 years) and that of the patients with morphea was 55 years (range 8–84 years). Most of the patients did not recall having had a tick bite; and this has been reported even for patients with confirmed erythema migrans (22), since the very tiny nymphs fall off the skin unnoticed after feeding. GA was localized in 38/73 (52%) and generalized in 35/73 (48%) of the patients (Table I, Fig. 1). Morphea was localized in 20/36 (56%) and generalized in 16/36 (44%) of the patients (Table I, Fig. 1).
Table I. Characteristics of 109 patients with granuloma annulare (GA) or morphea
Fig. 1. Clinical pictures of granuloma annulare (GA) and morphea skin lesions. (A) Localized GA typically presents with an annular lesion on the dorsum of hand. (B) Generalized GA consisting of papules coalescing into plaques in certain regions. (C) Interstitial GA may present as an erythematous macule (upper arm). (D) Typical presentation of a wide patch of morphea.
Histological findings are summarized in Table II and visualized in Fig. 2. Of the GA cases, 38% were of the interstitial type. Plasma cells were present in 48% of the palisading GA cases and 70% of the interstitial GA cases. Of the morphea cases, plasma cells were present in 31/34 (91%). No correlation between the presence of plasma cells and positivity for either Borrelia or Chlamydiales DNA could be found in either group.
Table II. Summary of histological findings
Fig. 2. Histology of granuloma annulare (GA) and morphea. (A) and (B) Palisading GA: central area of necrobiotic collagen and mucin surrounded by histiocytes, lymphocytes and giant cells. (C) Interstitial GA: histiocytes and lymphocytes are scattered around collagen bundles and blood vessels. Mucin is prominent. In this case plasma cells are present. (D) Histology of fibrotic stage morphea is characterized by tightly packed and eosinophilic collagen bundles, atrophic sweat glands and minimal inflammatory infiltrate. (Haematoxylin-eosin stain; original magnification: A and D ×4; B ×10; C ×20).
B. burgdorferi DNA was detected in 7/73 (9.6%) of the GA cases and 1/36 (2.8%) of the morphea cases. Unlike erythema migrans, lymphocytoma or acrodermatitis chronica atrophicans skin samples (27), 6/7 (85.7%) of the above GA biopsies and the single morphea sample were positive only for ospA. Only one GA sample was positive for both ospA and 16S rRNA targets. Three of the 7 patients with GA had received oral antibiotics before our PCR determination (during the preceding year), which may have influenced the result. Most, 5/7 (71%), of the GA cases positive for Borrelia DNA were of the interstitial type.
Anti-borrelial antibodies were measured in 69 patients with GA and in 35 patients with morphea. The antibodies were defined positive in 8/69 (11%) cases of GA and in 4/35 (11%) cases of morphea. In addition, 7/69 (10%) patients with GA and 4/35 (11%) patients with morphea had borderline antibody titres.
The antibody levels did not correlate directly with the presence of Borrelia-specific DNA in the skin biopsies, since the only PCR-positive morphea patient and 3/7 (43%) of the PCR-positive GA patients had only borderline positive antibody reaction and the rest, 4/7 (57%) of the PCR-positive GA patients had negative serology.
All patients positive for Borrelia DNA received antibiotic treatment with amoxicillin, doxycycline or ceftriaxone with dosage recommended for Borrelia infections (27). Of the GA-cases positive for Borrelia DNA, 5/7 (71.4%) persisted regardless of adequate antibiotic therapy. One patient was cured with parenteral ceftriaxone treatment and one patient was lost to follow-up. The only morphea case positive for Borrelia DNA was cured with a course of amoxicillin and topical corticosteroid. In Borrelia PCR-negative cases, 40/67 (59.7%) of the GA lesions and 22/35 (62.9%) of the morphea lesions persisted until the end of the follow-up. The mean follow-up time was 9 months for GA and 18 months for morphea patients.
Chlamydiales DNA was detected by PCR in 53/73 (72.6%) of biopsies from lesions of GA, and in 25/34 (73.4%) of biopsies from morphea. Altogether 70 sequences were obtained (45 from GA and 25 from morphea). When possible, the sequences were classified by BLAST analysis to family level. In morphea lesions, most of the Chlamydiales sequences belonged to the families of Parachlamydiaceae (56%) and Criblamydiaceae (12%), while 23.5% remained unclassified. Within the GA group, a wider range of Chlamydiales sequences were detected: again, the most prevalent types were Parachlamydiaceae (24.4%) and Criblamydiaceae (15.6%), but in addition to those we detected members of Waddliaceae (11.1%), Rhabdochlamydiaceae (4.4%) and Chlamydiaceae (2.2%). Within the samples from GA, 42.2% of the Chlamydiales sequences could not be classified to the family level (Fig. 3).
All 7 GA skin biopsies positive for Borrelia DNA were also positive for Chlamydiales DNA. However, the single morphea patient positive for Borrelia DNA was negative when tested for Chlamydiales DNA.
Fig. 3. Chlamydiales families in the sequenced pan-Chlamydiales PCR-positive skin biopsies from lesions of granuloma annulare (GA) and morphea, compared with those previously detected in Ixodes ricinus ticks and in biopsies of healthy skin (17).
The diversity of Chlamydiales sequences in skin lesions of morphea closely resembled that found in healthy skin (Fig. 3). However, in the GA lesions, the diversity was wider and also contained members of families Waddliaceae and Rhabdochlamydiaceae, also found in Ixodes ricinus ticks (Fig. 3).
This study is the largest of its kind on PCR and hybridization-based detection of B. burgdorferi in patients with GA. Also, it is the first to inspect Chlamydiales in GA and morphea. According to our results on the prevalence of Borrelia DNA, we propose that infections with B. burgdorferi can trigger GA in some cases, but the direct causal role seems unlikely. The prevalence of Borrelia DNA in our data was 9.6%, which is in accordance with the few previous studies (10). It is noteworthy that Borrelia DNA may persist in the skin for long time (28) and does not necessarily reflect an active Borrelia infection. However, in our retrospective study, the presence of Borrelia DNA was studied because of a clinical or histopathological suspicion of Borrelia infection. Thus, the prevalence in the whole spectrum of GA may be somewhat lower. Since all our GA patients positive for Borrelia DNA were treated with appropriate antibiotics and in at least 71.4% of the cases GA lesions persisted regardless of antibiotic treatment, Borrelia infection does not seem to be directly causative, but rather a triggering factor. This idea is supported by the finding that the antibody levels did not directly correlate with the presence of Borrelia-specific DNA. This is in accordance with the current literature (1). It could also be argued that the only Borrelia DNA positive GA patient whose GA lesions resolved after antibiotic treatment may have actually been a case of GA-like acrodermatitis chronica athrophicans. Four similar cases have been reported recently by French authors (29).
The prevalence of B. burgdorferi in morphea lesions has been studied much more than its correlation with GA. Most studies report a low or missing prevalence of Borrelia (10). Our result with a single case (2.8%) positive for Borrelia DNA is in accordance with previous studies. Because of the low prevalence, a causative or even triggering correlation between Borrelia infection and morphea is unlikely.
Members of the Chlamydiales, Chlamydia-related bacteria are naturally resistant to beta-lactam antibiotics, including amoxicillin and ceftriaxone used in the treatment of Borrelia infections. However, Chlamydia-related bacteria should be sensitive to doxycycline (30). In our study, 8 patients with GA positive for Chlamydiales DNA were treated with doxycycline, but none of them was cured. This speaks against a direct causative role of Chlamydiales in the pathogenesis of GA. Thus, only a triggering effect for GA is possible.
This study has some limitations. The clinical and serological data were retrieved retrospectively from the patient files, and thus the documentation or follow-up of patients was not standardized. The description of possible systemic symptoms was vague or absent in most of the cases, and the majority of patients with localized disease was not followed after initiation of treatment, mostly topical corticosteroid creams or ointments.
In conclusion, Chlamydiales DNA is frequently detected in skin lesion in GA and morphea. In GA, the Chlamydiales diversity differs from that in healthy skin and resembles the diversity observed in Ixodes ricinus ticks, suggesting a tick-derived origin. In morphea, however, the diversity of Chlamydiales sequences was close to that in healthy skin. The occasional presence of Borrelia DNA and the tick-like Chlamydiales diversity in GA lesions combined with poor response to antibiotic treatment favours a possible triggering role of these tick-mediated infections in GA. Their correlation with morphea, however, is unlikely.
This study was supported by Biomedicum Helsinki Foundation, Academy of Finland (1285975) and Helsinki University Central Hospital Research Funds, Helsinki, Finland. The authors would like to thank Leila Jeskanen, MD, for histopathological analyses, and Alli Tallqvist, Kaija Järvinen and Anu Kaitonen for technical assistance.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize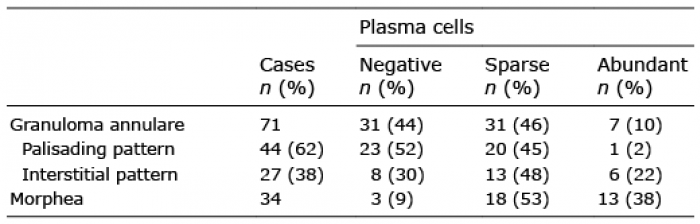 Click to show fullsize
Click to show fullsize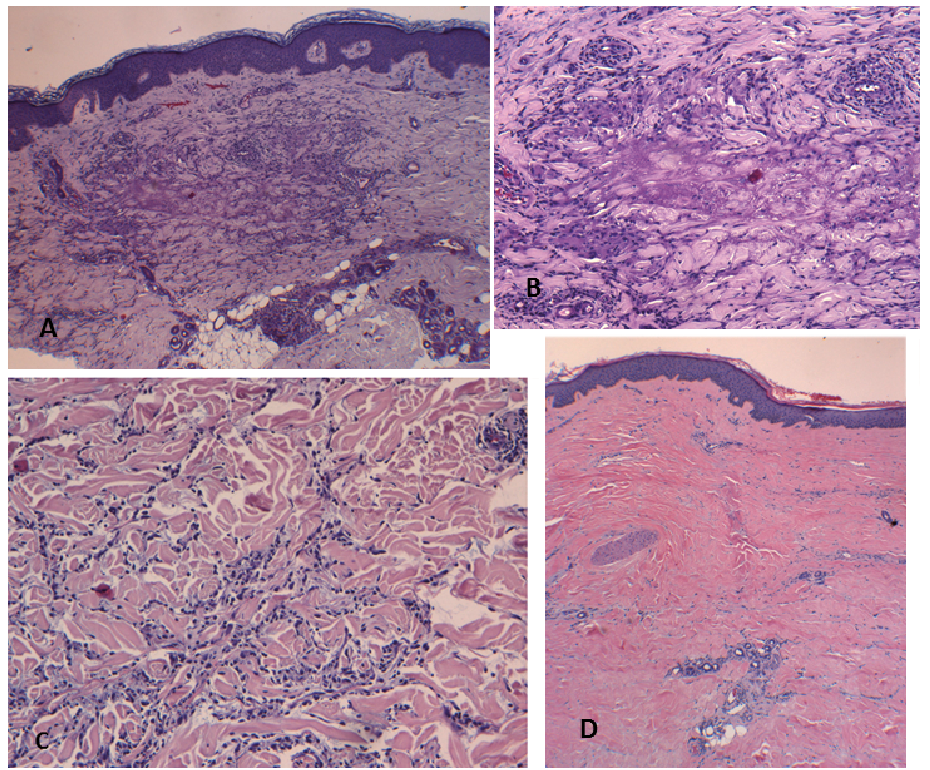 Click to show fullsize
Click to show fullsize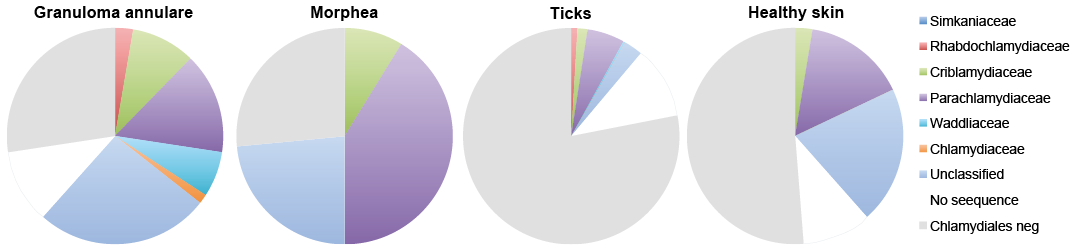 Click to show fullsize
Click to show fullsize