


Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, Denmark
Monitoring of biological treatment efficacy for psoriasis is based on clinical evaluation and patient’s quality of life. However, long-term correlation between Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI) in real life has not been studied in patients treated with ustekinumab. All patients with psoriasis treated with ustekinumab at our department were included (n = 120) in this study. Correlation analyses between the change in PASI and DLQI and the individual subquestions in DLQI were performed using Spearman’s rank correlation coefficient. A correlation value of 0.57 (p-value < 0.001) and 0.45 (p-value < 0.001) between PASI and DLQI were found in the period baseline – 4 months and baseline – 12 months, respectively. In DLQI subquestions, the greatest association was found for the questions on “Symptoms and feelings”. Objective improvements in the severity of psoriasis were weakly to moderately associated with improvements in quality of life in patients with psoriasis treated with ustekinumab.
Key words: psoriasis; PASI; DLQI; correlation; ustekinumab.
Accepted Oct 31, 2017; Epub ahead of print Nov 7, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Jeanette Halskou Hesselvig, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Kildegårdsvej 28, DK-2900 Hellerup, Denmark. E-mail: jeanette.halskou.hesselvig@regionh.dk
Initiation and evaluation of the effect of biologic treat-ment for psoriasis is based on clinical evaluation by the treating physician and on the patient’s quality of life (QoL). The Dermatology Life Quality Index (DLQI) is used to measure patient’s self-reported QoL. The severity of psoriasis lesions is often assessed with the Psoriasis Area and Severity Index (PASI) (1–3). During the first 10–16 weeks of biologic treatment, a strong correlation is seen between reduction in PASI and reduction in DLQI (4). In addition to improvements in the symptoms and severity of psoriasis, clinical trials with ustekinumab have shown an improvement in QoL (5, 6). However, to our knowledge, long-term correlation between PASI and DLQI has not been investigated in patients treated with ustekinumab. Moreover, it is unclear whether and how the individual subquestions in the DLQI questionnaire are correlated with PASI in patients with psoriasis.
The aim of the current study was therefore to examine the potential correlation between changes in DLQI and PASI in patients with psoriasis treated with ustekinumab by conducting a register-based cohort study in a single hospital clinic in Denmark.
The study was approved by the Danish Data Protection Agency (ref. HGH-2016-048, I-Suite: 04520). In Denmark, ethical approval is not required for registry studies. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies (STROBE) recommendations (7).
According to Danish guidelines, biologic therapy can be given to patients with moderate-to-severe psoriasis (defined as PASI > 10, DLQI > 10, or affected body surface area (BSA) > 10%), in whom previous conventional systemic treatments have failed, or for whom conventional systemic treatments are contraindicated (1).
The present study was a cohort study with data collected prospectively. All patients with plaque psoriasis treated with ustekinumab from the Department of Dermatology, Gentofte Hospital, Denmark, were included.
All of the patients who are treated with ustekinumab should have PASI and DLQI registered, at least at baseline, usually after 4 months, and then every year. Patients with missing baseline data either for DLQI or PASI were excluded. Ustekinumab has been available in Denmark since April 2009 (8). The last data entry in the present study was March 2017. Since 2012, the national guidelines have recommended ustekinumab as first-line biologic treatment for patients with moderate-to-severe psoriasis with no joint involvement, i.e. psoriatic arthritis or psoriatic arthropathy. Information on PASI and DLQI was obtained from the baseline (the date of first treatment with ustekinumab) and from the 4- and 12-month visits, respectively. Data were observational, from a real-life setting, and there was therefore no requirement for a wash-out period between the previous treatment and the start of treatment with ustekinumab.
The DLQI is an assessment tool with 10 questions, which is used to measure the effect of skin disease on the QoL of the patient (9). The DLQI total score ranges from 0 to 30, with 0 corresponding to no impairment of the QoL and 30 to maximum impairment due to the skin disease. The questions are divided into the following topics: “Symptoms and feelings” (questions 1 and 2), “Daily activities” (questions 3 and 4), “Leisure” (questions 5 and 6), “Work or school” (question 7.1 and 7.2), “Personal relationships” (questions 8 and 9), and “Treatment” (question 10) (9).
PASI is an index that is used to measure the severity of psoriasis lesions. It combines the severity of 3 clinical signs (erythema, induration (plaque thickness), and desquamation), the percentage of area affected, and the area factor (defined as head (10%), arms (20%), body (30%), and legs (40%)). PASI ranges from 0 (no psoriasis) to 72 (maximum) (2).
The primary outcome of this study was an assessment of the potential correlation between the reduction in psoriasis symptoms (PASI) and the reduction in QoL (DLQI) over time while treated with ustekinumab (baseline–4 months, baseline–12 months, and 4 months–12 months). The correlation was calculated as both the absolute reduction and the relative reduction in PASI and DLQI. The secondary outcome was the correlation between the absolute reduction in the PASI and the absolute reduction in the individual subquestions of the DLQI.
For continuous data, means with standard deviations (SDs) and medians with percentiles were calculated, and for categorical data, proportion (n) with percentage were calculated.
As the scores were not normally distributed, the correlation analyses between the changes in PASI and DLQI were performed using Spearman’s rank correlation coefficient (rs) (10). A 2-sided p-value <0.05 was considered statistically significant. Data were exported from an Excel file to SAS. All analyses were performed using SAS software version 9.2 (SAS Institute, Cary, NC, USA).
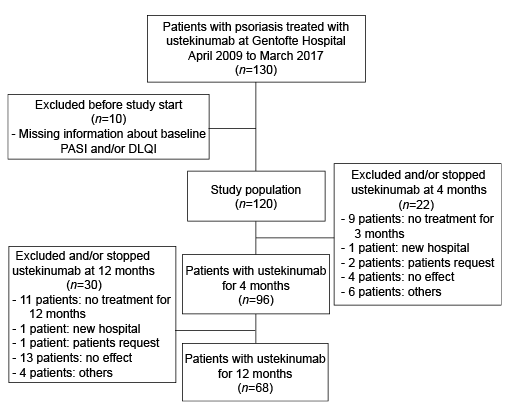
The study comprised a total of 120 patients with psoriasis who were treated with ustekinumab in the period April 2009 to March 2017. During the study period, 98 patients were treated with ustekinumab for at least 4 months and 68 patients were treated for at least 12 months (Fig. 1).
Fig. 1. Flow chart of selection of the study population.
Baseline characteristics are shown in Table I. A strong male predominance was seen (71.7%). Only one patient had recorded joint problems when starting treatment with ustekinumab, and 48.3% of the patients were bio-naïve.
Table I. Baseline characteristics of the study population
Median PASI and median DLQI at baseline, 4 months, and 12 months are shown in Fig. 2. A reduction in median PASI from baseline to month 4 and a subsequent slight reduction until month 12 were observed, showing objective improvements in the severity of psoriasis. A similar pattern was seen for DLQI, showing improvements in QoL.
Fig. 2. Median Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI) in the study population at baseline, month 4 and month 12.
The correlations between PASI and DLQI are shown in Table II, calculated as absolute reduction, relative reduction, and relative reduction in PASI and absolute reduction in DLQI. The greatest correlation was seen in the period from baseline to 4 months, rs = 0.48 (p-value < 0.001) and rs = 0.57 (p-value < 0.001) calculated for absolute and relative reductions, respectively. In the period from baseline to 12 months, the correlation between PASI and DLQI was weaker compared with the period from baseline to 4 months. All the correlation coefficients were statistically significant. Fig. 3 illustrates the correlation between the absolute reduction in PASI and DLQI.
Table II. Spearman’s rank correlation coefficients (rs) for the reduction in Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI) after treatment with ustekinumab
Fig. 3. Scatter plots illustrating the correlation between absolute reduction in Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI).
In general, women had a greater correlation between reduction in PASI and reduction in DLQI compared with men, remarkable after 12 months (women; rs = 0.60, p = 0.004, men; rs = 0.22, p = 0.138). No clear differences were seen in the results when stratifying for age (< 40 years and ≥ 40 years) (Table III).
Table III. Spearman’s rank correlation coefficients (rs) for the reduction in Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI) when stratifying for sex and age, respectively
No differences were observed in correlation between PASI and DLQI when stratifying patients based on their bio-naivety (Table IV).
Table IV. Spearman’s rank correlation coefficients (rs) for the reduction in Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI) when stratifying for bio-naïve and biologic-exposed
The correlations between the individual subquestions in DLQI and PASI are shown in Table V. The greatest correlation was seen in question 1 on “Symptoms and feelings”, mainly attributable to pruritus and pain. Overall, the numerically smallest correlations were seen in question 7 on “Work or school” and in question 8 on “Personal relationships”. Not all of the results in Table V were statistically significant.
Table V. The Spearman’s rank correlation coefficients for the individual questions in Dermatology Life Quality Index (DLQI) (questions 1–10) and Psoriasis Area and Severity Index (absolute reduction) in patients with psoriasis treated with ustekinumab
This Danish study of 120 patients treated with ustekinumab found that the objective improvements in the severity of psoriasis were weakly to moderately associated with the improvement in QoL. The greatest association was seen in the period from baseline to 4 months. Similarly, we found that the objective improvements in the severity of psoriasis were moderately associated with improvements in symptoms, such as pruritus and/or pain (question 1 on “Symptoms and feelings”). On the other hand, daily activities and treatment were weakly correlated with improvements in the severity of psoriasis.
A previous systematic review found a correlation coefficient value of 0.898 for relative reduction in PASI and absolute reduction in DLQI from baseline to 10–16 weeks after treatment (4). This correlation was stronger than our finding (rs = 0.45, p < 0.001). A possible explanation is that the studies were all clinical trials with highly selected patients, they all had a wash-out period after previous treatment, and they used a variety of different biologic drugs. Interestingly, some, but not all, studies have found a similar weak-to-moderate correlation between changes in PASI and changes in DLQI during short-term treatment (week 10–16) (11–13).
In our study, analyses of long-term treatment (baseline–12 months) showed only weak associations between improvements in the severity of psoriasis and improvements in QoL compared with the short-term treatment (baseline–4 months). Although speculative, the weak correlation seen after 12 months of treatment with ustekinumab could be due to a lack of consensus in the patients regarding what was an acceptable treatment response. Some patients are satisfied with a few remaining plaques and others want total clearance. Another explanation as to why the correlation between PASI and DLQI was generally weak-to-moderate could be that clinical outcome and QoL are not solely dependent on the severity of psoriasis. Indeed, Fig. 3 shows a high degree of heterogeneity and large distances from the trend line, suggesting that the association between PASI and DLQI may be influenced by other variables. Fig. 3 also illustrates that a number of patients have a large reduction in DLQI even with a small reduction in PASI during the course of treatment. This may be due to the localization of the plaques (e.g. genital plaques), where even a slight reduction in plaques can have potentially major importance for the patient.
In our analysis of the individual DLQI subquestions, “Symptoms and feelings” (question 1, dealing with pruritus and pain) showed the strongest association with objective improvements in the severity of psoriasis. Objective improvements in the severity of psoriasis resulted in almost twice the improvement in question 1 compared with the questions on leisure (questions 5 and 6). No previous studies have investigated the correlation between the individual DLQI subquestions and PASI over time in patients treated with ustekinumab. A clinical trial with patients with psoriasis treated with ixekizumab showed that pruritus is an important mediator of the association between PASI and DLQI (14).
Some limitations should be considered when interpreting the findings from this study: firstly, the low number of patients who were treated for 12 months. Secondly, when using the Spearman’s rank correlation coefficient it is not possible to adjust for confounders or to draw any conclusions about the causal relationship between PASI and DLQI.
One of the strengths of the study was the validated tools being used. PASI and DLQI are validated clinical measurement tools that are used extensively in clinical trials (3, 15). However, one reason for the correlations between PASI and DLQI not being stronger may have been the measurement tools, which were presumably not sufficiently accurate. PASI is not precise enough when describing low values and then subsequently comparing with DLQI, e.g. a single thick psoriasis lesion on the leg can result in a high PASI without the QoL of the patient being affected. Similarly, the DLQI questionnaire is developed for dermatological patients in general and not specifically for psoriasis. It is possible that a disease-specific measurement would be more sensitive to meaningful changes in the disease. Another strength was that the data came from a real-life setting, with the patients resembling those seen in the everyday clinic, thereby increasing the external validity of the current observations. Finally, the data were collected prospectively, thus eliminating potential recall bias.
We found that objective improvements in the severity of psoriasis were weakly to moderately associated with improvements in QoL over time in patients with psoriasis treated with ustekinumab. The strongest correlation between objective improvements in the severity of psoriasis and improvements in QoL was seen in the period from baseline to 4 months. In DLQI subquestions, the highest association was seen between objective improvements in the severity of psoriasis and the improvements in question 1 regarding pain and pruritus. Further studies are needed to investigate the causal relationship between PASI and DLQI.
The study was supported by an unrestricted grant from Janssen-Cilag.
Conflicts of interest. AE has received research funding from Eli Lilly and Pfizer, and honoraria as a consultant and/or speaker from Eli Lilly, Pfizer, Galderma, Novartis, and Janssen-Cilag. LS has been a paid speaker for Pfizer, AbbVie, Eli Lilly, Novartis, and LEO Pharma, and has been a consultant or has served on Advisory Boards with Pfizer, AbbVie, Janssen-Cilag, Novartis, Eli Lilly, LEO Pharma, and Sanofi. She has served as an investigator for Pfizer, AbbVie, Eli Lilly, Novartis, Amgen, Regeneron, and LEO Pharma and has received research and educational grant from Pfizer, AbbVie, Novartis, Sanofi, Janssen-Cilag and LEO Pharma. KK has been a paid speaker for AbbVie, Eli Lilly, LEO Pharma, Meda, Sanofi-Pasteur, Merck, and Gilead and has been a consultant or has served on Advisory Boards with AbbVie, Janssen-Cilag, Novartis, and Celgene. He has served as an investigator for Novartis and has received research grants from Sanofi-Pasteur. CZ has consulting relationships and/or is an investigator and/or has received grants or honoraria from Eli Lilly, Janssen-Cilag, Novartis, AbbVie, Takeda, Amgen, MSD, LEO Pharma, and Regeneron and has served as an investigator for Pfizer, AbbVie, Eli Lilly and Company, Novartis, Amgen, Regeneron and LEO Pharma. The other authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize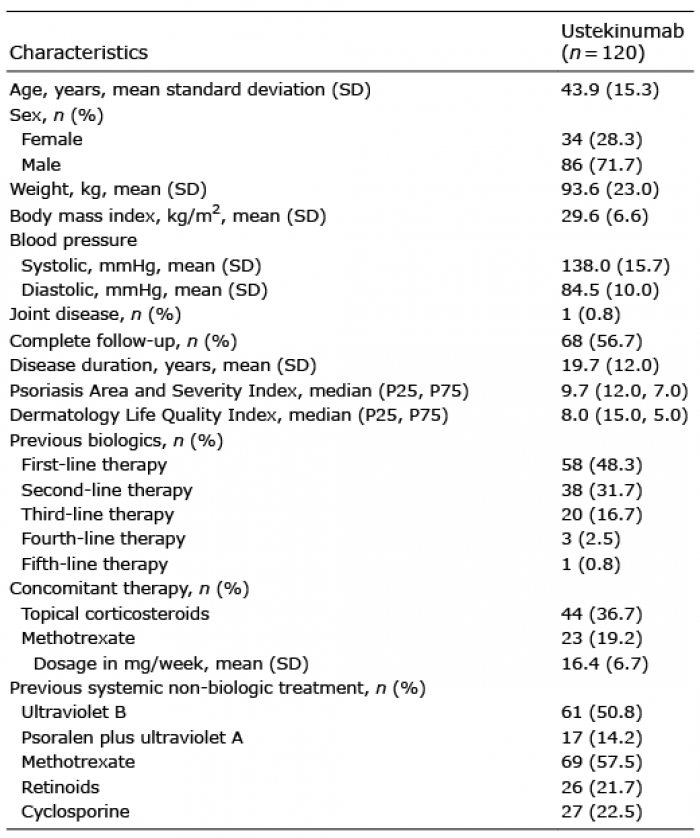 Click to show fullsize
Click to show fullsize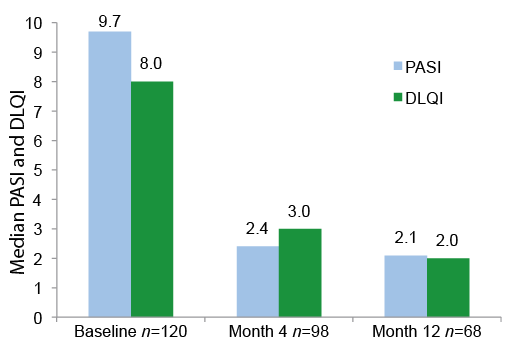 Click to show fullsize
Click to show fullsize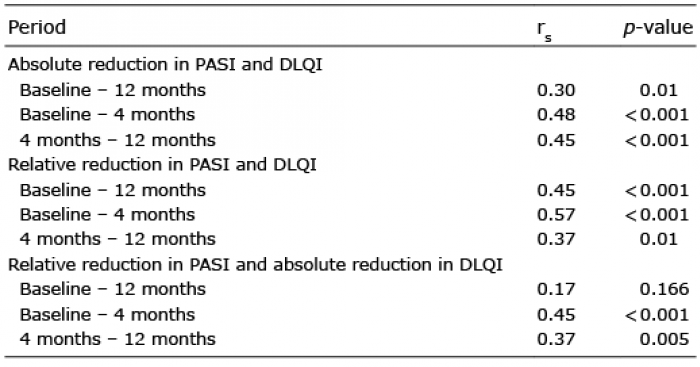 Click to show fullsize
Click to show fullsize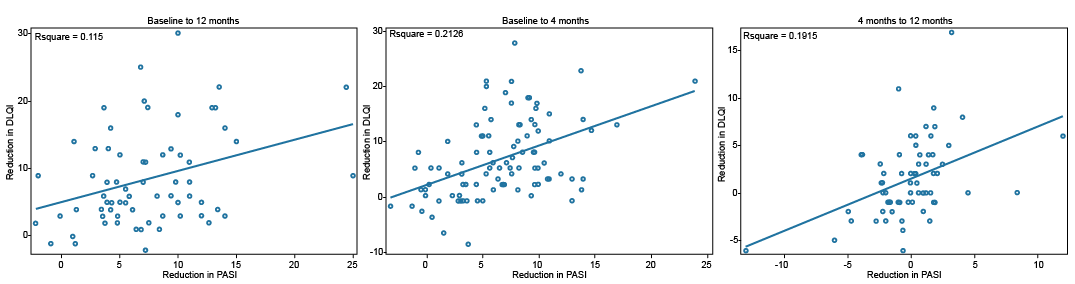 Click to show fullsize
Click to show fullsize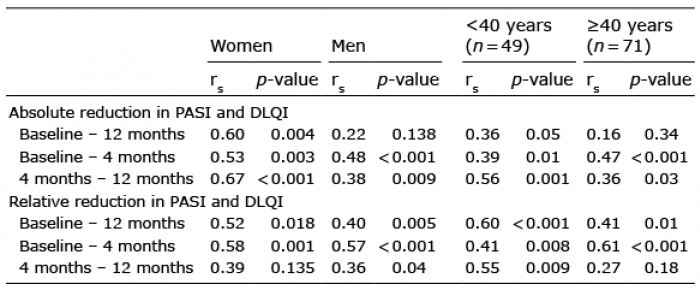 Click to show fullsize
Click to show fullsize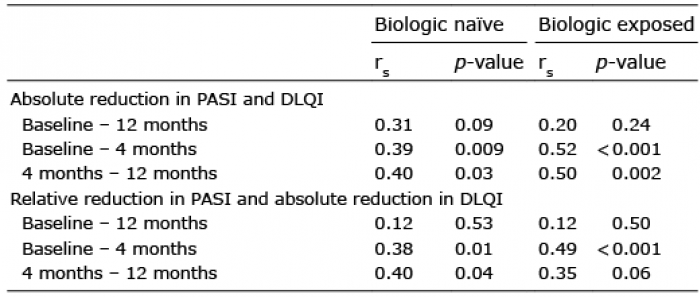 Click to show fullsize
Click to show fullsize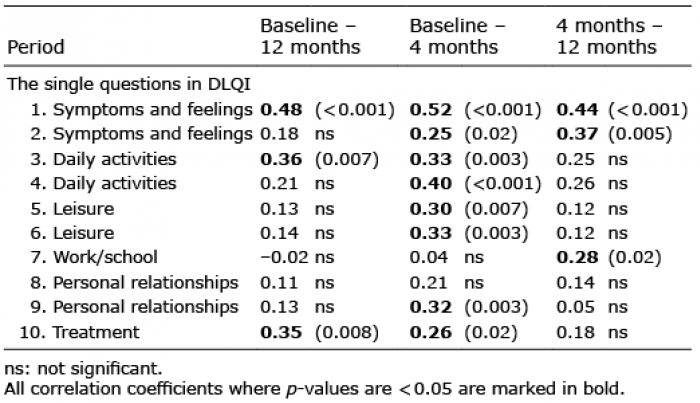 Click to show fullsize
Click to show fullsize