


1Infectiology and Dermatology and 2Bacteriology Laboratory, Hospital of Fréjus-Saint-Raphël, 240 avenue Saint Lambert, FR-83600 Fréjus, 3National Reference Center of Streptococcus, Universitary Hospital Paris Center, site Cochin, AP-HP, Team «Barrière et Pathogènes», Cochin Institute, Inserm 1016, CNRS UMR 8104, 4Paris Descartes University, Paris, France. E-mail: del-giudice-p@chi-fsr.fr
Accepted Nov 2, 2017; Epub ahead of print Nov 7, 2017
Infectious cellulitis is mainly caused by Streptococcus pyogenes or Staphylococcus aureus (1, 2). Other less frequently isolated bacteria include Pasteurella from animal bites, non-typable streptococci or Bacillus anthracis in intravenous drug users, Vibrio spp. or Aeromonas spp. due to skin wounds in sea water (1, 2). We present here, to our knowlegde, the first human case of a cellulitis caused by a new pathogen, Streptococcus halichoeri.
An 84-year-old man was hospitalized due to bacterial cellulitis of his left thigh in November 2015. His past medical history was marked by obesity, diabetes mellitus treated with gliclazide, insulin and metformin, dyslipidaemia treated with atorvastatin, hypertension treated with bisoprolol and perindopril, hyperuricaemia treated with allopurinol, atrial fibrillation, and prostatic adenocarcinoma treated with surgery and radiotherapy. Sixteen months earlier he had been hospitalized due to cellulitis in the same location. Streptococcus agalactiae was isolated from blood cultures. Cardiac ultrasonography revealed left-sided endocarditis and the patient was treated with parenteral amoxicillin (100 mg/kg) associated with gentamicin (3 mg/kg) for 15 days, followed by oral amoxicillin alone for one month. The outcome was favourable. An infected chronic ulcer of the left leg was thought to be the likely route of entry of infection.
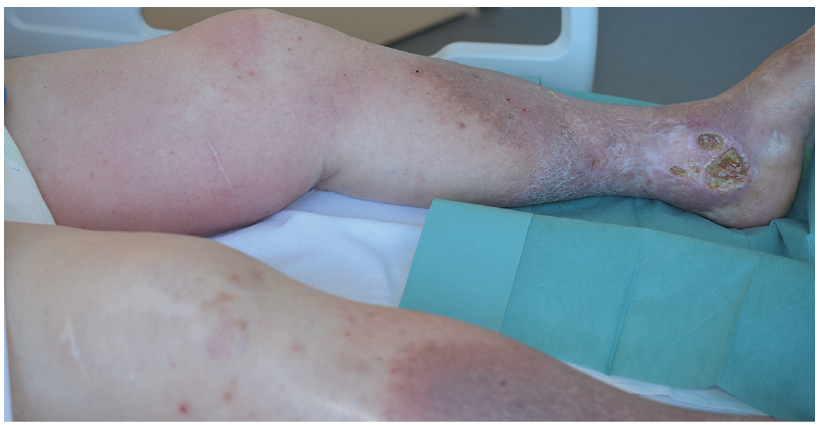
The new hospitalization, 16 months later, was marked by cellulitis of the thigh in the same location with persisting chronic ulceration of the left leg (Fig. 1). On admission, the patient’s body temperature was 38.5°C, associated with a large erythematous skin plaque on his thigh consistent with bacterial skin cellulitis. The patient was treated empirically with intravenous amoxicillin (100 mg/kg). Blood cultures, and samples from the leg ulcer, grew non-haemolytic colonies on sheep-blood agar plates. Gram-staining revealed Gram-positive cocci, in chains. The identification results were discordant: S. pyogenes (91% probability) by VITEK 2 Gram-positive card system (bioMérieux, Marcy l’Etoile, France) and S. agalactiae (unacceptable profile) by Api 20 STREP gallery (bioMérieux, Marcy l’Etoile, France). The bacteria grouped with Lancefield type B antisera (Streptococcal Grouping Latex Kit, DiaMondial, Vienna, Austria). Recurrence of the endocarditis was eliminated by normal endoesophageal and transthoracic echographies. The outcome was favourable after 15 days’ treatment with 100 mg/kg amoxicillin.
Fig. 1. Clinical characteristics. Cellulitis of the left thigh, with chronic ulceration of the lower leg.
All the strains isolated during both episodes were sent to the French Reference Center for Streptococci for expert analysis (CNR-Strep; https://www.cnr-strep.fr/). Strains isolated during the first episode grew beta-haemolytic colonies on horse-blood agar plates. The bacteria were catalase-negative, Gram-positive cocci, in chains, Lancefield grouping with type B antisera (Remel™ PathoDxtra™ Strep Grouping Kit), giving typical orange pigmented colonies on Granada-based media plate (Granada™, bioMérieux, Marcy l’Etoile, France) and identified as S. agalactiae (score 2.43) by MALDI-TOF MS (Matrix Assisted Laser Desorption Ionisation Time Of Flight) mass spectrometry (Bruker™). Molecular characterization identified a capsular serotype III strain (3). Antimicrobial drug-susceptibility testing performed according to the European Committee on Antimicrobial Susceptibility Testing guidelines (http://www.eucast.org) characterized the strains as susceptible to penicillin (minimum inhibitory concentration (MIC) ≤ 0.25 mg/l), erythromycin, clindamycin, levofloxacin, tetracycline, and linezolid. Strains isolated from blood culture and wound sample during the second episode both grew non-haemolytic and non-pigmented colonies on horse-blood agar plates and Granada™ plates, respectively. Both bacteria were catalase-negative and Gram-positive cocci in chains. They were identified as S. halichoeri (score 2.21 and 2.43, respectively) by MALDI-TOF MS and as S. suis serotype 1 (87% probability) by VITEK 2 Gram-positive card system (bioMérieux, Marcy l’Etoile, France). MALDI-TOF MS allows a rapid and precise microbial identification and strain typing. It is an analytical technique in which chemical compounds are ionized into charged molecules and the ratio of their mass to charge (m/z) is measured. A characteristic spectrum, called a peptide mass fingerprint (PMF), is then generated. Identification of microbes by MALDI-TOF MS is carried out by comparing the PMF of the unknown organism with the PMFs in the database (4).
Molecular identification at the species-level was carried out by sodA gene and 16S ribosomal RNA gene sequencing (5, 6). Sequence analysis yielded 100% identity over 438 bp with the sodA gene sequence of the S. halichoeri strain SS1939 (KP890268 NCBI database) and 99% identity over 971 bp with the 16S ribosomal RNA gene of the S. halichoeri type strain SS1844 (KP851845 NCBI database), allowing definite identification of S. halichoeri. Antimicrobial drug-susceptibility testing characterized the strains as susceptible to penicillin (MIC≤0.25 mg/l), levofloxacin, and linezolid and resistant to erythromycin, clindamycin and tetracycline, due to the presence of erm(B) and tet(O) antibiotic-resistant genes, respectively (7). Thus, the second episode was not a recurrence of S. agalactiae infection, but bacteraemic cellulitis due to S. halichoeri.
S. halichoeri was first reported in 2004 from UK veterinary laboratories in wounds in seals (8–11). In 2014 Foo & Chan (12) reported the first case of human infection caused by this bacterium in a 45-year-old Chinese male from Singapore who had a postoperative empyema. The current patient is retired with no known contact with seals or other sea animals. We report here the first human case of skin cellulitis. Foo & Chan (12) emphasized that other zoonotic streptococci, including Streptococcus canis, Streptococcus equi subsp. zooepidemicus, Streptococcus iniae, and Streptococcus suis, are emerging pathogens in humans. On the basis of phenotypic, genotypic and antimicrobial comparison of S. halichoeri characteristics isolated from a seal and from 6 human clinical isolates (4 from blood, 1 from osteitis and 1 from maxillary sinus), Shewmaker et al. (13) proposed in a recent study that S. halichoeri should be divided into 2 subspecies; S. halichoeri subsp. hominis, for the human isolates and S. halichoeri subsp. halichoeri for the grey seal isolates. In their study none of the 6 human isolates were isolated from cellulitis. The phenotypic and genetic characterization of our strains is similar to the results already obtained with S. halichoeri isolated from human isolates. These results lead us to suggest that these strains belong to the S. halichoeri subspecies hominis. To our knowledge, this is the first report of a human case of an infectious cellulitis and skin infection due to S. halichoeri. Increased vigilance is needed to evaluate the emergence of this pathogen in human medicine.


 Click to show fullsize
Click to show fullsize