


Departments of 1Dermato-Allergology, 3Rheumatology and 4Cardiology, Herlev and Gentofte University Hospital, Copenhagen, Denmark, 2Department of Dermatology, Kaiser Permanente Los Angeles Medical Center, Los Angeles, CA, USA, and 5Department of Cardiology, Odense University Hospital, Odense, Denmark
Recent findings indicate that patients with systemic sclerosis have an increased risk of cardiovascular disease. To determine whether patients with systemic sclerosis or localized scleroderma are at increased risk of cardiovascular disease, a cohort study of the entire Danish population aged ≥ 18 and ≤ 100 years was conducted, followed from 1997 to 2011 by individual-level linkage of nationwide registries. Multivariable adjusted Cox regression models were used to estimate the hazard ratios (HRs) for a composite cardiovascular disease endpoint. A total of 697 patients with localized scleroderma and 1,962 patients with systemic sclerosis were identified and compared with 5,428,380 people in the reference population. In systemic sclerosis, the adjusted HR was 2.22 (95% confidence interval 1.99–2.48). No association was seen between patients with localized scleroderma and cardiovascular disease. In conclusion, systemic sclerosis is a significant cardiovascular disease risk factor, while patients with localized scleroderma are not at increased risk of cardiovascular disease.
Key words: localized scleroderma; systemic sclerosis; cardiovascular risk; cardiovascular disease; inflammation; epidemiology.
Accepted Nov 13, 2017; Epub ahead of print Nov 14, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Kristian Kofoed, Department of Dermato-Allergology, Herlev and Gentofte University Hospital, Kildegaardsvej 28, DK-2900 Hellerup, Denmark. E-mail: kristian.kofoed@regionh.dk
Recent findings indicate that patients with systemic sclerosis (SSc) have an increased risk of cardiovascular disease (CVD) (1, 2), but population-based cohort studies are lacking (3, 4). In addition, little is known about the risk of CVD in patients with localized scleroderma (LS).
SSc is a chronic autoimmune disease characterized by fibrosis of the skin and internal organs. LS, also known as morphea, is characterized by excessive deposition of collagen leading to thickening of the dermis, subcutaneous tissues, or both. Depending on the subtype and site affected, adjacent structures, such as adipose tissue, muscles, joints and bones, may be involved, but the internal organs are not affected and no progression to SSc occurs (5).
Other autoimmune diseases, such as rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE), are associated with increased risk of developing CVD (6–8). One of the reasons for this association is related to chronic inflammation that predisposes to atherosclerosis (9–12).
The aim of this Danish nationwide cohort study was to determine whether patients with LS and SSc have increased risk of CVD and all-cause mortality, compared with the general population, based on the unique Danish Health registers.
The study was approved by the Danish Data Protection Agency. In Denmark, ethics committee approval is not required for register studies. The following registries were used: the Civil Registration System, which holds information on patient date of birth, sex and vital status (13); the National Patient Registry, which holds information on all inpatient and outpatient visits to Danish hospitals since 1978, with diagnoses according to the International Classification of Diseases (ICD) (prior to 1994, according to the 8th revision (ICD-8) and thereafter the 10th revision (ICD-10)) (14), which was used to identify patients with scleroderma and to obtain information on comorbidity; and the Registry of Medicinal Product Statistics, which holds information on all prescription claims since 1995 (15). All drugs are classified according to the Anatomical Therapeutical Chemical (ATC) classification. Pharmacies in Denmark are required to register all dispensed prescriptions.
Data on death (16), comorbidity, concomitant medication and socioeconomic status (17) were linked at the individual level.
The study population comprised all Danish citizens ≥ 18 and ≤ 100 years of age from 1 January 1997 to 31 December 2011. All residents in Denmark have a 10-digit personal identification number, which is the same throughout all national registries, and hence register linkage is possible.
Patients with a diagnosis of LS were identified by ICD-10: DL940 localized scleroderma, DL940B sclerodermia circum-scripta or DL941 scleroderma lineare, and patients with SSc by ICD-10: DM340 progressive systemic scleroderma, DM348 other forms of systemic scleroderma, DM348B systemic scleroderma with acrosclerosis or DM349 systemic sclerosis unspecified. It was decided not to include patients with DM342 systemic scleroderma caused by drugs or chemicals, DL903 Pasini-Pierinis atrophoderma, and DM341 CREST syndrome because of discrepancies in how these codes were used. Patients with a history of CVD prior to the beginning of the study were excluded.
The baseline (up to 6 months prior to inclusion) pharmacological treatment was identified by patient prescriptions (from the Danish Registry of Medicinal Product Statistics) for: platelet inhibitors (ATC classification code: B01AC), beta-blockers (C07), renin-angiotensin-aldosterone system inhibitors (C09), calcium antagonists (C08), loop diuretics (C03C), thiazide diuretics (C03A), spironolactone (C03D), cholesterol-lowering drugs (C10A), glucose-lowering drugs (A10), non-steroidal anti-inflammatory drugs (NSAID) (MA01A), antidepressants (N06A), and anti-thyroid drugs (H03B).
Baseline comorbidity was defined by hospitalization (in the Danish National Patient Registry) up to 12 months prior to inclusion, according to the previously validated Charlson comorbidity index. The comorbidity index is the established sum for the 19 included clinical conditions, which were given weights ranging from 1 to 6, as follows: 1: myocardial infarct, congestive heart failure, peripheral vascular disease, dementia, cerebrovascular disease, chronic lung disease, connective tissue disease, ulcer, chronic liver disease, diabetes; 2: hemiplegia, moderate or severe kidney disease, diabetes with end-organ damage, tumour, leukaemia, lymphoma; 3: moderate or severe liver disease; and 6: malignant tumour, metastasis, or acquired immunodeficiency syndrome (AIDS) (18).
The primary endpoint of the study was a composite of cardiovascular death (ICD-10 I00-I99), myocardial infarction (ICD-10 I21 and I22) and stroke (ICD-10 I60, I61, I63 and I64). The secondary endpoint, all-cause mortality, was examined. Previous studies have demonstrated that diagnoses of acute myocardial infarction (AMI) and stroke in the Danish registries are accurate (19, 20).
Patients were followed from 1 January 1997 or on the subsequent day that the subjects reached 18 years of age, and were censored on 31 December 2011 or during follow-up, if an event or death occurred. Event rates per 1,000 person-years and 95% confidence intervals (95% CIs) were calculated for patients with LS, SSc, and for the reference population, respectively. Multivariable adjusted Cox regression models were used to estimate hazard ratios (HRs) and 95% CIs. We adjusted for a priori defined confounding factors, including age, calendar year, concomitant medication, comorbidity, socioeconomic status and sex. The comorbidity index score was incorporated into the model as a continuous variable and concomitant medication as a dichotomous variable. LS and SSc status at a given age were included as time-dependent variables, to ensure accurate allocation of time at risk. Comorbidity, use of medication and socioeconomic status were included as fixed variables obtained at baseline. Socioeconomic status was defined according to the mean yearly income in the 5 years preceding the beginning of the study, divided into quintiles. One-year time bands were created and the patient’s age was updated at each time-band. In addition, all analyses were repeated with inclusion of prescription drug use as a time-dependent variable, to ensure inclusion of continuously updated information on comorbidities in the analyses. A 2-sided p-value < 0.05 was considered statistically significant. All analyses were performed with the use of SAS software (Version 9.2, SAS Institute, Cary, NC, USA), and Stata software (Version 11.0, StataCorp, College St., TX, USA).
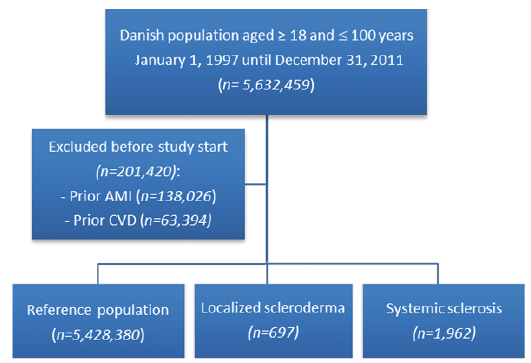
The study comprised a total of 697 patients with LS, 1,962 with SSc and 5,428,380 in the reference population (Fig. 1). The incidence rate (IR) of LS was 1.1 per 100,000 person-years and 3.1 events per 100,000 person-years for SSc.
Fig. 1. Flowchart of the study population. AMI: acute myocardial infarction; CVD: cardiovascular disease.
The baseline characteristics of the study population are shown in Table I. Follow-up time, number of events and incidence rates (IRs) are shown in Table II.
Table I. Baseline characteristics of the study population
Table II. Follow-up time (person-years), number of events and incidence rates per 1,000 person-years
Patients with SSc were associated with a significantly increased risk of CVD and all-cause mortality (Table III). In this group the adjusted HRs were 2.22 (95% CI 1.99–2.48) and 2.66 (95% CI 2.45–2.90) for composite CVD and all-cause mortality, respectively.
Table III. Hazard ratio (HR) and 95% confidence interval (CI) for composite cardiovascular disease (CVD) endpoint and all-cause mortality for patients diagnosed with localized scleroderma and systemic sclerosis and adjusted for age, calendar year, concomitant medication, comorbidity, socioeconomic status and sex
No association was found between patients with LS and CVD or all-cause mortality. In patients with LS, the HRs for composite CVD endpoint and all-cause mortality were comparable to the HRs in the reference population.
The inclusion of prescription drug use as time-dependent information on comorbidities in the analyses did not significantly alter the results. In the sensitivity analyses, the HR for the composite CVD endpoint for patients with LS was 0.89 (95% CI 0.67–1.18), compared with 0.96 (95% CI 0.72–1.27) in the main analyses; and for patients with SSc, the HR was 2.11 (95% CI 1.89–2.36), compared with 2.22 (95% CI 1.99–2.48) in the main analyses.
Similarly, there was no difference in the results when stratifying the data into age categories (data not shown).
In this Danish nationwide cohort study, SSc was a significant cardiovascular risk factor for the composite endpoint of stroke, myocardial infarction, and cardiovascular death, and for all-cause mortality. Patients with LS were not at increased risk for CVD and did not have increased all-cause mortality, compared with the general population.
The reason for the increased risk of CVD in patients with SSc is not clear. Atherosclerotic CVD may be due to the chronic inflammation (3, 9), as seen in other autoimmune diseases (6, 8) besides the traditional cardiovascular risk factors. Similarly, pulmonary hypertension and pulmonary fibrosis are probably part of the explanation for the increased risk of CV death in these patients.
Chronic inflammation predisposes to atherosclerosis, which is the hallmark of CVD (9–12). A systematic review from 2011 concluded that patients with SSc had increased atherosclerosis compared with healthy individuals (21). Other mechanisms, by which atherosclerosis is believed to be promoted in connective tissue diseases is due to altered lipid profiles and function, autoantibodies and endothelial dysfunction (3, 4, 22).
The survival of patients with scleroderma has improved over the past 30 years. Fewer scleroderma-related deaths are being reported, with patients living longer despite having the disease. Pulmonary hypertension and pulmonary fibrosis are the primary cause of scleroderma-related deaths today (23).
No association was seen between CVD and patients with LS. In LS, the risk of having a composite CVD endpoint was the same as in the general population. This is in contrast to findings in patient with cutaneous lupus erythematosus without systemic involvement and in patients with psoriasis (8, 24). Indeed, the results indicate LS as being a disease limited to the skin without any systemic effect.
In previous studies, SSc is mentioned as a cardiovascular risk factor, and the risk of these patients having CVD is increased (2, 25, 26). In our study, the HR of the composite CVD endpoint was 2.2-fold higher for patients with SSc, compared with the general population in Denmark. A study from a UK database found an adjusted HR for AMI or stroke of 2.16 (95% CI 1.49–3.14) (2), a study from Canada showed an adjusted HR for CVD of 2.70 (95% CI 2.07–3.51) (25) and a meta-analysis found a risk of ischaemic stroke with a pooled risk ratio of 1.68 (95% CI 1.26–2.24) (26). All results were in agreement with our findings for patients with SSc. Similarly, the HR for all-cause mortality in patients with SSc is in agreement with earlier finding (27).
A Swedish study examined whether there was an association between hospital admission in a variety of immune-mediated diseases, one of which was LS, and subsequent risk of hospitalization for coronary heart disease (CHD) (28). The study did not show any clear results for LS. Depending on the division of the data, the risk of having CHD was either increased or decreased. If the age at diagnosis of CHD was < 50 years then the standardized incidence ratio (SIR) for subsequent CHD, after one year of follow-up, was 0.98 (95% CI 0–5.62), and if the age at diagnosis of CHD was ≥ 70 years then the SIR was 1.28 (95% CI 1.28–1.49) after one year of follow-up. Our study did not find an increased risk when the data were stratified into age categories. In the Swedish study, the overall SIR for CHD for patients with LS was 1.24 (95% CI 1.07–1.43); however, the majority of the results were not significant. In addition, the study was limited by low numbers of participants with LS, and it only included hospitalized patients with LS; hence, it might not represent the risk of developing CHD for all patients with LS, as most patients with LS are not hospitalized (28). Our study included both inpatients and outpatients and the LS group comprised almost 3.5-fold as many patients. The same authors performed a similar study, in which the endpoint was ischaemic and haemorrhagic stroke (29). The trend for LS was the same, with several insignificant results and a low numbers of participants.
The present study has some limitations. No data on traditional cardiovascular risk factors, such as body mass index, diet and smoking, were included. Information on smoking is not available in the databases; however, we indirectly adjusted for smoking using socioeconomic status and via chronic obstructive pulmonary disease (30, 31).
Another limitation is that some patients with LS are followed by their private dermatologist or general practitioner, and our results cannot be generalized to these patients. However, the most severely affected patients are followed at a hospital. Misclassification of patients with LS as references would tend to bias the results towards having no differences in risk of CVD. Moreover, this limitation should not be present in patients with SSc, as, in Denmark, they are traditionally followed at a hospital. A further limitation is that we did not evaluate the different subtypes of LS.
The diagnoses of LS and SSc in the Danish National Patient Registry have not been validated previously. We found IRs of 1.1 per 100,000 person-years and 3.1 events per 100,000 person-years for LS and SSc, respectively. Previously reported IRs varied greatly according to the geographical location and study design (32–35). Our IRs are not directly comparable with the findings of previous studies due to different geographical location, calendar-year and study design, but the results are almost in agreement with earlier findings (32–35).
We did not investigate change in CVD during the study period.
The use of the Charlson comorbidity index as a summary score to adjust for comorbidities is widely accepted; however, it is important to acknowledge that the index has not been validated in selected populations without previous cardiovascular events and may not be an accurate predictor of mortality in this setting.
The Danish population is predominantly of Caucasian descent, and extrapolation of results to patients of other ethnicities should be carried out with caution. Ethnicity affects the incidence and prevalence, with Afro-Americans having higher incidence and prevalence than Caucasians (33).
The large number of participants, the nationwide coverage of recorded registries, no loss to follow-up and the long duration of the follow-up period represent major strengths. The nationwide coverage minimized selection bias, compared with data obtained from highly specialized centres. Also, the use of nationwide, prospectively recorded registries eliminated recall bias. Finally, the results were supported by the sensitivity analyses accounting for changes in comorbidities during follow-up and stratification of age.
In this nationwide study, SSc, but not LS, was a significant cardiovascular risk factor for the composite endpoint of stroke, myocardial infarction, and cardiovascular death, and for all-cause mortality.
Patients with SSc should be advised and evaluated regarding traditional cardiovascular risk factors, so that the overall risk for the individual patient can be determined. It is new and useful knowledge that patients with LS do not have increased risk for CVD and reassuring that these patients can follow the same guidelines as the general population.


 Click to show fullsize
Click to show fullsize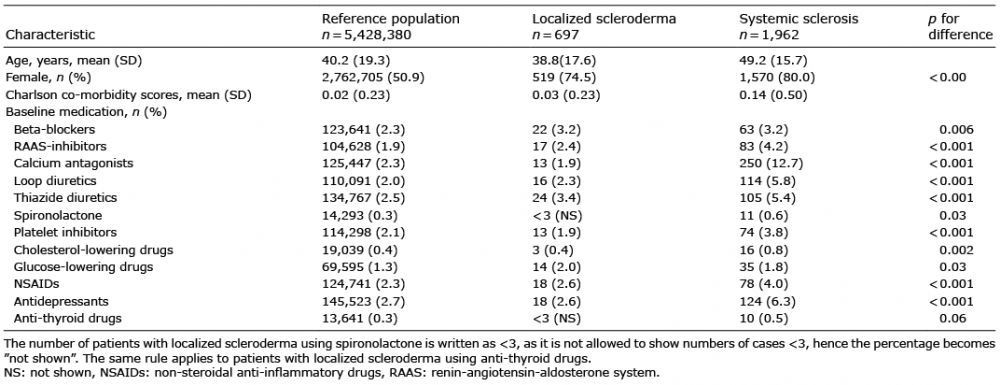 Click to show fullsize
Click to show fullsize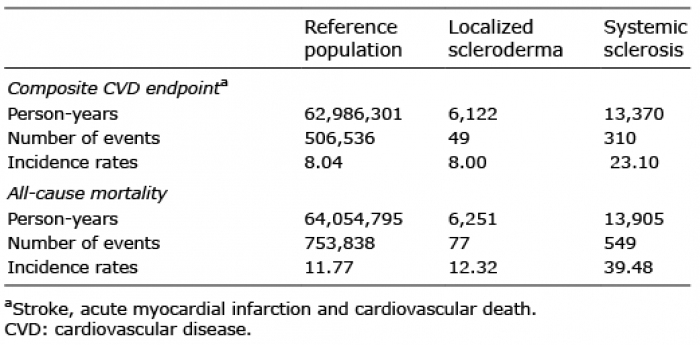 Click to show fullsize
Click to show fullsize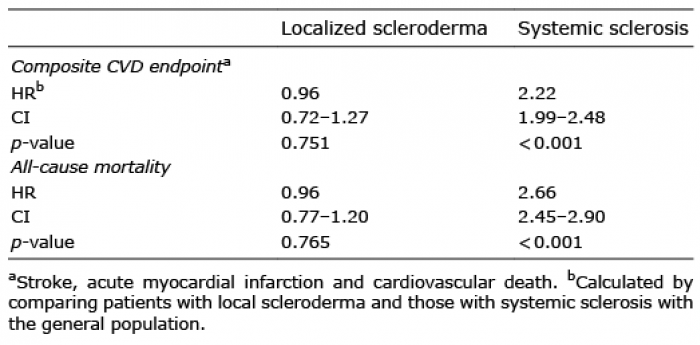 Click to show fullsize
Click to show fullsize