


1Department of Dermatology, 2GROW, School for Oncology and Developmental Biology, Maastricht University Medical Centre, Maastricht, 3Department of Dermatology, Flevo Hospital, Almere, 4Department of Epidemiology, CAPHRI, School for Public Health and Primary Care, Maastricht University, Maastricht, The Netherlands
Current literature on risk factors for surgical site infection (SSI) in dermatological surgery in the absence of antibiotic prophylaxis is limited. The aim of this study was to retrospectively evaluate patients presenting for dermatological surgery. A total of 1,977 procedures were reviewed. SSI was clinically suspected in 79 (4.0%) patients and confirmed by culture in 38 (1.9%). Using the strictest definition of SSI (clinical symptoms with positive culture) significantly higher risk of SSI was found for location on the ear (odds ratio (OR) 6.03, 95% confidence interval (95% CI) 2.12–17.15), larger defects (OR 1.08 per cm2 increase, 95% CI 1.03–1.14), closure with flaps (OR 6.35, 95% CI 1.33–30.28) and secondary intention (OR 3.01, 95% CI 1.11–8.13). These characteristics were also associated with higher risk of clinically suspected SSI regardless of culture results with slightly lower ORs. In conclusion, the risk of acquiring a SSI is increased in surgeries performed on the ear, in larger wounds and in defects closed with flaps or healed by secondary intention.
Key words: surgical site infection; wound healing; antibiotic prophylaxis; dermatological surgery.
Accepted Nov 13, 2017; Epub ahead of print Nov 14, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Xiaomeng Liu, Department of Dermatology, Maastricht University Medical Centre, P. Debyelaan 25, NL-6229 HX Maastricht, The Netherlands. E-mail: xmxmliu@gmail.com
Increasing numbers of patients with skin malignancies requiring surgical treatment are presenting to dermatologists worldwide (1, 2). These procedures are generally associated with a low risk (< 5%) of surgical site infection (SSI) (3–10). However, there is ongoing debate that, under certain circumstances, the risk of SSI is significantly increased and could surpass the acceptable threshold.
Different factors could influence the risk of SSI after dermatological surgery. The first group consists of “patient-related factors”, which include diabetes and immunological status. The impact of these factors on the risk of SSI in dermatological surgery is a matter of debate (5–7, 9). The second group of potential risk factors are “procedure-related factors”, such as environmental circumstances, type of procedure and method of closure. Several studies have compared the risk of SSI after Mohs micrographic surgery (MMS) and excision and found no significant difference (6–8). Studies have not reached consensus as to whether the method of closure is a significant independent risk factor (6, 7, 9, 10). The last and most studied group consists of “lesion-related factors”, such as anatomical site and defect size. Regarding anatomical site, the nose, ears, genital/groin, and location below the knees and on extremities have been identified as risk factors in various studies (3, 6–8, 11). Several studies have also shown that larger defects are associated with an increased risk of SSI (4, 8, 11).
Many published studies evaluating risk factors in dermatological surgery have included a group of patients who received antibiotic treatment during the perioperative period. To our knowledge, the only large study including patients who did not use antibiotics was published by Dixon et al. in 2006, including 5,091 procedures in 2,424 patients (6). Although the study presented an in-depth evaluation of different risk factors for SSI, no multivariate analysis was performed to assess the independent effect of risk factors. Routine use of antibiotic prophylaxis should be avoided, as this could lead to adverse reactions and increase bacterial resistance. In 2008, an advisory statement in the USA was published on this topic, suggesting antibiotic prophylaxis be used for certain patients or operations on high-risk locations (12). The authors, however, emphasized that the avail-able evidence was limited, and encouraged researchers to further identify important risk factors.
The aim of this study was to perform a comprehensive evaluation of the independent effect of multiple risk factors on the risk of SSI, using a multivariate approach in patients not receiving any antibiotics in the perioperative period.
An observational cohort study was conducted at the Department of Dermatology, Maastricht University Medical Centre for one year. All patients who received surgery under local anaesthesia were eligible. A waiver to obtain written informed consent was authorized by the local ethics committee as the study protocol did not differ from standard care. Biopsies, curettages, shave-excisions or laser procedures were excluded. Patients who received antibiotics in the perioperative period (1 month prior to or after the procedure) were also excluded.
Data on patient-related characteristics (age, sex, diabetes and immunosuppression), surgical procedure characteristics (setting, number of separate procedures on one day, type of procedure and type of closure) and lesion-related characteristics (type, location and defect size) were collected retrospectively from the electronic patient charts.
Surgical procedures were performed at 2 locations. At the operation theatre, both the patient and healthcare professionals were dressed in clean surgical gowns. The surgeons and assistants wore scrub hats, masks and sterile gloves. If the operation involved a large skin tumour, sterile gowns were also worn. In the outpatient clinic, patients wore their own clothing. The healthcare professionals wore clean surgical gowns, scrub hats, masks and sterile gloves. In both locations, the surgical site was prepared under sterile conditions. During conventional excision the surgical site was disinfected once, prior to incision, with chlorhexidine digluconate 0.5% solution in ethanol 70%. Local anaesthesia was achieved with lidocaine hydrochloride 1% and adrenaline 1:100,000 injections. In case of MMS, the surgical site was disinfected prior to each stage. After every stage the wound was dressed with sterile gel with 0.5% chlorhexidine and sterile gauze. Instruments were changed after every third stage or before closure when more than one stage was performed with the same instruments.
Wounds were sutured in layers with dermal absorbable sutures and cutaneous sutures. The sutured wounds were supported by adhesive closure strips and a clean pressure dressing. Patients were advised to keep the wounds dry until suture removal (approximately one week on the face and 2 weeks on the trunk). Open wounds were dressed with paraffin-impregnated gauze for 3–7 days. After these first days, patients were instructed to rinse the wound daily with clean tap water.
Most patients received follow-up at least until suture removal. Patients who had not returned for suture removal were contacted by phone and questioned about adverse events. In case of an adverse event, patients had follow-up until the wound had healed. At the start of the study, all doctors working at the department received instructions on the definition of SSI and were asked to obtain wound cultures in case a SSI was suspected. Two definitions of SSI were used. According to the strictest definition, a SSI required local symptoms indicative of wound infection (purulent drainage, pain, swelling, erythema and/or heat) combined with a positive culture occurring within 30 days after the surgery. Wound culture was considered positive if it yielded appropriate pathogenic bacteria and was interpreted as such by the clinical microbiologist. As culture was not available in all cases, we also defined a second group wherein all patients with clinical symptoms were considered to have a SSI.
The distribution of baseline characteristics in groups with and without SSI was summarized by absolute numbers and percentages for categorical variables and by mean values with standard deviations or median with range for continuous variables. Univariate and multivariate logistic regression analyses were performed and odds ratios (OR) with 95% confidence intervals (CI) were used to quantify the association between potential risk factors and risk of SSI. The multivariate model included all potential risk factors as covariates, in order to evaluate the independent effect of single risk factors. In some patients multiple procedures were performed. Observations in these patients are likely to be correlated. Robust standard errors were calculated, because ignoring this correlation can lead to misleadingly small estimates of the standard error and consequently too small 95% CI. Multiple imputation was used for dealing with missing values for risk factors. p-values ≤ 0.05 were considered to indicate statistical significance. Analyses were performed using IBM SPSS Statistics version 23.0.0.2 and Stata version 13.
From 1 April 2014 to 1 April 2015, a total of 2,058 surgical procedures were performed in 1,459 patients. Twenty-seven procedures (20 patients) were excluded because antibiotic prophylaxis was required for prosthetic valves or joints as these patients received surgery in locations where the mucosal membrane could potentially be breached. Twenty-one procedures (16 patients) were excluded because the patient received antibiotics in the peri-operative period unrelated to the procedure. Thirty-three procedures (16 patients) were excluded because the occurrence of a SSI could not be verified. These were patients who had not visited their dermatologist or general practitioner after the procedures and could not be contacted.
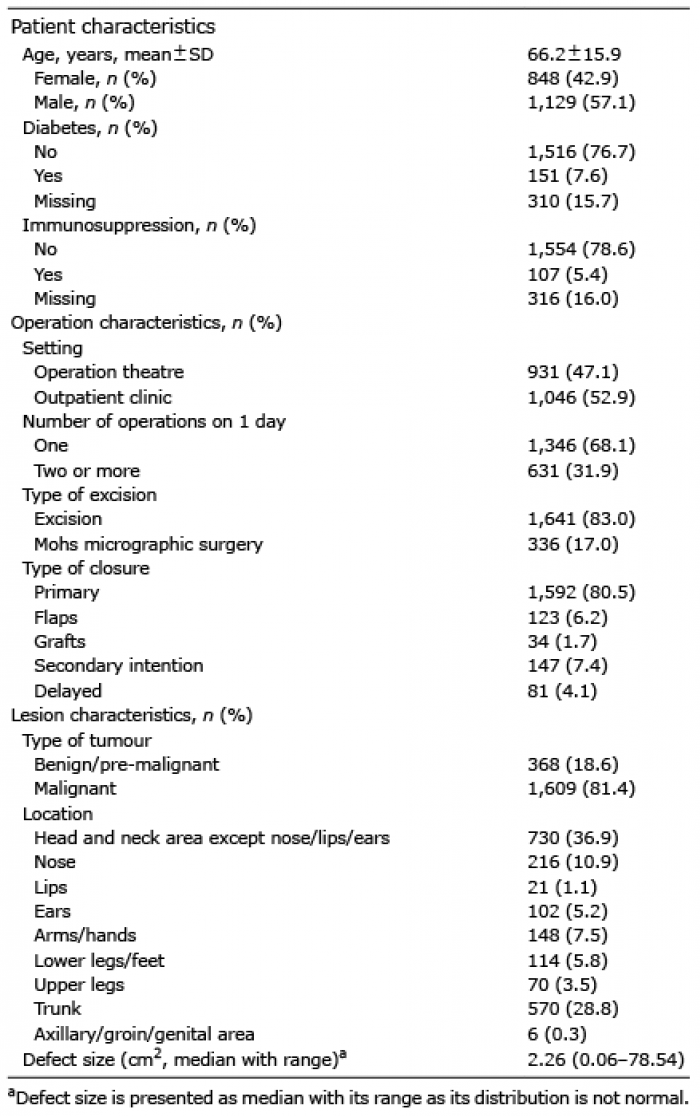
The final study population consisted of 1,977 procedures in 1,407 patients. Baseline characteristics are shown in Table I. Of the 81 procedures with delayed closure, 3 were closed primarily, 40 received grafts and 38 received a flap. Seventy-nine cases (4.0%) presented with clinical symptoms suspicious for a SSI and were treated as such. Wound cultures were obtained in 41 of 79 cases with clinical suspicion and were found positive in 38 (2.0%) (Fig. 1). In 50 of 79 cases, oral antibiotics were prescribed. Of all patients treated with oral antibiotics, 4 experienced gastrointestinal side-effects. No other side-effects were recorded. No re-operation occurred due to impaired wound healing. Of the 5 patients who developed a SSI after delayed closure, 2 developed it before the closure and 3 after closure. Post-operative haemorrhage occurred in 58 procedures (2.9%). Wound dehiscence occurred in 45 procedures (2.3%). Both complications occurred more frequently in the group of patients with SSI.
Table I. Baseline characteristics (n = 1,407 patients; n = 1,977 procedures)
Fig. 1. Clinical presentation of surgical site infections with culture results. MRSA: methicillin-resistant Staphylococcus aureus (SA).
In the primary analysis, the 38 patients with clinically suspected SSI and a positive culture were considered as having SSI. These patients were compared with 1,898 cases without any clinical suspicion of SSI. However, not all patients with clinically suspected SSI had a wound culture, and therefore we performed secondary analysis, in which we considered all 79 patients with clinical suspicion as having SSI. Table II presents the numbers and percentage of procedures with the 2 definitions of SSI, according to the presence of potential risk factors.
Table II. Numbers and percentages with surgical site infections (SSI) according to the presence or absence of potential risk factors
The results of multivariate logistic regression analyses are shown in Table III. When using the strictest definition of SSI (clinical symptoms with confirmation by culture) location on the ears (OR 6.03 95% CI 2.12–17.15), larger defects (OR 1.08 95% CI 1.03–1.14 per unit (cm2) closure by flaps (OR 6.35 95% CI 1.33–30.28) and healing by secondary intention (OR 3.01 95% CI 1.11–8.13) were identified as significant risk factors. In the secondary analyses, considering all 79 patients with clinical suspicion as having SSI regardless of culture results, the same risk factors were associated with significantly increased risk apart from flap reconstruction, but the associations were less strong. In this analysis, procedures performed in the axillary, groins and genital area were also associated with a higher risk of clinical SSI (OR 9.49, 95% CI 0.85–106.55). However, only 6 procedures were performed at these sites and the OR did not reach statistical significance.
Table III. Odds ratios (OR) from multivariate logistic regression analyses
The current study comprehensively evaluated the independent effect of patient, surgery and lesion-related factors on the risk of SSI. The results indicate that the risk of SSI is significantly increased in procedures performed on the ears, in larger defects and in surgical wounds closed by flaps or secondary intention.
The increased risk of SSI in procedures performed on the ear was first suggested by Futoryan & Grande in 1995 (8). Other studies examined the risk of wedge excision, including those on the ear and the lips, and showed conflicting results (6, 10). No multivariate analysis was performed in those 2 studies and therefore the independent effect of location could not be evaluated. In our study, accounting for other potential risk factors by multivariate regression analysis, location of the lesion on the ear was identified as a significant independent risk factor for SSI.
The method of closure as a risk factor for SSI has been studied previously (3, 6, 7, 10). However, no consensus has been reached. These studies did not adjust for other risk factors that can be correlated with the method of closure, such as the location of the tumour and the defect size. In the present study, the independent effect of the closure method was estimated using multivariate regression analysis and the risk of SSI was found to be significantly increased in wounds closed with flaps. A seemingly contra-intuitive finding is that healing by secondary intention was associated with a significantly higher risk of SSI. This specific risk factor has not previously been identified in literature. It is possible that an open wound is more susceptible for an infection occurring after the procedure. This is, however, only a hypothesis, as the mean time to the onset of SSI in this subgroup did not differ from the other closure methods. Further research is needed to confirm and clarify this finding.
One limitation of the current study is the low prevalence of some risk factors, which limited the power to detect small, but relevant, increase in risk for SSI with statistical significance. Secondly, the conclusions of this study are based on a single-centre experience. Extrapolating the results to other centres should be done with care. Thirdly, the results of wound cultures were not available for some patients who had clinical suspicion of SSI. For this reason, separate analyses were performed using 2 different definitions of SSI. The strongest associations were observed when using the strictest definition of SSI: clinically diagnosed infection verified by a positive culture. The weaker associations found in the secondary analysis using a less strict definition of SSI could be the result of misclassification of SSI. Such misclassification of outcome is known to bias odds ratios towards finding no effect. Finally, the authors are aware that not all potential risk factors were studied. For example, we did not routinely report the skin condition, such as ulceration prior to operation, and whether a patient was a present smoker, and therefore these risk factors could not be evaluated. The effect of these potential risk factors should be examined in a multivariate model, together with the risk factors found in the current study.
The clinical question remains: when is antibiotic prophylaxis justified in dermatological surgery? It is generally accepted that antibiotic prophylaxis is not routinely indicated in clean wounds where the risk of infection is below 5% (13, 14). Taking into account the mean low incidence of SSI, it is debatable whether an increase in risk of SSI in patients with a single risk factor requires antibiotic prophylaxis, bearing in mind the potential side-effects of prophylaxis. Therefore, it would be interesting to develop a model to predict the probability of SSI based on combinations of several risk factors in patients undergoing dermatological surgery. Such predicted probabilities could then be used to guide clinical decision-making.
In conclusion, this multivariate analysis of 1,977 invasive surgical procedures in dermatology suggests that procedures performed on the ears, those with larger defects and wounds healed by flaps or secondary intention have an increased risk of SSI.


 Click to show fullsize
Click to show fullsize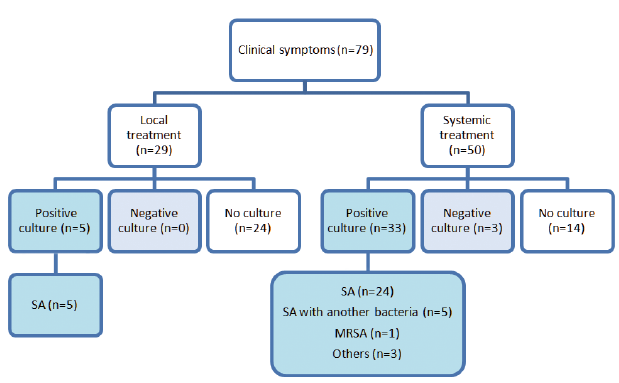 Click to show fullsize
Click to show fullsize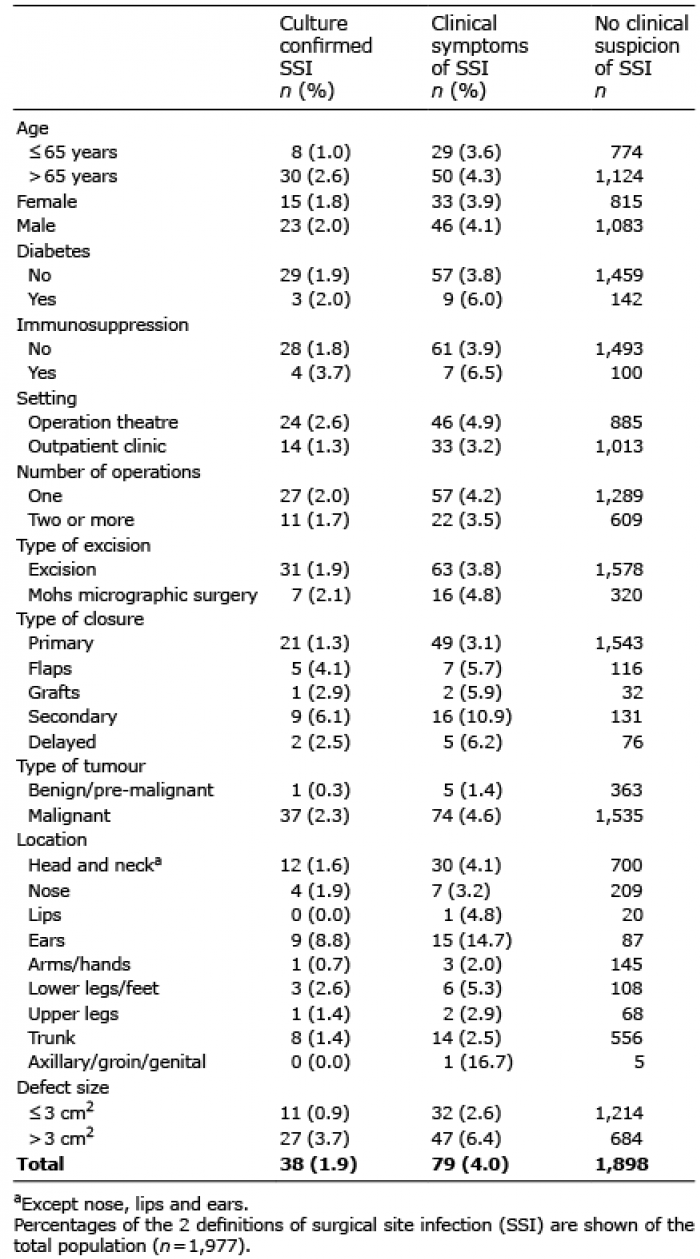 Click to show fullsize
Click to show fullsize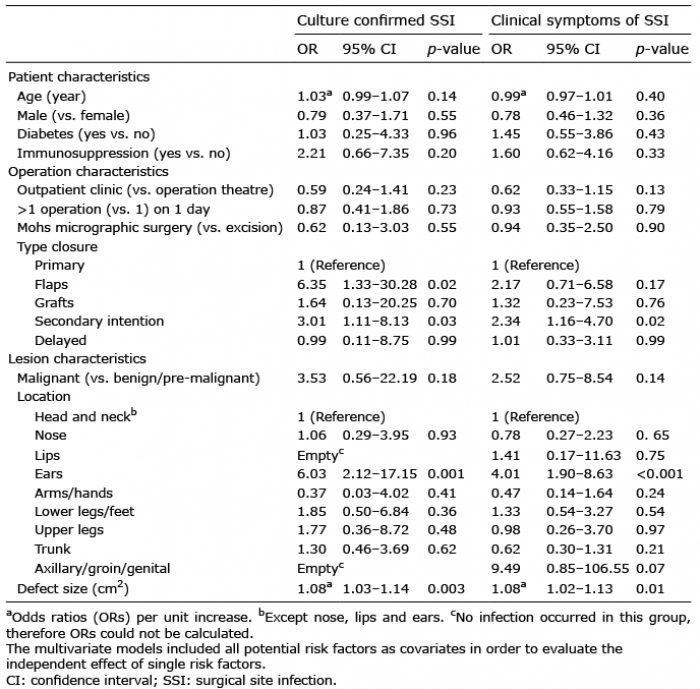 Click to show fullsize
Click to show fullsize