


1Department of Dermatology and 3Laboratory Medicine, University Hospital of Geneva, 1205 Geneva, Switzerland, and 2Department of Dermatology, University of Lübeck, Lübeck, Germany. E-mail: sebastien.menzinger@hcuge.ch
Accepted Nov 13, 2017; Epub ahead of print Nov 13, 2017
Bullous pemphigoid (BP) is an autoimmune blistering disease, with auto-antibodies (autoAb) that target 2 components of the hemidesmosome: BP180, thought to be the major antigen, and BP230. The majority of IgG autoAb in patients with BP react with the 16th non-collagenous (NC16A) domain of BP180 (1).
In patients with BP, IgE is frequently elevated and specific IgE autoAb, reacting with BP180, and BP230 have been described (2). Several studies have reported variable, but usually high, frequencies of IgE anti-BP180 NC16A domain and IgE anti-BP230 antibodies in the serum of patients with BP and a possible correlation between IgE anti-BP180 levels and disease activity (3–6).
The pathogenicity of IgE autoAb in BP remains elusive. It is likely that IgE binding to Fc-epsilon receptors (FcεR) on mast cells or eosinophils leads to inflammation and pruritus, causing the urticarial prodromal phase often seen in BP (7, 8). However, 2 studies showed no correlation between an urticarial/erythematous phenotype of BP and high levels of serum IgE autoAb (3, 4). In vitro, IgE autoAb act in a FcR-independent manner through direct binding to keratinocyte antigens, which trigger interleukin (IL)-6 and IL-8 release by keratinocytes and a decrease in hemidesmosomes (9). This may ultimately contribute to the weakening of the adhesive strength at the dermal–epidermal junction (DEJ) seen in BP.
We report here a case of severe BP in a patient having both IgE and IgG anti-BP180 and BP230 autoAb, which was treated successfully with omalizumab, a humanized monoclonal antibody that binds to the receptor-binding portion of IgE.
A 76-year-old woman with multiple comorbidities (dementia, chronic renal failure, ischaemic cardiopathy, gastro-duodenal ulcer, osteoporosis) presented with an intense pruritic disease that had been present for several weeks, with diffuse eczematous patches, excoriations, crusts and tense blisters (Fig. 1).
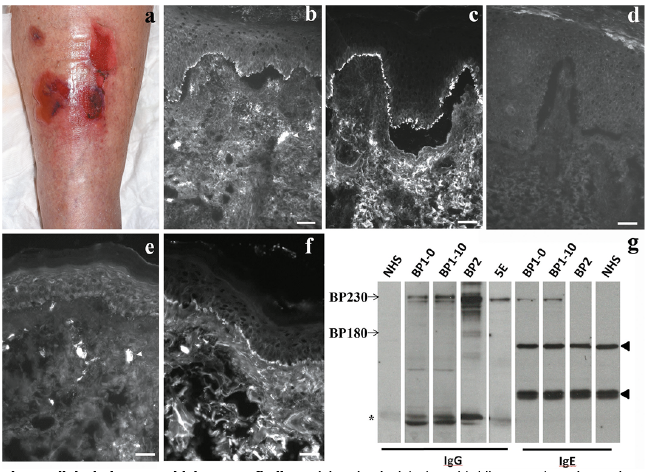
Fig. 1. Clinical picture and laboratory findings. (a) Patient’s right leg with blisters and erosions. Direct immunofluorescent microscopy of the patient’ skin (perilesional skin) at disease onset, demonstrating (b) linear IgE and (c) IgG deposition at the dermal–epidermal junction (DEJ). (d) Negative control. Ten months after disease onset, (f) IgG, but not (e) IgE, was still found at the DEJ. Highly anti-IgE stained cells, presumably mast cells, in the dermis (b, e) arrowhead. (Scale bar 20 µm). (g) Characterization of IgG and IgE autoAb by immunoblotting analysis of normal human keratinocytes extract. In our patient’s sera (BP1), IgG reactivity was found, at 0 and 10 months with a high molecular mass antigen similar to BP230 (5E) and to BP control serum reactive to BP230 in enzyme-linked immunoassay (ELISA) (BP2). Patient’s sera, but not BP2, also contain IgE autoAb recognizing a 230 kDa antigen. No IgG or IgE reactivity was found at 180 kDa. No specific reactivity was found in the serum from a healthy donor normal human serum (NHS), arrowheads denote unspecific reactivity found in all sera. *Probable reactivity with BP230 proteolytic products.
Blood tests revealed elevated eosinophil count and high levels of total IgE (Table I). A lesional skin biopsy showed spongiosis and subepidermal blister with accumulation of eosinophils in the blister cavity and the underlying dermis. Direct immunofluorescence (DIF) micro-scopy disclosed linear deposits of IgG, IgE, and C3 at the DEJ (Fig. 1). Circulating IgG and IgE reacting with the epidermal side of 1M NaCl split normal human skin were detected by indirect IF microscopy. High serum levels of anti-BP180 NC16A IgG and IgE, and anti-BP230 IgG were found by enzyme-linked immunoassay (ELISA) (Table I). By immunoblotting with extract of cultured normal human keratinocyte, IgG and IgE antibodies reacted exclusively with BP230 (Fig. 1). These findings suggested that IgE autoAb targeting DEJ antigens were implicated in this case. Therefore, as our patient had multiple comorbidities and since the disease was not controlled by whole-body application of topical class IV (highly potent) corticosteroids, treatment with omalizumab was started (300 mg subcutaneously (s.c.) monthly). Topical corticosteroids were continued during the first month of treatment, then tapered off and stopped after 2 months of treatment. A dramatic improvement in the pruritus occurred within 2 days, as well as excellent control of the disease with healing of all skin lesions after 8 weeks without adverse events. An increase in total IgE and anti-BP180 IgE was observed, with a reduction in eosinophil count and a decrease in anti-BP180 IgG titres (Table I). After 7 months, the follow-up was lost for 2 months and a relapse occurred. A new DIF in involved skin revealed only linear IgG and C3 depositions, but no IgE (Fig. 1). Serum anti-BP180 IgE and anti-BP230 IgE autoAb were still detectable; however, anti-BP180 IgE level was reduced (Table I). Omalizumab monotherapy was resumed with a good disease control after 8 weeks.
Table I. Summary of the patient’s biological findings during the course of the disease
Treatment of BP with omalizumab in case of contraindications or resistance to usual therapies has been reported previously (10–14). All reported patients had elevated IgE and eosinophil count, as our patient. Here, the implication of IgE targeting BP antigens in the course of the disease was supported by the biological findings: IgE deposition was found together with a linear deposit of IgG and C3 at the DEJ in patient’s skin. Using DIF we also observed IgE-positive cells in the dermis with a morphology suggestive for mast cells. We also hypothesize that some IgE-positive cells were eosinophils. Indeed, Messingham et al. established that eosinophils express FcεRI in the skin (7), and Ishiura et al. (6) showed that IgE anti-BP230 can correlate with local eosinophil accumulation in BP. Using a combination of ELISA and immunoblot we demonstrated that our patient had circulating IgE autoAb targeting both BP180 and BP230. The discrepancy between ELISA and immunoblots for BP180 autoAb could be explained by poor sensitivity of immunoblot compared with anti-BP180 ELISA. Alternatively, IgE anti-BP180 may target conformational epitopes that were not conserved in immunoblot.
In the case described here, the disease was controlled with omalizumab monotherapy. After 2 months of therapy, total IgE and anti-BP180 IgE levels increased in the patient’s serum, probably because IgE/omalizumab complexes have an increased half-life (15). More surprisingly, a reduction in anti-BP180 and, to a lesser extent, anti-BP230 IgG levels, was observed after 7 months of therapy. When the treatment was involuntarily discontinued, a clinical and biological relapse was observed, with an increase in levels of IgG autoAb and peripheral blood eosinophil count, but a decrease in IgE anti-BP180 levels. Moreover, at relapse, IgE were no longer detectable at the DEJ by DIF, but the resumption of omalizumab was effective. This observation supports the multiple implications of IgE autoAb in BP, through FcR-independent or -dependent effects. Overall, our findings strongly suggest that IgE is critically implicated in the activity of the disease in patients with BP with IgE autoAb.
Thus, omalizumab should be considered as a therapeutic alternative to immunosuppressive regimen, especially in patients with comorbidities and anti-BP180 IgE reactivity. Larger trials are needed to better define the indication for omalizumab in BP and to determine the importance of measuring IgE anti-BP antigens in the management of BP.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize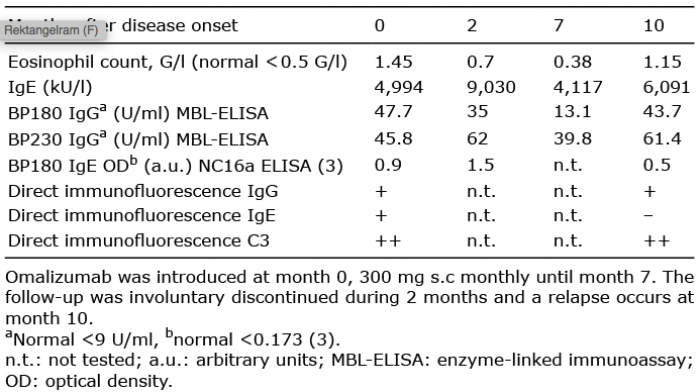 Click to show fullsize
Click to show fullsize