


Department of Dermatology, University Hospital, Jena, Germany
Scleroedema adultorum Buschke is a rare skin disease, which can be divided into 3 subtypes: classic type, occurring after respiratory infections; a type lacking association with infections; and a type associated with diabetes. Scleroedema adultorum Buschke is characterized by thickening and tightening of the skin, which typically starts at the neck. In half of patients, spontaneous remission may occur. The aim of this systematic review is to summarize all reported treatments for scleroedema adultorum Buschke, based on articles from PubMed database, using the query “scleroedema adultorum Buschke treatment”, English and German, published between 1970 and 2016 and documenting adequate treatments. The results are based mainly on individual case reports, small case series, and retrospective studies often reporting unsuccessful results. Treatment options include topical as well as systemic treatments, and physical modalities. There is a need for randomized controlled trials and studies on long-term outcomes after treatment.
Key words: scleroedema adultorum Buschke; treatment.
Accepted Nov 13, 2017; Epub ahead of print Nov 14, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Diana Miguel, Department of Dermatology, University Hospital, Erfurter Straße 35, DE-07740 Jena, Germany. E-mail: Diana.Miguel@med.uni-jena.de
Scleroedema adultorum Buschke (SAB) is a rare skin condition of unknown aetiology that was first described by Curzio in 1752. However, its name is associated with Abraham Buschke who reported a 46-year-old patient developing skin hardening after an episode of influenza in 1902. The nomenclature has been criticized, since the disease also occurs in younger individuals lacking sclerosis. In fact, in 209 patients with SAB, 51% were younger than 20 years old. For childhood cases, SAB must be differentiated from scleroedema neonatorum (1–4).
SAB is characterized by skin thickening and tightening that typically starts at the neck and spreads over the upper part of the body, e.g. the face, scalp, shoulder, and trunk (Fig. 1). The hands and feet are usually not affected (5, 6). A case of SAB confined to the thighs has also been reported (7).
Fig. 1. Scleroedema adultorum Buschke with extensive severe skin thickening and solid oedema of the neck, back, shoulders and upper arms.
SAB can be divided into 3 types:
There are no specific laboratory abnormalities, but the diagnostic workup of SAB should include analysis of anti-streptolysin O titre, haemoglobin A1c, sedimentation rate, blood count, and protein electrophoresis. There is no racial or ethnic propensity, but women are usually more affected with type 1 and type 2 SAB than are men (1). Scleroedema has also been associated with internal malignancies, e.g. insulinoma and carcinoma of the gall bladder (11, 12).
Histologically, SAB is characterized by a normal epidermis with an up to 4 times thickened dermis containing mucopolysaccharides, as evidenced by Alcian blue stain, in oedematous spaces between collagen fibres. The subcutaneous fat tissue is usually replaced by coarse collagen fibres (13).
The course of scleroderma is usually slow and rarely fatal. Patient’s complaints include tightness, thickening, and hardening of the skin, which typically occurs on the face, neck, chest, proximal arms, and back. Patients usually have limitation in range of motion in the torso, shoulders and neck. Some patients describe erythematous discoloration of the affected areas. A few patients may describe a decreased oral aperture and dysphagia. In approximately 50% of cases, there is spontaneous resolution within less than 18 months. However, the other half are mostly resistant to treatment. SAB may also affect the heart, bones, joints, liver, spleen, eyes, bone marrow, salivary glands, nerve tissue, and tongue (1, 13–21). Differential diagnosis of SAB should include systemic sclerosis, scleromyxoedema, and eosinophilic fasciitis (10). In a retrospective study of 21 patients with diabetes, Rho et al. (22) reported that scleroedema might improve if hyperglycaemia is controlled.
Concerning the treatment of SAB, several options have been tried, including immunosuppressive agents, antibiotics, physiotherapy, thyroid hormones, and systemic glucocorticoids, but no effective treatment has yet been established (1).
To our knowledge this is the first systematic review of the treatment of SAB. We hereby summarize all previously reported treatment options, in order to help physicians make the choice of adequate treatment according to each patient’s SAB type.
A systematic review, based on PubMed, using the query “scleredema adultorum Buschke treatment” was performed. Our search was limited to English and German language, to human data and to papers published from 1 January 1970 to 31 December 2016, documenting adequate treatment for SAB. We reviewed the reference lists of full-length articles in order to identify additional articles that met the pre-defined inclusion criteria. A total of 34 articles was identified from the initial search in PubMed and an additional 21 articles were found through manual review. After reviewing all full-text articles and excluding reviews and papers about other diseases and articles without reporting on treatment, a total of 34 studies, 23 from the initial search and 11 from additional papers, were analysed (Fig. 2). For each study included, a summary of author, study year, country, study design, number of patients, therapies, follow-up/outcome, and trigger factors is given in Table SI.
Fig. 2. Flow diagram based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
The results of this study are mainly based on individual case reports, small case series, and retrospective studies (see Table SI). Treatment options include topical as well as systemic treatments, and physical modalities. Treatments were often reported to be unsuccessful. The disease course under treatment tends to be different according to each type of SAB. Thus, classification of the subtypes, as described above, appears to be the first useful step.
Topical and intralesional corticosteroids have been used in patients with SAB, with no improvement in the skin lesions in most reported cases, except for one patient with SAB and diabetes whose cutaneous disease progression was reported to have subsisted under topical treatment with triamcinolone cream 0.1% (13).
SAB is caused by an increase in acid mucopolysaccharides, resulting in accumulation of hyaluronic acid. Toyota et al. reported an improvement following hyaluronidase injections. However, they did not reach a conclusion, since the patient was concomitantly receiving vitamin E (23).
A total of 3 patients underwent systemic treatment with methotrexate. Shazzad et al. reported a patient with SAB with no trigger factor, who was successfully treated with methotrexate and psoralen plus ultraviolet A (PUVA) (24). Another patient with SAB and insulin-dependent diabetes mellitus had partial improvement under therapy with low-dose methotrexate (25). The third patient, reported by Venencie et al. (26), showed no response to treatment with methotrexate. An unsatisfactory outcome was reported in one patient treated with methotrexate, pentoxyfylline, and colchicine (27).
Treatment with prednisone was reported in 8 cases, and the therapeutic outcomes were variable. No improvement in the skin lesions was seen in 5 patients. One patient showed a partial response, but was also treated with UVA1 and penicillin (28). In 2 patients, systemic steroids resulted in a mild improvement.
Since SAB is often associated with diabetes mellitus, systemic corticosteroids may be contraindicated.
Intravenous immunoglobulin (IVIG) has diverse immunoregulatory effects decreasing the activation of autoreactive T cells. Aichelburg et al. (29) reported a patient with SAB associated with a post-streptococcal infection that was treated successfully with IVIG. It should be kept in mind, however, that post-streptococcal SAB tends to spontaneous regression.
Antibiotics are among the treatments of choice for SAB, with penicillin being the favourite.
Symptoms improved in a patient treated with high-dose antibiotics, and in 2 patients receiving penicillin. In one individual, in whom the lesions appeared to be associated with tonsillitis, penicillin led to complete regression. However, another patient did not show any improvement under treatment with penicillin (28, 30–33).
When penicillin allergy is suspected, eventual treatment with this drug should not be precluded. Wessbecher & Stangl (34) suggested a new scheme of tolerance induction after allergy testing is carried out. Allergy testing should include serological examination of specific IgE antibodies against β-lactams, followed by a skin-prick test and intradermal and epicutaneous testing. In fact, they describe a patient with SAB and hypersensitivity to penicillin in whom this drug was carefully administrated. This patient underwent clinical improvement with no complications or side-effects. The exact mechanism of action is not fully understood, but it may be due to the anti-fibrotic effect of penicillin, induced by the inhibition of prolyl hydroxylase activity (31).
Coagulation factor XIII is a plasma transglutaminase, and the final enzyme in the coagulation cascade. In 2004, Venturi et al. (35) published a single case of a patient whose disease remitted after intravenous treatment with factor XIII (FXIII). Factor XIII has been known to be effective in scleroderma, a disease that shares similarities with SAB, and is known for targeting anti-fibrinolytic proteins that act on vascular endothelial growth factor receptor VEGFR-2 and αvβ3 integrin, promoting angiogenesis and neovascularization, and for inducing cross-linking of the provisional matrix.
In case reports of 2 patients, therapy with cyclosporine resulted in complete resolution of SAB associated with pharyngitis and otitis (36). Again, we should consider that spontaneous regression may have been possible.
Other systemic therapies, such as pentoxyfylline, colchicine, interferon-γ, and D-penicillamine, have been tried and were almost always reported to be unsuccessful. Patients with type 2 SAB, associated with paraproteinaemia, were also treated with cyclophosphamide, chlorambucil, dapsone, melphalan, and/or adriamycin, with poor results. One patient with multiple myeloma experienced an improvement in symptoms, with the skin becoming more elastic, after receiving pulse therapy with cyclophosphamide and prednisolone (37).
Phototherapy consists of the use of speci?c wavelengths of ultraviolet (UV) radiation in a therapeutic setting, in which physicians can decide whether to use UVA (320–400 nm), UVB (290–320 nm) or both (38). Currently, phototherapy, namely long-wave UV, such as UVA, is widely used in the treatment of localized scleroderma (morphea), but the exact mechanism of how it reduces the symptoms of scleroderma is unclear.
Reports were found on a total of 8 patients who underwent phototherapy. Two patients were treated successfully with UVB radiation. Another patient did not respond to UVB treatment but showed a marked improvement after psoralen and ultraviolet A (PUVA)-bath therapy (33, 39, 40). The best results were seen after PUVA therapy, with 3 patients showing marked improvement in symptoms (24, 33). Two patients with recalcitrant SAB, one associated with diabetes mellitus, and another with IgA myeloma, showed no progress after phototherapy (15, 41). A single patient treated with a combination of penicillin, prednisolone, and 30 sessions of UVA1 reported a reduction in skin thickness and an increase in mobility (28).
ECP consists of the exposure of 10–20% of the body’s leukocytes to photoactivated 8-methoxypsoralen and their re-infusion to the patient. The exact mechanism of ECP is not known. It seems that the immune system exposure to physically modified T cell-clones may lead to a specific inhibition of T cell-mediated autoimmunity in diseases where T cells play a major role. A report by Stables et al. (42) showed regression of the skin lesions in a patient with SAB and paraproteinaemia after 6 months of ECP treatment.
The effects of ionizing radiation on SAB are unclear. It has been suggested that electron-beam radiation might induce apoptosis of abnormal dermal fibroblasts and may inhibit their proliferation by conditioning collagen and mucin production (43, 44). We found a total of 9 patients treated with radiotherapy. The first case was reported in 1994 by Angeli-Besson et al. (8). A patient with SAB associated with IgA kappa monoclonal hypergammaglobulinaemia showed a significant improvement in skin lesions after treatment with electron-beam radiation. Another 10 patients, the majority with SAB associated with diabetes mellitus, had positive results under radiotherapy (9, 43–47). However, 1 individual with SAB and monoclonal gammopathy showed no improvement after treatments with cyclophosphamide, plasma exchange, and electron beam radiation (20).
SAB is a rare skin disease characterized by skin thickening and tightening typically at the neck and the upper part of the body. The clinical response of SAB is inherently difficult to classify because of the paucity of objective measures, e.g. angle of arm abduction and self-reporting of symptoms by the patient. In our systematic review the “results” are mainly based on the individual report of each author, which makes comparisons difficult and limits the reliability of the findings. Therapy for SAB was often reported to be unsuccessful, and this may be the reason for the few cases published in the literature (publication bias). Due to the rarity of SAB, randomized controlled trials are difficult, and no first-line therapy has been suggested. Different treatment options have been considered, but most of them are unreliable. Due to the known positive effects of manual therapy, regardless of the possible mechanisms of its pathogenesis, connective tissue massages should be prescribed (41).
Patients with type 1 SAB associated with an underlying infection responded well to treatments with penicillin, UVB, and IVIG. All of these therapies were given in just a few patients, thus we cannot establish them as a standard treatment.
Paraproteinaemias occurring in association with SAB are usually therapy-resistant, and the malignant condition must be prioritized. Electron-beam therapy and ECP may be good options. Diabetic scleroderma is the most frequent and, based on our results, we would suggest phototherapy (especially PUVA) or electron-beam therapy as the treatment of choice.
In all types of scleroderma, combination therapy may be tried. Adjuvant therapy with penicillin or local therapy with corticosteroids may be worthwhile.
However, a final treatment decision should be made individually, taking into consideration the concomitant diseases of the patient, SAB extent (size and localization), and possible trigger factors. Patients should be advised that a great part of the treatment modalities are off-label use and that they may fail to fulfil the patient’s hopes and expectations. Finally, physicians should be aware that their therapeutic advice is based on the few case reports and case series already published. Clearly, new therapeutic ideas, based on a better understanding of the pathogenesis of SAB, are needed in order to manage this enigmatic and problematic disease.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize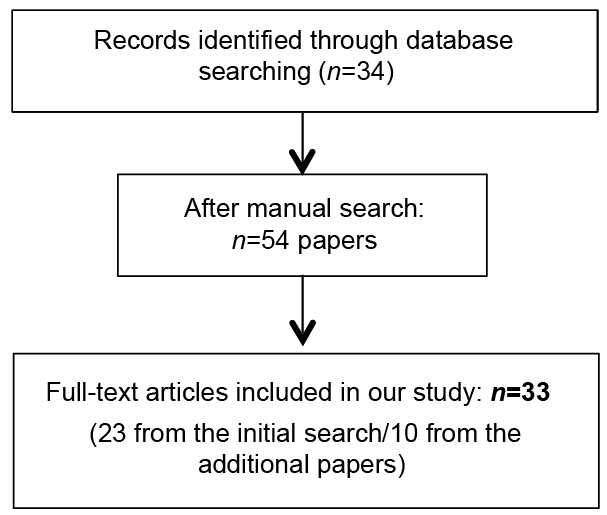 Click to show fullsize
Click to show fullsize