


1CIC, Inserm U1232, 2Department of Dermatology, 3Bacteriology and Hygiene Unit, Biology Institute, 4Biostatistic Department, PIMES, Saint-Jacques Hospital, Nantes University Hospital, Nantes, and 5Evaluation Department – CUTIS – Galderma R&D, Biot, France
Propionibacterium acnes, a major member of normal skin microbiota, is subdivided into 6 phylotypes: IA1, IA2, IB, IC, II and III. This study investigated P. acnes subgroups on the face and back in patients with severe acne and in healthy controls. In 71.4% of patients with severe acne, P. acnes phylotypes were identical on the face and back, whereas this was the case in only 45.5% of healthy controls. The healthy group carried phylotypes IA1 (39.1%) and II (43.4%), whereas the acne group carried a high predominance of IA1 (84.4%), especially on the back (95.6%). In addition, the single-locus sequence typing (SLST) method revealed A1 to be the predominant type on the back of patients with acne, compared with a wide diversity in the healthy group. We report here that severity of acne on the back is associated with loss of diversity of P. acnes phylotype, with a major predominance of phylotype IA1. The change in balance of cutaneous P. acnes subgroups might be an inducing factor in the activation of P. acnes, which could trigger inflammation.
Key words: acne; P. acnes phylotypes; clonal complexes; SLST-types.
Accepted Nov 13, 2017; Epub ahead of print Nov 14, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Brigitte Dréno, Department of Dermatology, Nantes University Hospital, 1 Place Alexis Ricordeau, FR-44035 Nantes Cedex 01, France. E-mail: brigitte.dreno@wanadoo.fr
Acne is one of the most common skin diseases worldwide, affecting up to 85% of the population (1). At the pathophysiological level, 2 factors play a crucial role: the sebaceous gland and Propionibacterium acnes. P. acnes is a commensal anaerobic Gram-positive bacterium of the healthy skin. This bacterial genus has high specificity, from face to feet areas (2). This study showed a predominance of Propionibacterium genus on the face and back. This microorganism diversity on the human body also depends on several factors, such as host factors (e.g. age, sex, hair follicle density) and environmental factors (e.g. occupation, clothing choice, antibiotic use) (3, 4).
P. acnes plays an important role in the maintenance of normal cutaneous microbiota, by inhibiting the development of some pathogenic bacteria, such as Staphylococcus aureus and Streptococcus pyogenes. It produces propionic acid and, thus, can maintain acidic pH in the pilo-sebaceous follicles. In addition to acne, P. acnes has also been implicated in deep infections and orthopaedic abscesses (5–7), lung abscesses (8), prostate cancer (9), and sarcoidosis (10). Its development in deep infections may be related to the secretion of a biofilm that increases both its adherence to surfaces and antibiotic resistance (11).
In the skin, P. acnes, as an anaerobic bacterium, is located more specifically in the pilo-sebaceous follicles. A number of studies have shown that P. acnes can activate innate immunity, mainly via Toll-like receptors (TLRs) expressed by keratinocytes and monocytes (12, 13). P. acnes also stimulates the secretion of interleukins (IL)-12, IL-8, IL-1β and IL-17 cytokines by monocytes (14). Thus, it plays a crucial role in the development of inflammatory lesions in acne.
P. acnes population strains are divided into 6 main phylotypes: IA1, IA2, IB, IC, II and III. Recent genomic studies have also highlighted the presence of subgroups among phylotypes, according to genome analysis called multi-locus sequence typing (MLST) (15) and single-locus sequence typing (SLST). These cluster differentiations are called clonal complexes (CCs). Some P. acnes phylotypes are associated with skin disease conditions, such as phylotype III and progressive macular hypomelanosis (16). Moreover, different P. acnes phylotypes are known to induce distinct immune responses in the context of acne (12, 17). The aim of this study was to determine and compare the different P. acnes phylotypes, CCs and SLST types on the face and back of patients with severe acne of the back vs. a healthy population.
At the first visit, patients with acne who fulfilled the inclusion criteria were selected. The inclusion criteria were: age (16–35 years), at least 2 nodules on the back, complying with wash-out periods for acne drugs including systemic antibiotics (1 month), oral retinoids (6 months) and topical treatments (2 weeks). Healthy volunteers were selected according to inclusion criteria, including the total absence of acne on the face and back, and the absence of other history or current dermatological pathologies. All patients provided signed informed consent and the study was approved by the health authorities (Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM); number 151141B-42) and ethics committee (Comité de Protection des Personnes (CPP); number 21–15).
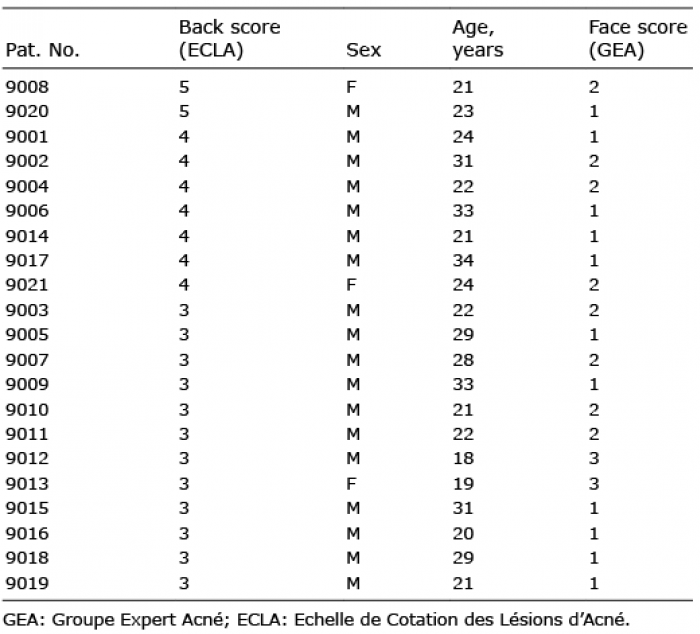
For each patient with acne, face and back acne scores were established by a dermatologist. These scores were estimated from 0 to 5 according to the type of acne (mild to severe), for both areas. All scores are shown in Table I. Scores for back acne were established according to the Echelle de Cotation des Lésions d’Acné (ECLA) scale (18). Scores for face acne were established according to the Groupe Expert Acné (GEA) scale (19). The experimental scheme of the study is detailed in Fig. 1.
Table I. Clinical data for acne patients
Fig. 1. Experimental scheme of the study and summary of the main results obtained. CC: clonal complex; SLST: single-locus sequence typing.
For all included patients, swab samples were taken from the face and the back at the same visit, from a surface area of 1 cm2 surrounding an inflammatory lesion (papule), by rubbing with the swab for 45 s. Samples were collected in both groups from the back and face zones, using a cotton swab, and separately discharged into a brain heart infusion medium and delivered to the Bacteriology Department of Nantes University Hospital within 30 min. Each sample was cultured anaerobically at 37°C for 7–10 days. Colonies with the macroscopic morphology of P. acnes were picked from each plate to recover the predominant strain of P. acnes. As reported recently (20), this picking method allows the predominant clone of P. acnes present in the cutaneous skin flora to be recovered. Indeed, it has been shown that the representative isolate constitutes 85–100% of the sample.
All isolates were identified by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry with a VitekMS® mass spectrometer (MALDI-TOF MS) (bioMérieux SA, Marcy-l’Etoile, France). All strains were identified accurately with a value > 99.9%.
Total DNA from P. acnes isolates was extracted using the InstaGene Matrix method (Bio-Rad Laboratories, Hercules, CA, USA) according to the manufacturer’s instructions.
The 6 main phylotypes for all isolates were determined as described previously (21).
MLST is a method to determine to which clonal complex a P. acnes strain belongs. Recently, 2 main MLST schemes have been developed (22, 23), but we decided to use the method developed by Lomholt & Kilian (23) according to its best discriminant power. This scheme is based on partial sequencing of 9 housekeeping genes, comprising a total of 4,287 nucleotides, and is available at http://pacnes.mlst.net/.
SLST is a molecular typing method based on the analysis of a single locus of the P. acnes genome. The portion of amplified DNA enables the identification of P. acnes SLST-types (A1, A5 etc.). SLST was carried out on all isolates, as described previously (24). Reference sequences for alignment and trimming are described in the web-interface typing tool at http://medbac.dk/slst/pacnes
Sequencing was performed on a 3130xl-1 Hitachi (Applied Biosystems, Foster City, USA). At the end of the sequencing, each sequence for each sample was reviewed and analysed using Seqscape software v2.5 (Applied Biosystems) before comparison with online databases.
Statistical analyses were performed using Fisher exact test (R software (R Foundation for Statistical Computing, Vienna, Austria)).
A total of 24 patients with acne and 12 healthy volunteers were recruited. For each patient with acne, GEA and ECLA scores were established by a dermatologist for the face and the back, respectively. Concerning the back zone, 15 of the 24 patients scored 3, 7 scored 4, and 2 scored 5. In addition, concerning the face zone, 14 scored 1, 8 scored 2 and 2 scored 3. The clinical data are shown in Table I.
Positive culture was obtained for all patients and controls (100%). Cultures identified P. acnes, but also other bacterial species, including S. aureus (acne group 2/48; 4.2% vs. healthy group 2/24; 8.3%), and S. epidermidis (acne group 33/48; 68.8% vs. healthy group 14/24; 58.3%). P. acnes was systematically recovered from all collected samples (n = 72) in culture, except for 4 samples. Instead of P. acnes, other species were discovered, including P. avidum in the healthy group (2/24; 8.3%), P. granulosum in the acne group (1/48; 2.1%) and P. namnetense in the acne group (3/48; 6.3%). However, no significant difference in bacteria diversity was noted on the back between acne and healthy individuals (p = 0.820). In addition, no significant difference in bacteria diversity was noted between the face samples from subjects with acne and healthy subjects (p = 0.690).
The P. acnes phylotypes found both on the back and on the face in acne vs. healthy groups were different.
In healthy group samples (face and back), 5 of the 6 main phylotypes were present, showing a large diversity: IA1, IA2, IB, II and III (Fig. 2). The most predominant ones were phylotypes IA1 and II (respectively, 39.1% and 43.5% of isolates), 8.7% were phylotype IB, 4.3% phylotype III and 4.3% phylotype IA2. On the face, the most predominant phylotypes found were phylotype IA1 (41.6%), and II (33.3%). This trend was the same on the back zone for this group, with a majority of phylotypes IA1 and II (36.3% and 54.5%, respectively).
Fig. 2. Propionibacterium acnes phylotype distribution on 2 sites on healthy volunteers and acne patients (n = 12 and n = 24, respectively). Categories “Healthy” and “Acne” represent the percentages of phylotypes found on the back and the face, respectively.
In acne group samples (face and back), 4 out of the 6 main phylotypes were identified: IA1, IA2, IC, and II (Fig. 2). Phylotype IA1 represented 84.4% of typed P. acnes. The other phylotypes represented only 6.6% for phylotypes II, 2.1% for IC, and 6.6% for IA2 (6.6%) (Fig. 2). No phylotype III was identified. Concerning the back zone, a large predominance of phylotype IA1 was found (95.6%) with a significant association (p < 0.001), phylotype II represented only 4.3% of the P. acnes strains, no other phylotype was detected on this body site. On the face zone, phylotype IA1 was the most predominant phylotype (72.7%), compared with 13.6% for phylotype IA2, 9.1% phylotype II. Moreover, a rare P. acnes phylotype was also found in the acne group on the face: phylotype IC (1/48; 2.1%). For both zones, no significant association was found between acne severity (GEA and/or ECLA scores) and phylotypes (p = 0.649 for the face and p = 0.391 for the back). The main results concerning phylotypes identification are shown in Fig. 1.
In conclusion, there was a higher diversity of P. acnes phylotypes on the face vs. the back zone, in both groups, and phylotype IA1 was largely represented in the acne group, especially in the back zone.
To go deeper in the analysis of P. acnes lineages involved in acne lesions, 2 additional molecular typing methods were performed: MLST and SLST. These additional methods offer more precise data about the phylogenetic clades distribution of P. acnes isolates. SLST-type A1 was predominant in the acne group (Fig. 3). A higher diversity of SLST-types associated with known phylotypes (IA1 and II) with new SLST-types never described before was also noted: K16 (phylotype II) and L7 (phylotype III) in the healthy group; A27, A28 (phylotype IA1), F11 (phylotype IA2), and K17 (phylotype II) in the acne group. Analysis of the distribution of clonal complexes (CC) among both healthy and acne populations in the back/face zones revealed that CC18 and CC53 were more associated with the acne group and the healthy group, respectively (Fig. 4). The main results concerning CC identification are shown in Fig. 1.
Fig. 3. Propionibacterium acnes single-locus sequence typing (SLST) type distribution according to 2 body sites on healthy volunteers and patients with acne (n = 12 and n = 24, respectively). Categories “Healthy” and “Acne” represent the percentages of the different SLST types found on back and on face in either the healthy group or the acne group. “ND” category represents the other species found instead of P. acnes, where typing was not possible.
Fig. 4. Propionibacterium acnes clonal complex (CC) distribution on 2 sites on healthy volunteers and acne patients (n = 12 and n = 24, respectively). Categories “Healthy” and “Acne” represent the percentages of the different CCs found on the back and face in either the healthy or the acne group. “ND” category represents the other species found instead of P. acnes, where the typing was not possible.
In healthy group samples, 41.6% belonged to the CC53 subgroup (phylotype II and K SLST-types), 20.8% of the P. acnes strains belonged to the CC18 subgroup and 16.6% to the CC28 subgroup belonging to phylotype IA1 including SLST-types A1, C1 and D1 (Figs 3 and 4). Taking into account the location (face or back), 50.0% of the back samples were CC53 (phylotype II including K1, K2, and K8 SLST-types), 16.6% were CC28 (phylotype IA1 including D1 SLST-type), 8.3% were CC18 (phylotype IA1 and A1 SLST-type), 8.3% were CC3 (phylotype IA1 and C1 SLST-type) and, finally, 8.3% were CC43 (phylotype III and new SLST-type named “L7”) (Figs 3 and 4). Concerning the face zone, 33.3% of the strains were CC18 (phylotype IA1 and A1 SLST-type) and 33.3% were CC53 (phylotype II including K1 and a new SLST-type named “K16”), whereas 16.6% were CC28 (phylotypes IA1 and IA2 corresponding to D1 and F4 SLST-types) and 16.6% were CC36 (phylotype IB and H1 SLST-types) (Figs 3 and 4).
Interestingly, the only P. acnes phylotype III found in this study was recovered in the healthy group, associated with CC43 and a new SLST-type L7 not previously described.
In acne group samples, 58.3% of the P. acnes strains belonged to CC18 and 16.6% belonged to CC28, including SLST types A1, A5, C1, D1 and E3 (Fig. 3, 4). Taking into account the location, 62.5% of the back samples were CC18, demonstrating a significant association of this CC with back acne skin-condition (p < 0.001). Moreover, 16.6% of the back samples were CC28, corresponding to phylotype IA1 (total absence of phylotype II), whereas 54.1% of the face samples were CC18, 16.6% were CC28, and 8.3% were CC53 (phylotype II corresponding to K SLST-types). In addition, a significant association was found between SLST-type A1 and back acne skin-condition (p = 0.002).
All new SLST-types described for the first time in this study are as listed: A27 (acne back), A28 (acne face), F11 (acne face), K17 (acne back), K16 (healthy face and healthy back), and L7 (healthy back). These new SLST-types have been incremented in the online database, based on Christian F. P. Scholz’s genetic system (http://medbac.dk/slst/pacnes). The main results concerning identification of CC and SLST-types are summarized in Fig. 1.
In summary, this study reveals that inflammatory severe acne of both face and back is associated with diversity loss of P. acnes phylotypes, and a high predominance of phylotype IA1, both on the face (72.7%) and the back (95.6%), which has not been described previously. In healthy individuals, 2 main phylotypes have been found: IA1 (39.1%) and II (43.4%). In addition, this study identifies A1 SLST-type as the predominant SLST-type recovered from nodular acne of the back.
Distribution of phylotypes and CCs on the human body in the context of acne has been studied previously. Lomholt & Kilian analysed the distribution of CCs in 2 patients with acne on the face/back (25), and showed the presence of several CCs, including CC3 and CC18 on face, but a lower diversity of CCs on the back. Moreover, the results of the current study confirm those of Lomholt et al. (20) regarding the predominance of IA1 phylotype (CC18) in patients with acne, but this study did not perform determination of SLST-types. In our study, among the large diversity of SLST-types found, we describe the significant association between A1 SLST-type and severe back acne. Overall, despite a highly conserved genome of P. acnes (26), we show that acne lesions are associated with the development of a specific subpopulation of P. acnes.
From our 72 isolates, the A1 SLST-type was significantly associated with acne skin condition. In addition, we found 6 new SLST-types that had not been described previously (i.e. F11, L7, K16, K17, A28, and A27), which have been incremented in the online database (24) (http://medbac.dk/slst/pacnes). Currently, the impact of the different SLST-types on skin disease is not known; this field represents an interesting avenue for future clinical investigations. To our knowledge, 2 studies currently describe P. acnes SLST-types found in acne vulgaris (27, 28). In Nakase et al., the SLST-type predominantly found in severe acne is A5. In our data, we found the SLST-type A1 as the predominant type in severe acne of the back. This difference can be due to ethnicity, skin care (i.e. use of cleansers, moisturizers, etc.), climate, and acne therapeutic care, which differs from country to country, notably with regard to use of antibiotics, isotretinoin and benzoyl peroxide. Nevertheless, in both cases we found clade A to be predominant in severe acne.
In contrast to SLST-types, association of CCs with some diseases is starting to be well-documented, such as: CC36 and CC53/60 in prostate cancer and absence of CC18 (29), and CC18 association with acne-skin condition (20). Previous works have reported a high diversity of CCs in sarcoidosis: CC36, CC28, CC53, CC18 and singletons (30). In the same manner, our data reveal a diversity of CC, found on both the back and face zones, in the healthy group. For example, phylotype IA1 was associated with CC18, CC28 and CC3. In addition, our study confirms the association between CC18 and acne, and between CC53 and healthy skin.
Our results show a decrease in diversity of P. acnes phylotypes in severe back acne (all patients had a minimum of 2 nodules on the back and 40% of patients were scored 4–5). This loss of diversity could be the result of hyperseborrhoea, which is associated with both qualitative and quantitative sebum modifications inducing alteration of the skin barrier and, subsequently, microbiota changes. Interestingly, it has been shown that there is a direct link between hyperseborrhoea, proliferation of P. acnes and onset of acne lesions (31). As the microbiota modulates the innate immunity of the skin (32, 33), this loss of diversity could activate innate immunity, triggering the development of inflammatory acne lesions.
We also report differences in the pattern of P. acnes phylotypes between the back and face. We hypothesize that these differences might be related to several factors that impact differently on face/back skin bacterial populations, such as cleansers and physical agents (wind, sun, etc.), although this has not been investigated for P. acnes phylotypes (3, 4).
In culture we identified P. namnetense in 3 patients (2 minor acne face score 1; 1 severe acne back score 3), which has not been described previously in acne and could lead to further investigations about the link between this bacterium and specific clinical forms of acne. All patients and controls were positive for P. acnes or related species with our sampling method, which is an important point at the methodological level, compared with previous studies in which culture positivity was found in approximately 70–84% of patient samples (34, 35). Concerning the association between S. epidermidis and P. acnes, we identified S. epidermidis in 50% of acne back samples (41.6% in healthy back), and 75% of acne face samples (75% in healthy face) (data not shown), respectively. Interestingly, these data favour the hypothesis of a symbiotic association between P. acnes and S. epidermidis, as a crucial element for skin microbiota balance (3, 36).
At the bacteriological level this study sheds light on an important question: Do all CCs that belong to a same cluster (i.e. IA1) stimulate innate immunity effectors in the same way? Seeing how different the P. acnes CCs and SLST-types are from one body area to another in both acne/healthy context, the elucidation of this question will permit better understand of the role of certain P. acnes subgroups (i.e. SLST-types and CCs), and determine whether some of them are associated with pro-inflammatory reactions in human skin.
The results of this study suggest that acne could be associated with the proliferation of one specific phylotype. These results can be related to the study from Tax et al. (37), who found a difference in growth properties and propionic acid production between the different P. acnes phylotypes. Taken together, these data provide a potential explanation for the role of the different P. acnes phylotypes in acne physiopathology.
This study opens up new areas of research into innovative alternative treatments for acne. In 2015, Yu et al. reviewed P. acnes molecular typing methods, and pointed out the importance of investigating P. acnes populations in acne vulgaris (38). The microbiological results presented here may be crucial for the elaboration of innovative therapies, such as probiotic treatments, as suggested previously (38). For instance, future topical treatments could restore the phylotype diversity, through re-introduction of P. acnes subgroup CC53. In addition, our data give a precise lineage description of the dominant P. acnes clones found in the context of severe acne, identifying for the first time the A1 SLST-type as the predominant SLST-type found in this disease. This information is currently the most precise genetic level of subgroup identification concerning P. acnes bacterium (24). It suggests the possibility of setting up a vaccine targeting A1 SLST-type, especially for children with a family history of severe acne, and with previous isotretinoin treatment in parents or brothers and sisters. Indeed, as acne occurs earlier and is more severe in patients with a positive family history, there is a need to investigate ways to prevent acne development, such as vaccination. Such treatments might prevent the irreversible scars associated with severe acne, which is a major problem in this disease.
This study was supported by a research grant from Galderma R&D - CUTIS (Sophia Antipolis). The authors would like to thank Dr Knol, Elodie Belliot, Nathalie Defossé and Julie Marraillac for technical support and assistance, and Aurélie Boisrobert for assistance with clinical sampling.
Conflicts of interest: SC, MS-J. and JMN have no conflicts of interest to declare. BD, AK and MAD declare a potential conflict of interest, as the study was funded by Galderma R&D - CUTIS (Sophia Antipolis, France). VB is an employee of Galderma R&D - CUTIS (Sophia Antipolis, France).


 Click to show fullsize
Click to show fullsize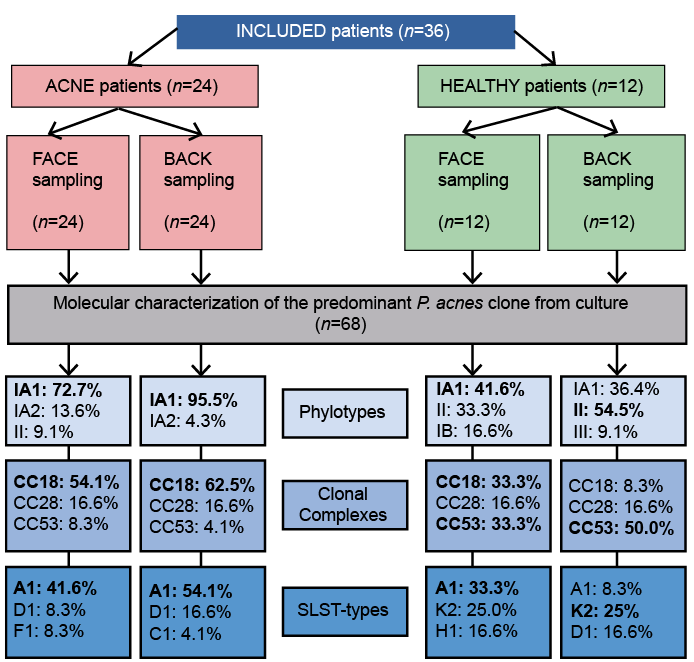 Click to show fullsize
Click to show fullsize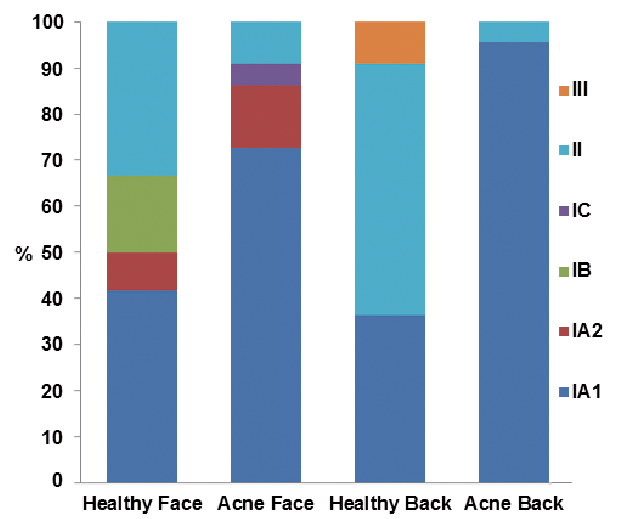 Click to show fullsize
Click to show fullsize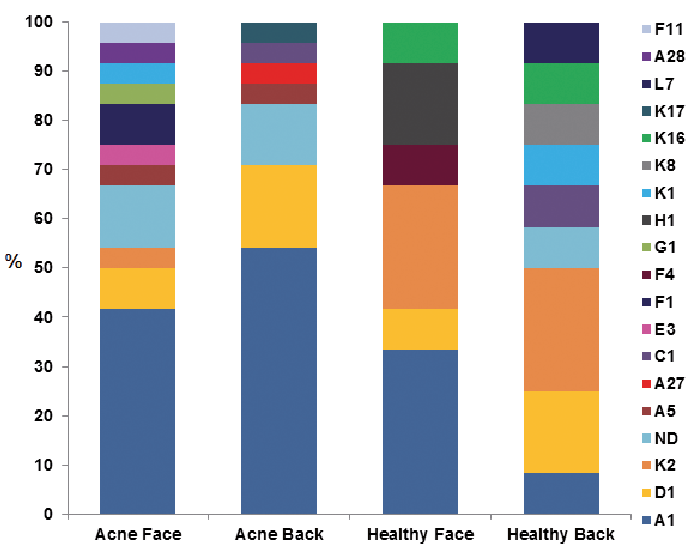 Click to show fullsize
Click to show fullsize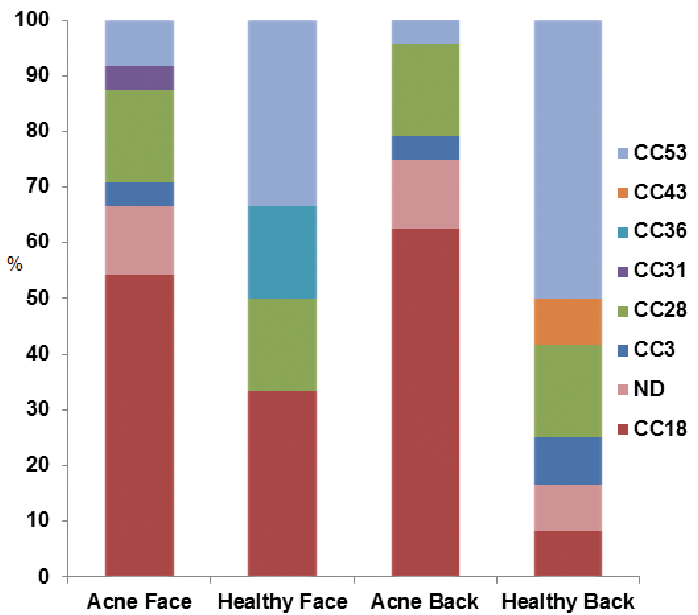 Click to show fullsize
Click to show fullsize