


1Dermatology and Venereology Unit, Department of Medicine Solna, Karolinska Institutet and Karolinska University Hospital, 2Pediatric Endocrinology Unit, Department of Woman and Child Health, Karolinska Institutet, Astrid Lindgren Children’s Hospital, 3Dermatology and Venereology Unit, Department of Medicine Huddinge, Karolinska Institutet and Karolinska University Hospital, 4Dermatology Clinic, Hudcentrum, Hagastaden, 5Dermatology Clinic, Stadions Läkarmottagning, Stockholm, 6Department of Clinical Chemistry, Department of Clinical and Experimental Medicine, Linköping University, Linköping, and 7Swedish Psoriasis Association Enskede, Stockholm, Sweden
Atopic dermatitis (AD) is a chronic, itchy, inflammatory skin disorder that may worsen due to stress and anxiety. Tachykinins have been suggested to be involved in the inflammation in AD, as well as pruritus. Aprepitant is a NK-1 receptor antagonist. This open randomized trial evaluated the effect of aprepitant added to topical treatment in adult patients with moderate–severe AD. The treatment group (n = 19) received 80 mg/day aprepitant for 7 days as a supplement to standardized topical treatment with a moderately strong steroid and a moisturizer. The control group (n = 20) received topical treatment alone. Patients were monitored for the extent of the disease (using SCORing of Atopic Dermatitis; SCORAD), pruritus, and scratching movements. In both the aprepitant-treated and the control groups there was a decrease in SCORAD, pruritus and scratching movements. How-ever, there was no significant additional improvement in any of these parameters in the aprepitant-treated group compared with the control group.
Key words: anxiety; atopic dermatitis; aprepitant; depression; neurokinin 1 receptor; pruritus; SCORAD; substance P.
Accepted Nov 24, 2017; Epub ahead of print Nov 28, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Louise Lönndahl, Dermatology and Venereology Unit, Department of Medicine Solna, Karolinska Institutet and Karolinska University Hospital, SE 171 76 Stockholm, Sweden. E-mail: louise.lonndahl@ki.se
Atopic dermatitis (AD) is a common, highly pruritic skin disease. For the majority of patients the symptoms decline after childhood, but, for some, AD continues into adulthood. AD per se is often associated with significant suffering for the patients as well as their families (1). The disease often has a remitting/flaring course, which may be exacerbated by social, environmental and biological triggers, such as psychological and physical stress (2).
The currently available standard treatment for AD is the use of moisturizers and topical steroids. If this treatment is not sufficiently effective, ultraviolet light (UV) and immunomodulator (e.g. cyclosporine, azathioprine, methotrexate) treatments are sometimes used. However, despite their higher potency, these treatments are not always effective. In addition, they carry the risk of severe side-effects, e.g. skin cancer, in the case of UV therapy, and infections and cancer in the case of immunomodulators.
As mentioned above, pruritus is a significant symptom of AD. Studies investigating the mechanisms of pruritus in humans (3) and mice (4) have reported substance P to be an important mediator of this symptom. Furthermore, substance P has been shown to induce wheal, flare and itching, when injected into human skin (3). This is thought to be partly due to the release of histamine from mast cells. Substance P is also considered a proinflammatory neuropeptide, and alterations in the number of substance P positive nerve fibres and levels of substance P have been reported in lesional compared with control skin of patients with AD (5).
The main receptor (R) of substance P is neurokinin (NK)-1R. A study in mice has suggested that a NK-1R antagonist (BIIF 1149 CL) could be effective in inhibiting scratching behaviour in mice (6). In humans, promising results have been shown for a NK-1R antagonist, aprepitant (EmendR, Merck Sharp & Dohme (Sweden) AB, Stockholm, Sweden) (which is registered in Sweden for the treatment of nausea during chemotherapy in cancer patients), when treating different pruritic skin disorders, including prurigo and atopic diathesis (7), and another report has shown a decrease in pruritus in patients with malignancies (metastatic solid tumours) and pruritus associated with their treatment (8).
The present study evaluated the effect of addition of aprepitant in the short-term treatment of adult patients with moderate-severe AD, in an open randomized trial, compared with topical treatment with a steroid and moisturizer alone. The primary outcome was treatment effect and the primary endpoint was the extent of the disease (measured using SCORing of Atopic Dermatitis; SCORAD), while the secondary outcome was pruritus. In addition, psychodemographic parameters, measured with an anxiety and depression score, were investigated.
We hypothesized that treatment with aprepitant might decrease pruritus and scratching in patients with AD, even over a short period of treatment. Aprepitant could then be a possible candidate for use in an alternative combination treatment that could modify the course of disease towards more rapid clinical improvement.
Forty-one adult patients (23 females and 18 males), aged between 20 and 50 years, were included in the study. The patients were recruited from dermatology clinics in the Stockholm area and examined at the Department of Dermatology, Karolinska University Hospital, Solna, Stockholm, Sweden. The patients had a moderate–severe (SCORAD > 20) AD, and diagnosis was determined according to the Williams criteria (9). Exclusion criteria were other concomitant diseases or medications (except for contraceptives), skin type 5–6 according to Fitzpatrick, skin infections, pregnancy and breast-feeding.
The washout period for prior systemic treatment was 2 months.
The study was an open randomized trial with an active treatment period of 7 days. All participants received oral and written information about the study and voluntarily signed an informed consent. The protocol was approved by the local ethics committee and by the Medical Products Agency. The study was conducted during the period October 2013 to March 2015, and not during the summer.
Randomization was performed using a randomization list with no stratification. The nurses who evaluated SCORAD in the patients were blinded as to which treatment group the patients belonged. The sex distribution was 12:7 (M:F) in the treatment group and 4:16 in the control group. The mean ± standard deviation (SD) age was 30.8 ± 8.4 years in the treatment group and 29.3 ± 9.2 years in the control group (Table I).
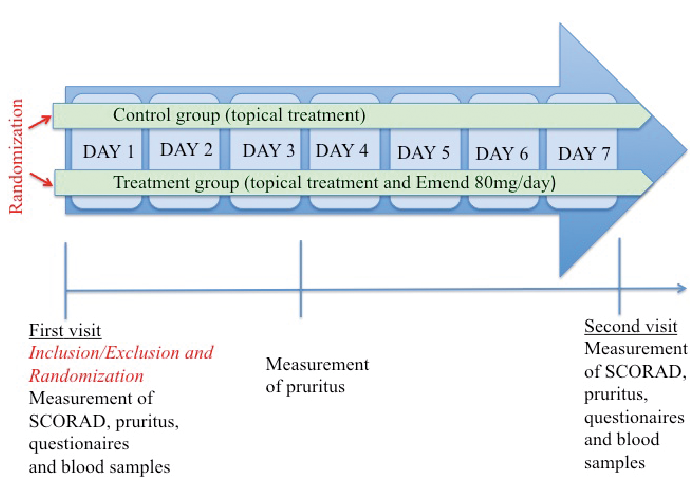
Fig. 1. Study design. SCORAD: SCORing of Atopic Dermatitis.
The patients received 80 mg/day of aprepitant orally for 7 days in addition to topical treatment with a moderately strong steroid cream (hydrocortisone butyrate; Locoid®, LEO Pharma AB, Malmö, Sweden) and a moisturizer. The control group received only the topical treatment. The patients were monitored regarding the extent of the disease (SCORAD), their pruritus, as well as anxiety and depressive scores (see below). The experimental design is shown in Fig. 1.
Table I. Clinical characteristics of patients in the treatment and control groups, who completed the study
Safety was assessed by recording adverse events (AE) at the second visit. The patients could also contact the clinic at any time during the treatment period if they observed any suspected side-effects.
The extent of the disease was assessed using SCORAD (10). Both objective and subjective SCORAD were included.
To achieve a dual assessment of pruritus, both a visual analogue scale (VAS), for subjective pruritus, and scratching movement registration were used. The degree of subjective pruritus was assessed using a VAS in which patients rated their own pruritus, twice a day, on a 0–10 scale (0 = no pruritus, 10 = worst imaginable pruritus). The mean of the 2 assessments daily were then calculated. In addition, patients registered the number of scratching movements per day using a manual counter (TAMACO 20-1681, Clas Ohlson, Insjön, Sweden) (11). The patients were asked to register either a scratching movement or, in the case of several movements, an episode.
Depression and anxiety scores were determined using enquiries (Montgomery Åsberg Depression Rating Scale (MADRS-S) (12) and Hospital Anxiety and Depressive scale (HAD) (13)), respectively.
General blood samples were taken before and after treatment to monitor possible side-effects (complete blood account, leukocyte differential count, liver enzymes, and creatinine). Plasma levels of total IgE were also determined. In addition, the level of substance P was determined and, for that purpose, serum samples were prepared by centrifugation at +5oC as well as in the presence of aprotinin (Sigma-Aldrich, Stockholm, Sweden). The samples were subsequently analysed using a radio-immunoassay technique, as follows. Samples were purified using reverse-phase C18 cartridges (Sep Pak, Waters, Milford, MA, USA) and the concentrations of substance P were analysed using antiserum SP2 (14), which reacts with substance P and substance P sulphoxide, but not with other tachykinins. (Tyr8)-substance P was labelled with 125I using the chloramine-T method and purified using reverse-phase gradient high performance liquid chromatography. Intra- and inter-assay coefficients of variations were 7% and 11%, respectively.
Statistical analysis was performed for all patients included in the study (intention to treat; IIT), as well as on values for patients who would continue in the study as planned by protocol (per protocol; PP). Lost values were included in the IIT analysis by “last value carried forward”. Statistical comparisons in order to test differences between 2 independent groups were made using the Student’s t-test for uncorrelated means, after validation for normal distribution. In the case of a normal distribution, correlated means were analysed using paired t-test. The difference in IgE within the groups was tested by a non-parametric method, Wilcoxon signed rank test, due to large SDs.
The number of patients in the study was calculated to provide 80% power to detect a difference in SCORAD improvement of 3 points at the 5% level of significance (2-sided). All analyses were carried out using the Prism system or SAS statistical software (SAS 9.4). The 5% level of significance was considered and, in the case of a statistically significant result, the probability value (p-value) is given.
In total, all but 2 patients in the treatment group completed the study, according to protocol. Those 2 patients interrupted study treatment due to adverse events. The results presented below were obtained from per protocol analysis, based on the 39 patients who completed the study. ITT analysis of 41 patients was also performed, but no statistical difference was found. Clinical characteristics of the patients are shown in Table I.
Furthermore, an interim analysis was performed after the inclusion of 31 patients. This analysis showed that, at 3 days, there was a tendency (p = 0.07) for a VAS value reduction in the group treated by aprepitant, compared with the control group.
The mean ± SD extent of AD, measured by OSCORAD, decreased in both the aprepitant-treated group (from 40.5 ± 12.0 to 32.0 ± 11.2; p < 0.01) and in the control group (from 37.0 ± 11.3 to 26.7 ± 14.7; p < 0.001). The mean ± SD subjective SCORAD (S-SCORAD) also showed a decrease in the treatment group (from 49.0 ± 14.1 to 38.1 ± 12.6; p < 0.001) and in the control group (from 47.7 ± 13.7 to 33.0 ± 18.9; ns (p = 0.09). There were no significant differences between the groups. The results are summarized in Table II.
Table II. Results in treatment group and control group, respectively
The mean ± SD VAS in the treatment group decreased from 5.5 ± 2.1 at inclusion to 3.8 ± 2.2 at the end of treatment (Day 7) (p < 0.05) and in the control group from 6.7 ± 2.2 to 4.1 ± 3.0 (p = 0.001). Scratching movements in the treatment group decreased from 77.3 ± 97.9 to 48.3 ± 62.6 (p < 0.05), and in the control group there was a tendency to a decrease from 65.0 ± 100.9 to 34.7 ± 45.0 (p = 0.07). There were no significant differences between the groups at any of the time-points (Days 1, 2, 3, 5 or 7).
In both the treatment group and the control group there was a decrease (p < 0.05) in mean ± SD MADRS-S score from 5.6 ± 4.9 to 4.0 ± 5.3 and from 9.3 ± 8.9 to 6.5 ± 5.9, respectively. In addition, a decrease in mean ± SD HAD depression score was seen in the control group, from 3.8 ± 2.7 to 2.4 ± 2.3 (p < 0.01). The decrease in HAD depression score was not significant in the treatment group; 1.9 ± 2.1 to 1.8 ± 2.4. There was a decrease in HAD anxiety score in the control group, from 6.6 ± 4.8 to 4.8 ± 3.7 (p < 0.05), but no difference was seen in the treatment group, where HAD anxiety score was 3.4 ± 4.1 before treatment and 3.5 ± 3.2 after treatment.
In the treatment group the mean ± SD value of total IgE before treatment was 903.7 ± 1,391 kE/l and after treatment 937.9 ± 1,403 kE/l. In the control group the mean value before treatment was 876.5 ± 1,934 kE/l and after treatment 821.1 ± 1,754 kE/l.
The mean values for serum substance P in the treatment group were 98.7 ± 54.4 pmol/g before and 97.6 ± 50.3 pmol/g after treat-ment. The values for serum substance P in the control group were 105.6 ± 46.5 pmol/g before and 91.0 ± 32.7 pmol/g after treatment.
Statistical analysis of the substance P measurements did not show any correlation between the level of substance P and the extent of disease (SCORAD) or pruritus (VAS) before treatment. Patients with high serum substance P did not respond better to aprepitant, measured as a correlation between serum substance P and the level of disease activity (SCORAD or VAS).
Thirteen out of the 21 aprepitant-treated patients reported adverse events (headache, fatigue, dizziness, elevated liver enzymes, palpitations, dyspnoea, altered ability to react, obstipation, stomach-ache, periocular dermatitis, and erectile dysfunction). All AEs were considered mild to moderate. All AEs were transient, except for one case of elevated liver enzymes that remained above normal at the last follow-up visit.
The 2 male patients in the treatment group who interrupted their participation in the study, specifically experienced transient side-effects, such as dizziness, impotence, headache (1 case) and lack of reactivity, dyspnoea and palpitations (the second case).
This study evaluated the effects of using aprepitant as an adjunct to standard topical treatment alone. The primary endpoint was extent of disease, and secondary endpoints were pruritus (using VAS and scratching movements) and psychodemographic measurements, depression and anxiety. We hypothesized that aprepitant at a dose of 80 mg/day would contribute to a decrease in pruritus and inflammation, and thereby might change the course of disease, even for this short time-period.
The results show a significant decrease in the extent of disease and pruritus in both the treatment and the control group. However, no additional effect of aprepitant was observed at the study dose and time-period. The setting of this clinical trial supported the patients in complying with all standards of care study procedures and obtaining significant relief of the disease symptoms.
No significant decrease in pruritus was found in the aprepitant-treated group compared with the control group. However, the patients with AD recruited to this study generally did not have worse than moderate pruritus, which may have had an impact on the results. It is also possible that pharmacokinetics and possible induction of a degrading system in the liver may explain the lack of response, especially since interim analysis showed a tendency to a significantly lowered pruritus on Day 3 in the treatment group compared with the control group.
The standard dose for the approved indication for chemotherapy-induced nausea (the approved indication in Sweden today) is 150 mg the first day, and 80 mg/day on the 2 following days. The dose chosen for our study was 80 mg/day, based on an earlier study of pruritus by Ständer et al. (7). Regarding the dose of aprepitant, it has been suggested that, for treatment of depression, near complete receptor occupancy for the NK-1R antagonist is needed, and that an occupancy of below 90% may be ineffective (15). In a study of co-morbid alcohol dependence and post-traumatic stress disorder a dosage of 125 mg/day for 4 weeks was used, based on positron emission tomography studies reporting > 90% central receptor occupancy at this dose (16). However, no effect was found. In addition, the influence of polymorphism of the tachykinin receptor (TacR) -1 gene may be of importance (15).
A further possible explanation for the results of the current study is that the disease and the mechanisms involved in both inflammation and pruritus are more complex, and not substantially dependent on substance P as a principal mediator and communicator via NK-1R. Earlier studies in humans showed no correlation between plasma levels of substance P and SCORAD (5, 17, 18). Animal studies have had contradictory results regarding the pruritic role of substance P and NK-1R. A recent study in mice showed no effect of aprepitant on scratching behaviour (19), whereas an earlier study (6) using a different NK-1R antagonist in a mouse strain showed that scratching behaviour could be inhibited. In a study on NC/Nga mice, treatment with aprepitant resulted in decreased levels of IgE as well as a decreased density of substance P nerve fibres, although there was no effect on clinical signs (20).
In the current study there were different sex distributions in the 2 groups, with a markedly higher proportion of men than women in the treatment group and vice versa in the control group. Thus, it cannot be excluded that aprepitant exerts sex-specific effects. In the study by Ständer et al. (7) a greater reduction in pruritus was noted in male patients, although no significant sex difference could be found. They suggested that aprepitant may be more effective in younger male patients, which would have given an optimal effect in our study, which had a male predominance in the treatment group. However, we did not observe such effects.
Both study groups reported a highly significant improvement in extent of AD and pruritus, which we interpreted as due to a high level of compliance with treatment. We used a moderately strong steroid cream and a moisturizer, and still measured a significant improvement in both the extent of disease as well as the pruritus. It should also be noted that the scratching movements showed a high level of deviation from the mean, leading to difficulties in comparing the treatment and control groups.
In conclusion, no additive effect was found due to short-term treatment with aprepitant for AD, compared with standardized topical treatment alone. It is possible that short-term treatment with aprepitant could be beneficial for patients with a higher level of pruritus, to decrease the pruritus and break the itch-scratch cycle. Further studies into a role for aprepitant in patients with severely itchy AD and resistance to topical treatment, are warranted.
This study was supported by a grant from Hudfonden. The assistance of RN Papely Kassiri and RN Kirsti Ajax is gratefully acknowledged. The authors also acknowledge Dr Anna Aleskog at MSD Sweden for valuable discussion of doses of aprepitant. RN Christina Åkerstedt and RN Laurence Gunnberg Querat, St. Erik Eye Hospital are gratefully acknowledged for monitoring source data.
Conflict of interest: During collection of the data M.H. was employed at Pfizer.


 Click to show fullsize
Click to show fullsize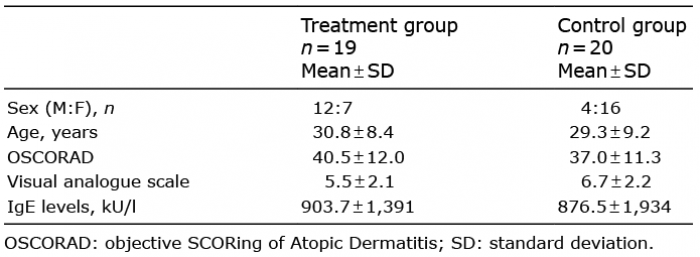 Click to show fullsize
Click to show fullsize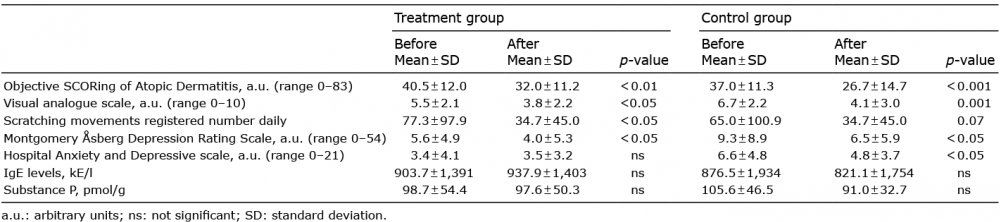 Click to show fullsize
Click to show fullsize