


1Department of Dermatology and Allergy Centre, Odense University Hospital, 2Department of Clinical Microbiology, Odense University Hospital, University of Southern Denmark, 3Virology Surveillance and Research Section, Department of Microbiological Diagnostics and Virology, Statens Serum Institut, Copenhagen, Denmark and University of Southern Denmark, Clinical Institute, and Center for Global Health, and 4Department of Clinical Pathology, Odense University Hospital, Odense, Denmark
Since 2008, outbreaks of atypical hand, foot, and mouth disease (HFMD) in children and adults have been reported worldwide. The majority of these outbreaks are caused by a new lineage of Coxsackie virus A6 (CV-A6) presenting a more severe clinical phenotype than the classical childhood HFMD caused by CV-A16. Between June 2014 and January 2016, 23 cases of atypical HFMD disease presented at a Dermatology Department at a regional University Hospital in Denmark. Patients were referred by general practitioners and dermatologists with a variety of clinical diagnoses, including eczema herpeticum, vasculitis, syphilis, dermatophytid, erythema multiforme and Stevens-Johnson syndrome. Three adults and 3 children required hospitalization due to extensive skin involvement and fever. All reported patients had laboratory-confirmed enterovirus infection. This study demonstrated an upsurge in atypical HFMD caused by CV-A6 in the Region of Southern Denmark and that atypical HFMD can be difficult to diagnose clinically as it may mimic other severe skin diseases.
Key words: atypical hand, foot, and mouth disease; Coxsackievirus A6; diagnostic mimicker.
Accepted Nov 24, 2017; Epub ahead of print Nov 28, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Hans-Henrik Horsten, Department of Dermatology and Allergy Centre, Odense University Hospital, DK-5000 Odense C, Denmark. E-mail: hans-henrik.horsten@rsyd.dk
Hand, foot, and mouth disease (HFMD) is a common viral illness generally affecting children under 7 years of age (1). Classical HFMD is a self-limiting condition presenting with oropharyngeal blisters, papular vesicles on the palms and soles, and sometimes fever. Patients will rarely be referred to the hospital, as symptoms are mild and complications, such as encephalitis and myocarditis, are rare in Europe (2–4). Seasonal outbreaks occur, with incident peaks during the summer and early autumn. The major causative agents have been Coxsackievirus A16 (CV-A16) and enterovirus (EV)-A71 within the species EV-A, members of the virus family Picornaviridae in the genus Enterovirus (5).
Since 2008 outbreaks of atypical HFMD caused by CV-A6 have been reported worldwide, mostly during the winter in temperate climates (6, 7). An increasing number of reports indicate that this new lineage of CV-A6 is more virulent, causing a widespread vesicular skin eruption in children as well as adults (8, 9). In atopic children, a clinical presentation resembling eczema herpeticum has been described and termed eczema coxsackium (10, 11).
The histopathological findings are mainly in the epithelium and consist of widespread keratinocyte necrosis and spongiosis, often with formation of vesicles. Neutrophilic exocytosis and reticular degeneration of the basal cell layer also occur. In the papillary dermis there is often massive oedema and a variable inflammatory infiltrate dominated by lymphocytes. As opposed to common findings in other viral diseases, there are no multinucleate cells, inclusion bodies or koilocytes (12, 13).
The aim of this study is to present the clinical and paraclinical features of atypical HFMD, in order to inform physicians about the new phenotype. Intrafamilial cases are also reported.
The Department of Dermatology and Allergy Centre, Odense University Hospital see patients referred from primary care physicians, practicing dermatologists and other hospital departments in the Region of Southern Denmark, which covers a population of ~1.2 million people. Based on a clinical picture suspicious of atypical HFMD, specimens were taken as vesicle fluid swabs, oropharyngeal swabs, and/or stool samples. The initial testing for EV was performed at the local Department of Microbiology using an in-house real-time PCR method. EV-positive samples were sent to the National World Health Organization (WHO) Reference Center for Polio at Statens Serum Institut for further characterization. Here, EV-RNA was subjected to a multiplex 1-step real-time assay with semi-nested PCR, and subsequently sequenced using Sanger technique targeting the region encoding the VP1 and VP2 genes, whose sequence corresponds with antigenic serotype (14). In addition, all EV-RNA positive samples were routinely cultivated in 3 cell lines established as part of the poliovirus surveillance programme. For samples that might not have been characterized successfully during the first attempts, the typing procedure was repeated on cultivated material.
From June 2014 until January 2016, a total of 26 patients with a clinical presentation suggesting possible atypical HFMD were tested for EV infection. Of these patients, 23 (88%) tested EV-positive, including 15 adults and 8 children. Thirteen patients tested positive for CV-A6, while the others could not be subtyped. A total of 3 adult patients had negative viral testing. Patients were referred to the department with the following diagnoses: erythema multiforme, Stevens-Johnson syndrome, eczema herpeticum, syphilis, dermatophytid, vasculitis, psoriasis, impetigo and atopic dermatitis. HFMD was suggested as a clinical diagnosis in the referral notes for only one patient. Clinical presentations and descriptions of adults and children are given in Fig. 1 and Table I. All patients were considered immunocompetent. Two children (#2, #5) and 2 adults (#12, #19) had a history of atopic dermatitis, but none had active dermatitis at the initial evaluation. One adult (#13) had a history of psoriasis. No other patients had a previous history of skin disease. Two adults (#22, #23) had artificial heart valves. One child (#1) developed fever and a vesicular eruption on the trunk during the last day of a 1-week trip to Turkey, while no other patients had a travel history or other significant exposures.
Fig. 1. Examples of skin lesions. Erythematous, papulovesicular eruption on the (A) face, (D) back, (B, C) upper and (E, F) lower limbs of an adult, and (G, H) trunk and leg of a child. (I) Onychomadesis in a child several weeks after remission of skin eruption.
Table I. Clinical presentations and descriptions of 8 children and 15 adults with atypical hand, foot, and mouth disease (HFMD) and confirmed enterovirus infection
The median age of the adult patients was 33 years (range 28–67 years), and 80% (12/15) presented with fever and oral mucosal symptoms. All adults developed a vesicular eruption and presented skin lesions on the dorsal and palmar surfaces of the hands; 87% (13/15) of adults had facial involvement and 27% (4/15) had lesions on the soles with itching and pain. Seven adult patients sought emergency care and 3 were hospitalized. Of the 8 children included, with a median age of 2 years (range 1–8 years), all presented with fever and 75% (6/8) presented with skin lesions on the hands and feet. Three children were hospitalized with a suspicion of eczema herpeticum or impetigo. Among all included patients, 2 were treated with acyclovir, 4 received systemic antibiotics and 2 received systemic corticosteroids. However, none of these treatments was effective.
Household transmission was documented in 3 families, demonstrating child-to-adult transmission and child-to-child transmission. In 2 of these families, children were only mildly affected compared with their parents, who presented with a severe eruption of atypical HFMD. Among adults, 47% (7/15) reported recent contact with a child who had symptoms compatible with HFMD.
The first sporadic cases of atypical HFMD in our department were seen during summer 2014 and 2015. Subsequently most of our patients were clustered between September 2015 and January 2016 (Fig. 2). No systematic follow-up was performed, but 2 children and no adults were reported to have delayed nail shedding.
Fig. 2. Seasonal outbreak of atypical hand, food and mouth disease in 23 Danish patients.
EV was identified in vesicle fluid samples (12/12), oropharyngeal swabs (12/16) and stool samples (11/13). In 13 individual cases virus subtyping was performed, and all identified CV-A6. In the other patients insufficient sample material prevented further subtyping. Details and timing of biological samples are listed in Table II.
Table II. Specimen collection (obtained in days after onset of symptoms) and results of diagnostic testing for enterovirus in 23 Danish patients presenting with atypical hand, foot, and mouth disease in the period 2014 to 2016
Skin biopsies were obtained from 1 child and 4 adults. In 3 of the biopsies, the dominating features were keratinocyte necrosis and foci with confluent necrosis interpreted as erythema multiforme. There was little spongiosis and only sparse intraepithelial inflammation, while oedema and lymphocytic inflammation were found in the papillary dermis. In one patient the epidermis was inconspicuous and the only change was a sparse perivascular infiltrate of lymphocytes. In the biopsy from the child, the epithelium did not have keratinocyte necrosis, but slight degenerative changes were detected. In the papillary dermis, oedema and lymphocytic inflammation were seen. The histopathological conclusion was chronic inflammatory changes with a possible viral aetiology.
This report describes the first outbreak of atypical HFMD caused by CV-A6 in our region of Denmark. A former case report of 2 adults with scalp affection was published in 2012 (15), and recently a childhood case has also been published by our group (11). In recent years CV-A6 has emerged as 1 of the major causes of epidemic HFMD worldwide. The first reported CV-A6 associated outbreak was in Finland in 2008 (6, 16), with subsequent outbreaks in Singapore (17), France (18), China (19, 20), US (21), Thailand (22), Cuba (23), New Zealand (24) and, most recently, the UK in 2014 (25).
Mostly children have been affected during CV-A6 outbreaks. In this study, surprisingly we saw more adult patients than affected children, and also several cases of likely intra-familial transmission. EV is considered highly contagious, and this is supported by the widespread household transmission of CV-A6. Counselling regarding hygiene precautions and information about the risk of infection through contact with fluid in vesicles, saliva, and prolonged stool shedding should be given to prevent disease transmission. In this study, one patient was positive for EV approximately 6 months after onset of symptoms. However, subtyping for CV-A6 was not possible.
All adults had a vesicular eruption involving the palms and dorsal hands, which differs from the typical HFMD, in which the palms are usually favoured. The acral hand and feet eruptions were highly symptomatic and led some adult patients to seek medical assistance in emergency rooms. The palmar and plantar eruption in 2 adult patients led their referring dermatologist to suggest syphilis as a tentative diagnosis. Several adult patients also displayed facial involvement with widespread vesicles, including the forehead. This was in contrast to children, who mostly had vesicles in a distinct perioral distribution, in accordance with earlier reports (10). Two children aged 1.5 years presented a distinct clinical picture of eczema coxsackium.
The diagnostic methods for determining the presence of EV included vesicle fluid swabs, oropharyngeal swabs and stool samples. Oropharyngeal swabs were positive from day 1 up to 15 days after the onset of symptoms. Stool samples were positive from day 1 to day 180, which exceeds the expected period of faecal excretion of up to 3 months (26, 27).
Skin biopsies were taken from 5 patients due to the atypical clinical picture. Only a few published cases of atypical HFMD have been accompanied by histopathology. One of the important differences between classical HFMD and atypical HFMD is extensive necrosis of the epidermis. The necrotic keratinocytes in CV-A6 associated HFMD may mimic Stevens-Johnson syndrome, erythema multiforme and toxic epidermal necrolysis in the microscope, as was the case in 3 of our 5 biopsies. This can be a possible pitfall, especially when the clinical picture was atypical and could imitate these disorders. A former histopathological study of 3 cases pointed out that intraepidermal vesiculation with a predominantly neutrophil-rich infiltrate was a characteristic feature, as well as a specific involvement of the upper stratum spinosum and stratum granulosum, with relative sparing of the stratum corneum (13). Two of our biopsies were without specific changes, and additional biopsies might be necessary in order to demonstrate the typical histological changes. It has also been reported that histopathology can imitate a severe cutaneous drug reaction (28).
In the presented cases, differential diagnoses to atypical HFMD were ruled out, based on the clinical features, histopathology and PCR for herpes simplex and varicella zoster virus.
The limitation of our study is that it is a case series from a single dermatological department in a hospital setting. The range of referral diagnoses from dermatologists included eczema herpeticum, vasculitis, Stevens-Johnson syndrome and syphilis, highlighting the mimicking of a broad variety of clinical presentations. It is important that clinicians are informed about the atypical presentation of CV-A6-associated HFMD. A correct diagnosis is critical to avoid unnecessary therapy and to provide the patient with accurate prognostic expectations and advice on precautions to limit spread of the disease.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize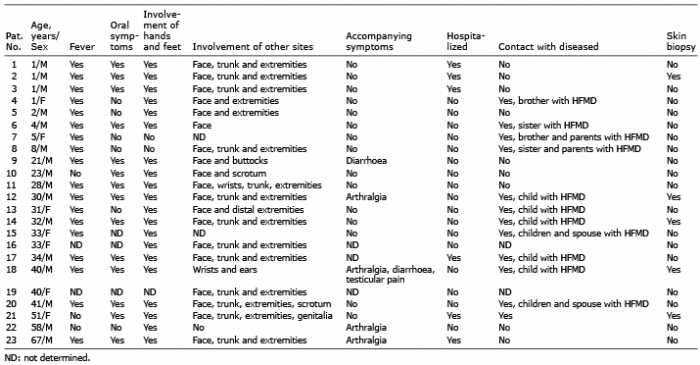 Click to show fullsize
Click to show fullsize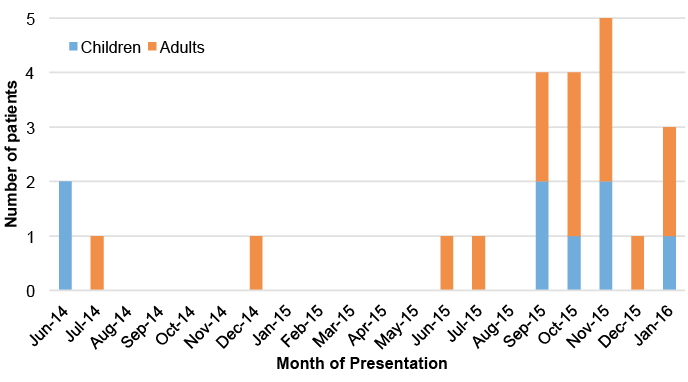 Click to show fullsize
Click to show fullsize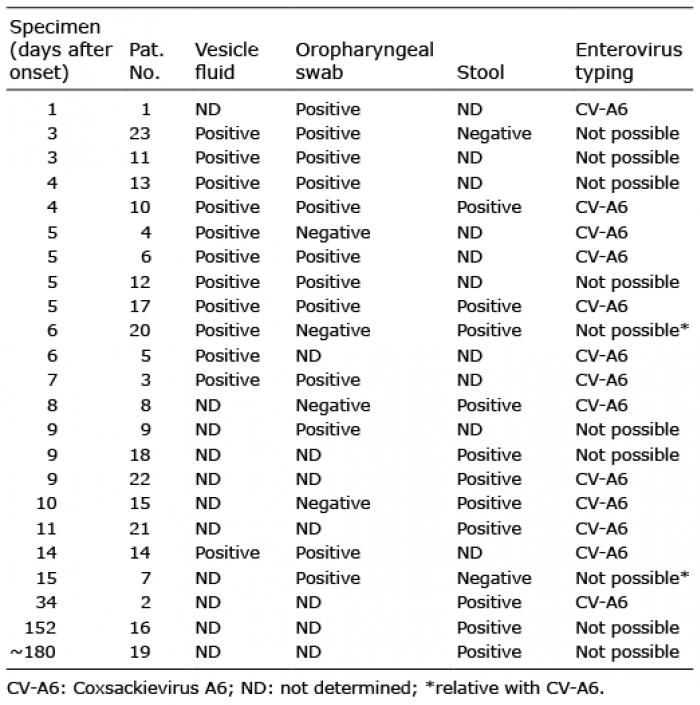 Click to show fullsize
Click to show fullsize