


1Department of Dermatology Seoul St Mary’s Hospital, College of Medicine, The Catholic University of Korea, 2Department of Biostatistics, College of Medicine, The Catholic University of Korea, 222, Banpo-daero, Seocho-gu, Seoul, 06591, and 3Department of Dermatology, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea. *E-mail: ygpark@catholic.ac.kr, lyb80@catholic.ac.kr
#These authors contributed equally to this work.
Accepted Nov 24, 2017; Epub ahead of print Nov 28, 2017
Actinic keratosis (AK) is characterized by a proliferation of atypical keratinocytes in the epidermis. AK occurs mainly in middle-aged and older, fair-skinned, subjects, and is related to chronic exposure to ultraviolet light (UV) (1). Non-melanoma skin cancers (NMSCs) (i.e. basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)) are the most common type of skin cancers. The rate of progression from AK to SCC is variably reported as 0.25–20% per year (2, 3). Few studies have examined the incidence of NMSCs and malignant melanoma (MM) among Asian patients with an initial diagnosis of AK, as assessed through long-term follow-up. This study analysed the incidence of AK and the risk of skin cancer in patients with AK based on data obtained from the National Health Insurance System (NHIS) in South Korea.
This study utilized nationwide data from January 2006 through December 2015. Data were analysed from patients over 40 years of age who visited clinics or hospitals with a diagnostic code (International Classification of Diseases 10th revision; ICD-10) of AK (L570) more than once in a given year. A detailed description of the data source and methodology of this retrospective study is given in Appendix SI.
The total number of NHIS registrations involving individuals > 40 years of age in the period 2006 to 2015 was 229 millions. The corresponding number of patients with AK was 77,975 (Table SI). The incidence rate increased from 17.94 to 53.99 per 100,000 person-years between 2006 and 2015. After adjusting for age, the incidence also increased strikingly, from 19.57 to 52.86 per 100,000 person-years, between 2006 and 2015. We also analysed AK patients aged 40 years or older in 2015 (Table SII). The incidence rates of AK per 10,000 person-years increased consistently with age (Table SII and Fig. S1). It is notable that the incidence rate increased sharply for persons in their 70s (Fig. S1). In 2015, the prevalence of AK per 10,000 people was 1.95, 4.00, 9.43, 21.90, and 31.81, for persons aged in their 40s, 50s, 60s, 70s, and 80s, respectively.
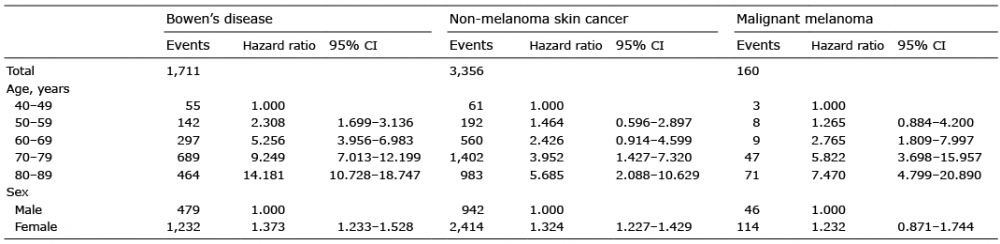
Patients diagnosed with AK between 2006 and 2014 were followed up until 2015. Our analysis included 63,935 subjects who were diagnosed with AK (Table I). Of these AK patients, follow-up revealed 464 cases that had developed in situ SCC (Bowens disease; BD) 983 cases with NMSC, and 71 cases with MM in their 80s. The hazard ratio (HR) for individuals developing skin cancer was evaluated in patients with AK, with the reference age range of 40–49 years. The HR for BD, NMSC, and MM was 9.25, 3.95, and 5.82, respectively, in patients with AK between the ages of 70 and 79 years. In patients with AK aged 80 years or older, the HR for BD, NMSC, and MM was 14.18, 5.69, and 7.47, respectively. In addition, the HR for subjects who develop skin cancer was higher in women than in men.
Table I. Incidence of Bowen’s disease, non-melanoma skin cancer, and malignant melanoma in patients with actinic keratosis
AK is a common potentially premalignant disease, and occurs mostly on areas of the skin with high levels of exposure to the sun. Age, male sex, skin type, and cumulative exposure to the sun are considered independent risk factors for AK (4). In this large study, the incidence of AK increased from 19.57 in 2006 to 52.86 per 100,000 person-years in 2015. The present study showed that the incidence of AK in South Koreans was much lower than that of the Western population (5, 6). This difference is thought to be due to differences in skin types, or geographical areas, ethnicity or lifestyle. Consistent with previous reports, this study showed that the incidence and prevalence of AK increased notably with age (7–9).
AK, BD and SCC have been shown to share a common pathomechanism, which includes a mutation in the p53 gene (10). Previous reports have shown that 65–72% of cutaneous SCCs arise from AKs in Caucasians (11, 12). In a recent systematic review, progression rates of AK to SCC were shown to be 0~0.075% per lesion-year (3). BCC developed in 36% of lesions diagnosed clinically as AKs in the USA (12). Foote et al. (13) reported that the estimated incidence of BCC and SCC in adults with AK in the USA was 0.041 and 0.032 per person-year, respectively. In a systematic meta-analysis of observational studies of melanoma, the pooled estimated relative risk of actinic damage indicator in MM was 2.02 (95% CI: 1.24–3.29) (14). The authors of that study suggested that a shared internal pathway may explain the association between AK and the increased risk of melanoma. Chen et al. (15) reported that there was a 6-fold increase in risk of NMSC or MM in people with AK compared with people without AK in the USA. They suggested that older white males with a history of AK represented a group at high risk of developing skin cancer (15). In the current study involving an Asian population, the risk of skin cancer was higher in women with AK than in men with AK. In addition, the risk of BD, NMSC and MM increased significantly in the patients with AK in their 70s or 80s compared with the patients with AK in their 40s.
A limitation of this study is that it was not known whether skin cancer occurred at the same location where the AK developed initially. There was no analysis of the site of the lesions, the number of lesions, or AK subtype. Despite these limitations, our results suggest that analysis of data gathered from national surveys may be useful for investigating the incidence of AK and the risk of developing malignancy associated with AK. Since the incidence of AK and the risk of skin cancers in patients with AK increases with old age, early diagnosis and immediate treatment of AK is important.
Funding sources: This study was approved by the ethics committee of Seoul St Mary’s Hospital, The Catholic University of Korea (KC17ZESI0126) and was supported by a National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (numbers NRF-2015R1C1A2A01054767 and 2016R1C1B1008288).


 Click to show fullsize
Click to show fullsize